Radiologic-Pathologic Correlation of Unusual Lingual Masses:Part II: Benign and Malignant Tumors
- Affiliations
-
- 1Seoul Natl Univ Hosp,Dept Diagnost Radiol Chongno Gu,28 Yongon Dong, Seoul 110744, South Korea.
- KMID: 754122
- DOI: http://doi.org/10.3348/kjr.2001.2.1.42
Abstract
- Because the tongue is superficially located and the initial manifestation of most diseases occurring there is mucosal change, lingual lesionscan be easily accessed and diagnosed without imaging analysis. Some lingual neoplasms, however, may manifest as a submucosal bulge and be located in a deep portion of the tongue, such as its base; their true characteristics and extent may be rec-ognized only on cross-sectional images such as those obtained by CT or MRI. Some uncommon tongue neoplasms may have characteristic radiologic fea-tures, thus permitting quite specific radiologic diagnosis. Lipomas typically manifest at both CT and MR imaging as homogeneous nonenhancing lesions. Relative to subcutaneous fat they are isoattenuating on CT images, and all MR sequences show them as isointense. Due to the paramagnetic properties of melanin, metastases from melanotic melanoma usually demonstrate high signal intensity on T1-weighted MR images and low signal intensity on T2-weighted images. Although the radiologic findings for other submucosal neoplasms are nonspecific, CT and MR imaging can play an important role in the diagnostic work-up of these unusual tumors. Delineation of the extent of the tumor, and recognition and understanding of the spectrum of imaging and the pathologic features of these lesions, often help narrow the differential diagnosis.
Keyword
MeSH Terms
Figure
-

Fig. 1 Lipoma in a 40-year-old man with a non-tender, soft mass at the left dorsum of the tongue. A. T1-weighted axial image shows an ovoid mass, its high signal intensity similar to that of subcutaneous fat, at the left anterior aspect of the tongue (arrow). B. T2-weighted axial image also shows that the high signal intensity of this mass is similar to that of subcutaneous fat (arrow). C. Photomicrograph (original magnification ×100; H & E staining) shows that the lipoma is composed of mature adipocytes (*). The mass is well demarcated by a fibrous pseudocapsule (arrow) and separated from lingual muscle (not shown). An easily detachable yellow-to-white soft tissue mass was excised.
