Pelvic Fistulas Complicating Pelvic Surgery or Diseases: Spectrum of Imaging Findings
- KMID: 754111
- DOI: http://doi.org/10.3348/kjr.2001.2.2.97
Abstract
- Pelvic fistulas may result from obstetric complications, inflammatory bowel disease, pelvic malignancy, pelvic radiation therapy, pelvic surgery, or other traumatic causes, and their symptoms may be distressing. In our experience, various types of pelvic fistulas are identified after pelvic disease or pelvic surgery. Because of its close proximity, the majority of such fistulas occur in the pelvic cavity and include the vesicovaginal, vesicouterine, vesicoenteric, ureterovaginal, ureteroenteric and enterovaginal type. The purpose of this article is to illustrate the spectrum of imaging features of pelvic fistulas.
Keyword
MeSH Terms
Figure
-
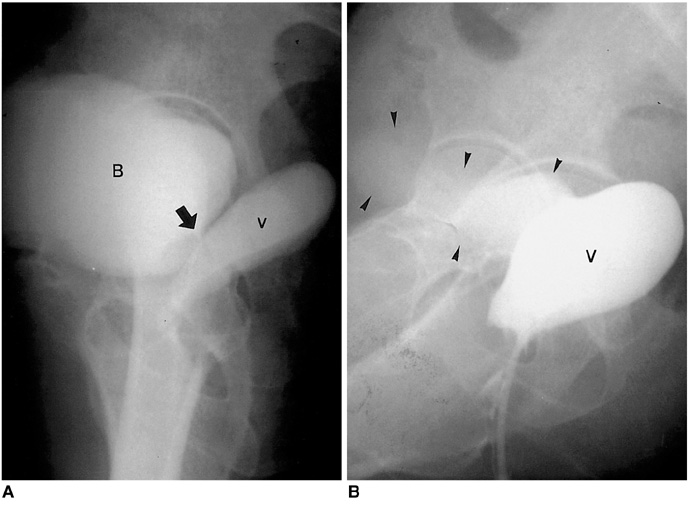
Fig. 1 Vesicovaginal fistula in a patient who underwent hysterectomy due to cervical cancer. A. Cystogram demonstrates the presence of a short fistulous tract (arrow) between the bladder neck and vaginal stump. B. Vaginogram reveals sac-forming vagina and contrast leakage into the bladder (arrowheads) (B, bladder; V, vagina).

Fig. 2 Vesicovaginal fistula in a patient who underwent hysterectomy one month earlier due to uterine myoma. Cystogram shows contrast leakage from the urinary bladder into the vagina (B, bladder; V, vagina; arrows, fistula).

Fig. 3 Vesicovaginoileal fistulas in a patient with recurrent cervical cancer who underwent hysterectomy and irradiation (arrow). A. Cystogram shows contrast leakage from the urinary bladder into the vaginal stump. B. Small bowel series indicates irregular fistulous communication (arrow) between the A distal ileum and vaginal stump (V, vagina).
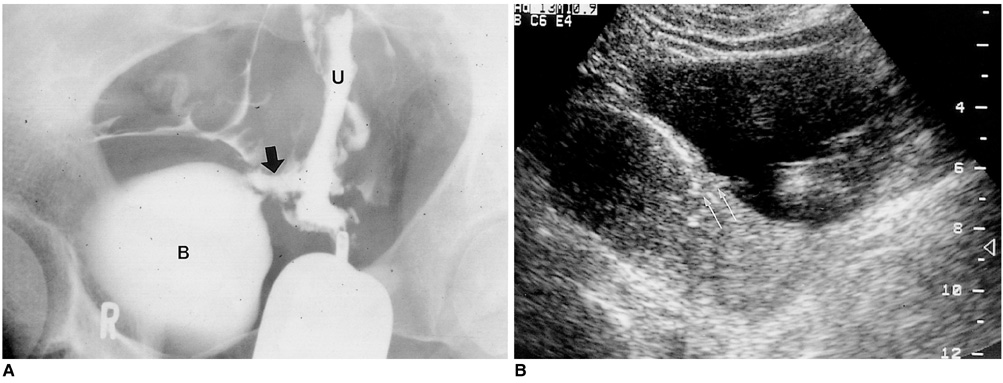
Fig. 4 Vesicouterine fistula in a patient with urinary incontinence after a cesarean section. A. Hysterosalpingogram shows a fistulous tract (arrow) and contrast leakage from the uterine cavity into the bladder. B. Longitudinal ultrasonographic scan of the pelvis demonstrates hyperechoic line in continuity with the endometrium of the uterus and bladder (Reprinted, with permission, from reference 3) (B, bladder; U, uterus; arrows, fistula).