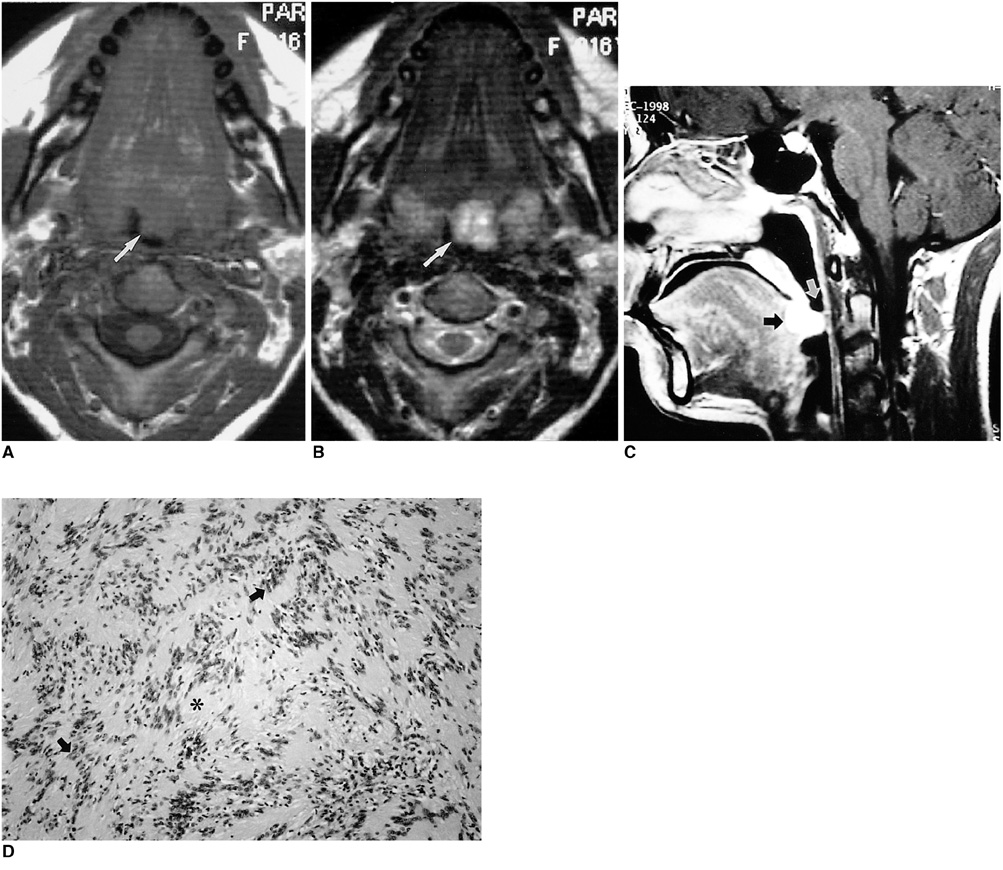
Fig. 2 Schwannoma in a 16-year-old girl with swallowing difficulty. A. T1-weighted axial image shows a well-defined, homogeneous mass (arrow), isointense to surrounding muscle, at the base of the tongue and encroaching on the airway. B. T2-weighted axial image shows a mass with heterogeneous high signal intensity (arrow). C. Enhanced T1-weighted sagittal image shows that the mass is located at the posterior one-third of the tongue, which corresponds to the region of the foramen cecum (black arrow). This mass significantly encroaches on the airway (white arrow). D. Photomicrograph (original magnification ×40; H & E staining) shows spindle cells with some whirling and pallisading of their nuclei (arrows). The cells resemble Verocay bodies and enclose a space nearly devoid of nuclei (*). There is no evidence of malignancy.
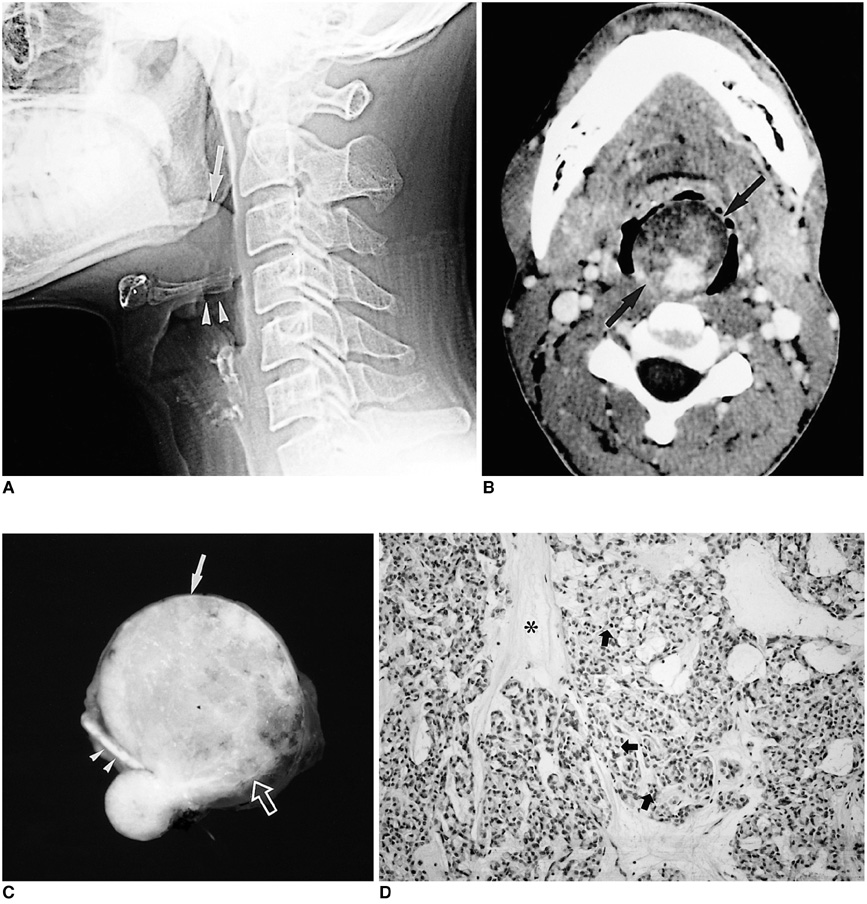
Fig. 3 Myoepithelioma in a 35-year-old man with severe dyspnea and difficulty in swallowing. A. Lateral view of plain cervical spine shows a lobulating, well-defined soft tissue density mass (arrow) at the base of the tongue, resting against the epiglottis (arrowheads) and encroaching on the airway. B. Contrast-enhanced axial CT scan shows a well-defined mass with heterogeneous attenuation (arrows) at the base of the tongue. Since the anterior portion of this mass has low attenuation similar to that of subcutaneous fat, initial differential diagnosis included benign mature teratoma and benign minor salivary gland tumor such as pleomorphic adenoma. C. Photograph of a cut section of gross specimen shows a well-demarcated yellowish mass (arrow) arising from the base of the tongue (open arrow). A lower small daughter nodule is covered by intact lingual mucosa. Note the intervening epiglottis (arrowheads) between the main mass and the nodule. D. Photomicrograph (original magnification ×100; H & E staining) shows plasmacytoid-type myoepithelioma composed of small polygonal cells (arrows) with centrally located nuclei and abundant cytoplasm in a myxoid ground substance (*).

Fig. 4 Hemangioma in a 20-year-old man with lingual bulging. A. Postcontrast CT scan shows a well enhancing, clearly demarcated soft tissue mass with heterogeneous attenuation at the right lateral aspect of the tongue (arrows). Note the multiple enhancing linear or curvilinear structures suggesting hypervascularity (open arrows). B. T1-weighted axial MR image shows a homogeneous iso-intense mass (black arrow) extending across the midline. The peripheral high signal intensity rim (white arrow) increases the conspicuity of the mass. The lingual septum is seen only posteriorly, still displaced to the left (open arrow). C. T2-weighted axial image shows heterogeneously high signal intensity of the lesion. D. Enhanced T1-weighted sagittal image shows strong enhancement of the lesion and increased conspicuity of its extent. This mass is truly located in the submucosa with intact overlying mucosa. Note the large serpentine vascular structures with signal void due to rapid flow at the anterior aspect of the mass (arrows). E. Selective lingual arteriography performed for selective embolization of the lesion shows tumor staining arising mainly from hypertrophied sublingual (arrows) and deep lingual (open arrows) arteries. After embolization, the patient underwent total excision of the mass. F. Photograph of a cut section of gross specimen shows a yellowish mass with multiple vascular channels (arrows). G. Photomicrograph (original magnification ×100; H & E staining) demonstrates dilated vessels lined by flattened endothelium (short arrows), and a thick smooth muscle wall (long arrow). Note the presence of intervening skeletal muscles of the tongue (open arrow).
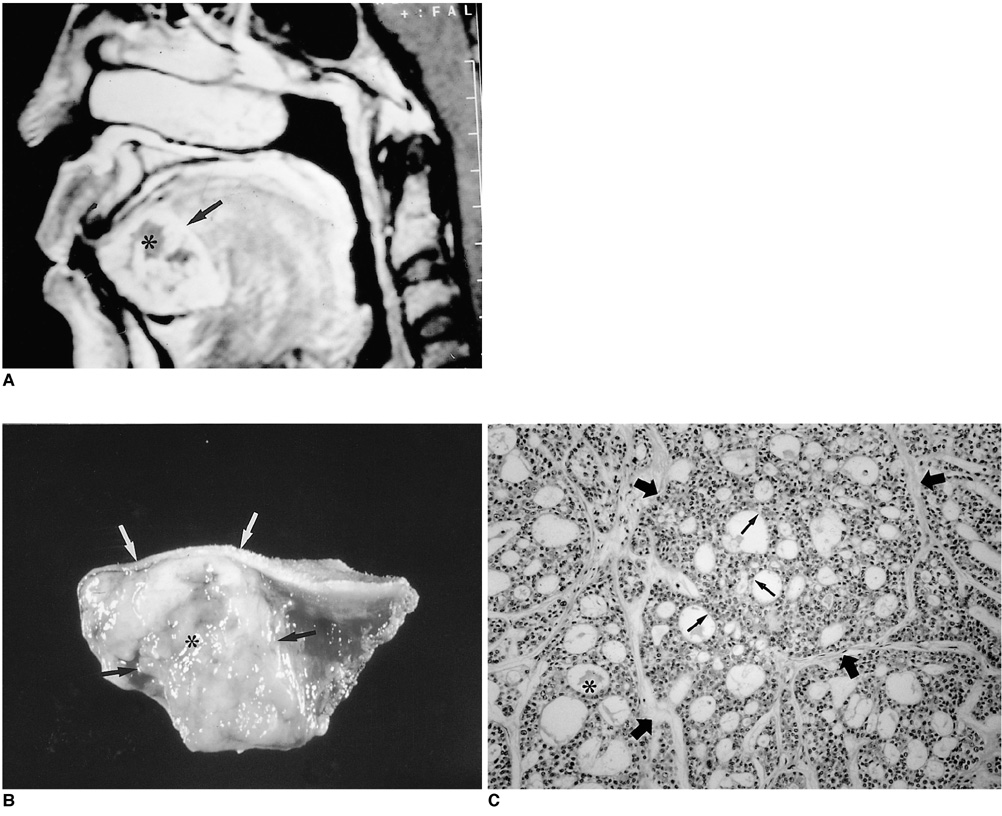
Fig. 5 Adenoid cystic carcinoma in a 63-year-old woman with growing lingual mass. A. Enhanced T1-weighted sagittal image shows a well demarcated, markedly enhancing mass in the submucosal area of the anterior tongue (arrow), with heterogeneous attenuation suggesting necrosis (*). B. Photograph of a cut section of gross specimen shows a well-demarcated yellowish mass (black arrows) with a central irregular necrotic area (*) in the anterior region of the tongue. Note the presence of intact overlying lingual mucosa (white arrows). C. Photomicrograph (original magnification ×100; H & E staining) shows tumor cells composed of uniform, small, angulated cells (thin arrows). Sharply defined cylindrical cores of hyaline material (*) create a cribriform, pseudocystic appearance (thick arrows), characteristic of grade-1 adenoid cystic carcinoma. Due to perineural invasion, the patient underwent hemiglossectomy and adjuvant chemotheraphy.
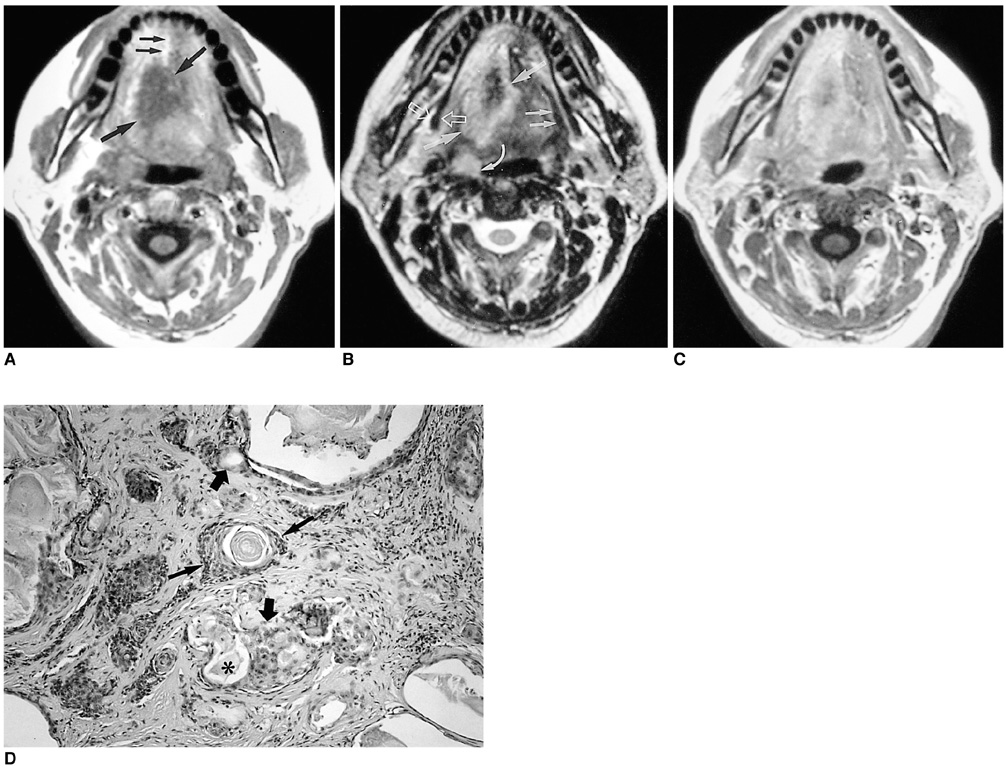
Fig. 6 Mucoepidermoid carcinoma in a 48-year-old female with a painful tongue. A. T1-weighted axial image shows a soft tissue mass with low signal intensity at the right lateral aspect of the tongue which extends across the midline (thick arrows). The lingual septum is seen only at the anterior half of the tongue (thin arrows). The right lateral margin of the mass is indistinct. B. T2-weighted axial image shows a mass with increased signal intensity (thick arrows). Anterolateral extension of this mass is more easily recognized than on the T1-weighted image. The right lateral tissue plane and hyoglossus muscle are obliterated, though on the left side are visible (thin arrows). Note the prominent right palatine tonsil (curved arrow), suggesting tonsilar metastasis, and the intact right mylohyoid muscle (open arrows). C. Enhanced T1-weighted axial image demonstrates heterogeneous, moderate enhancement, making differentiation of the mass from squamous cell carcinoma impossible. D. Photomicrograph (original magnification ×100; H & E staining) demonstrates a mixture of the glandular component lined by well-differentiated cuboidal to columnar epithelium (thick arrows) containing abundant mucous material (*) and solid nests composed of squamous cells (thin arrows).
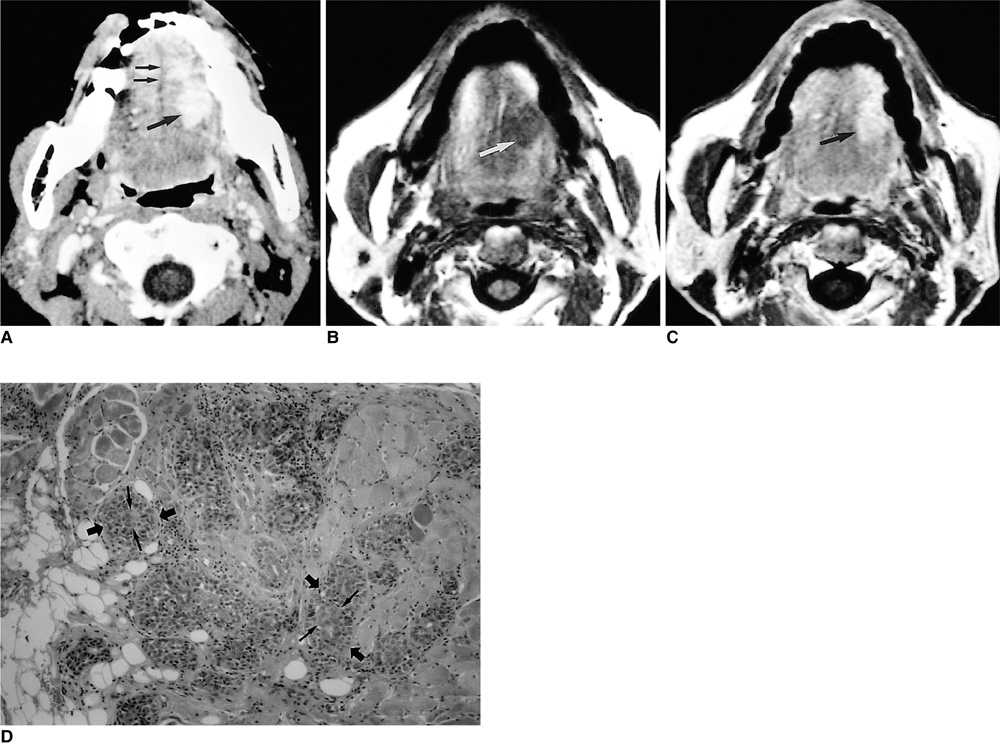
Fig. 7 Epi-myo-epi carcinoma in a 70-year-old man with tongue pain. A. Contrast-enhanced axial CT scan shows an irregularly marginated, homogeneously enhancing mass at the left lateral aspect of the tongue (thick arrow). Note the preserved midline fatty septum (thin arrows). B. T1-weighted axial image shows a mass with low signal intensity (arrow) confined to the mobile part of the tongue. C. Enhanced T1-weighted axial image shows homogenous dense enhancement of the mass(arrow). D. Photomicrograph (original magnification ×100; H & E staining) demonstrates distinctive epithelial tubules or ductules (thin arrows) surrounded by neoplastic myoepithelial cells (thick arrows).
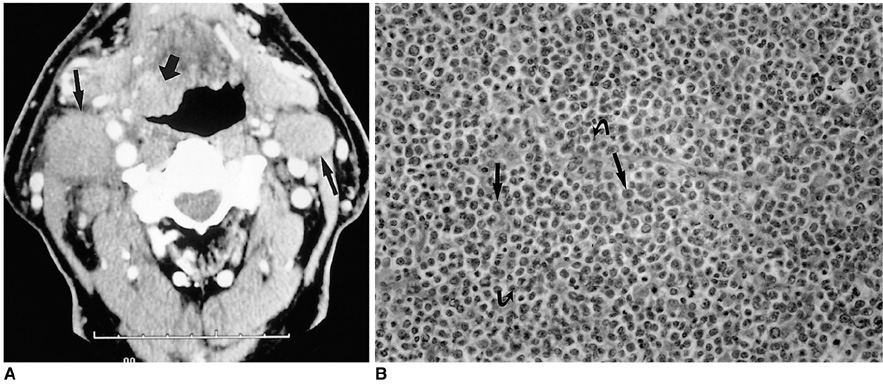
Fig. 8 Lymphoma in a 78-year-old-man with palpable neck mass. A. Contrast-enhanced CT scan obtained at the level of C3 demonstrates a moderately enhancing, poorly-defined mass involving the right-side base of the tongue and right vallecula (thick arrow). Multiple bilateral lymphadenopathies with homogeneous attenuation characteristic of lymphoma (thin arrows) are present. B. Photomicrograph (original magnification ×200; H & E staining) shows diffuse infiltration of non-cohesive, monotonous neoplastic cells with vesicular nuclei (arrows) and one or two inner nucleoli (curved arrows). The patient underwent chemotheraphy combined with radiation therapy.

Fig. 9 Metastasis from carcinoma of the bronchus in a 48-year-old man. A. Contrast-enhanced axial CT scan shows an ill-defined, well-enhancing mass at the base of the tongue and right vallecula, with exophytic growth to the oropharyngeal cavity (arrows). The superficial portion of the mass is ulcerated (curved arrow). The mass extends laterally, causing prominence of the right palatine tonsil (arrowheads). Multiple bilaterally enlarged lymph nodes can also be seen (open arrows). B. Photomicrograph (original magnification ×200; H & E staining) demonstrates poorly differentiated adenocarcinoma (arrows) metastasized from bronchogenic carcinoma. Palliative radiotherapy was performed.
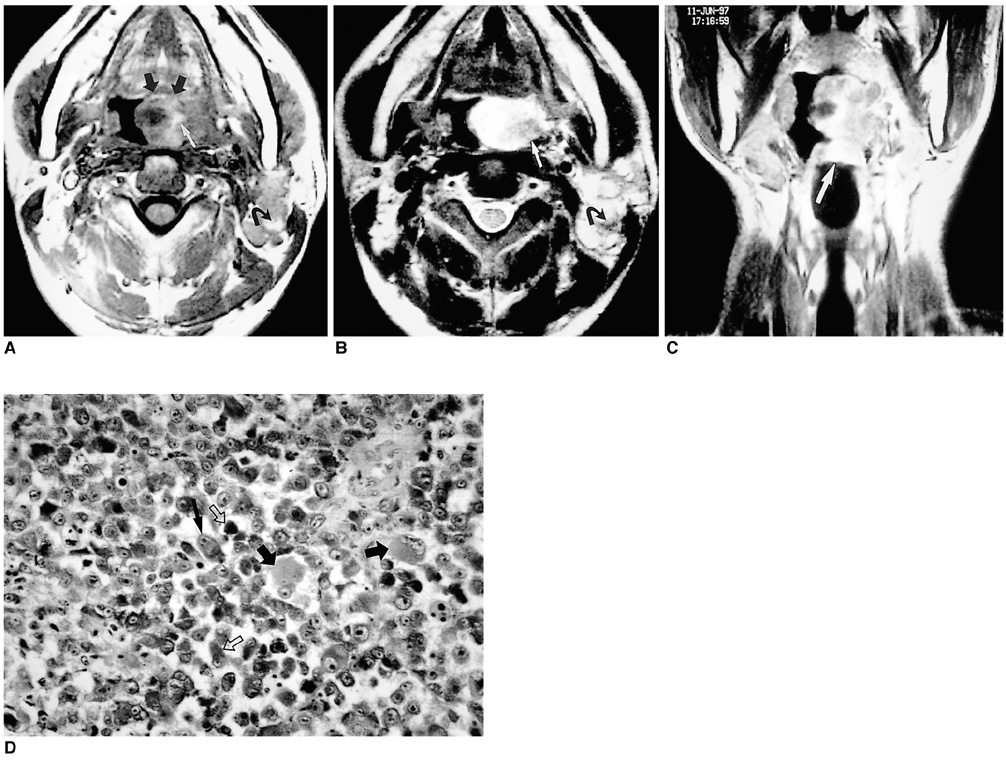
Fig. 10 Metastasis from melanotic melanoma in a 40-year-old man with severe dyspnea and hoarseness. A. T1-weighted axial image demonstrates a large mass at the left lateral base of the tongue and left lingual tonsil (thick arrows). The mass contains areas of low and high signal intensity (white arrow). In addition, multiple lymphadenopathies with high signal intensity foci (curved arrow) are seen in the left jugulodigastric chain. B. T2-weighted axial image reveals that the hyperintense areas on the T1-weighted image have become slightly hypointense (arrow). Multiple enlarged lymph nodes show mixed and heterogeneous signal intensity (curved arrow). The signal intensity characteristics of this mass suggest melanotic melanoma of the base of the tongue, with lymph node metastasis. C. Enhanced T1-weighted coronal image shows moderate enhancement of the tumor. Note extension of the tumor to the epiglottis (arrow). D. Photomicrograph (original magnification ×200; H & E staining) demonstrates the typical appearance of melanotic melanoma: large, patternlessly distributed round cells with vesicular nuclei and prominent inner nucleoli (thin arrow). A large amount of finely granulated, brown to black melanin (open arrows) is seen in the eosinophilic cytoplasm (thick arrows) of the neoplastic cells. Multiple masses where melanotic melanoma was diagnosed were present on the patient's back.
Reference
-
1. Som PM, Scherl MP, Rao VM, Biller HF. Rare presentations of ordinary lipomas of the head and neck: a review. AJNR. 1986. 7:657–664.2. Dreher A, Gutmann R, Grevers G. Extracranial schwannoma of the ENT region. Review of the literature with a case report of benign schwannoma of the base of the tongue. HNO. 1997. 45:468–471. [Article in German].3. Sciubba JJ, Brannon RB. Myoepithelioma of salivary glands: report of 23 cases. Cancer. 1982. 49:562–572.4. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 1982. 69:412–420.5. Burrows PE, Mulliken JB, Fellows KE, Strand RD. Childhood hemangiomas and vascular malformations: angiographic differentiation. AJR. 1983. 141:483–488.6. Sigal R, Monnet O, De Baere T, et al. Adenoid cystic carcinoma of the head and neck: evaluation with MR imaging and clinical-pathologic correlation in 27 patients. Radiology. 1992. 184:95–101.7. Healey WV, Perzin KH, Smith L. Mucoepidermoid carcinoma of salivary gland origin: Classification, clinical-pathologic correlation, and results of treatment. Cancer. 1970. 26:368–388.8. Corio RL. Ellis G, Auclair P, Gnepp D, editors. Epithelial-myoepithelial carcinoma. Surgical pathology of the salivary glands. 1991. Philadelphia, Pa.: WB Saunders Co.;100–109.9. Griffin TJ, Hurst PS, Swanson J. Non-Hodgkin's lymphoma: a case involving four third molar extraction sites. Oral Surg Oral Med Oral Pathol. 1988. 65:671–674.10. Zegarelli DJ, Tsukada Y, Pickren JW, Greene GW Jr. Metastatic tumor to the tongue: Report of twelve cases. Oral Surg Oral Med Oral Pathol. 1973. 35:202–211.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Review of Epithelial Tumors in the Lacrimal Gland
- Radiologic-Pathologic Correlation of Unusual Lingual Masses:Part I: Congenital Lesions
- Incidental Solid Renal Masses: Radiologic Assessment and Managements
- Usefulness of the Bosniak Classification in Cystic Renal Mass on CT
- The Comparison between Pre- and Postoperative Diagnosis in Renal Masses Smaller than 3cm in Diameter
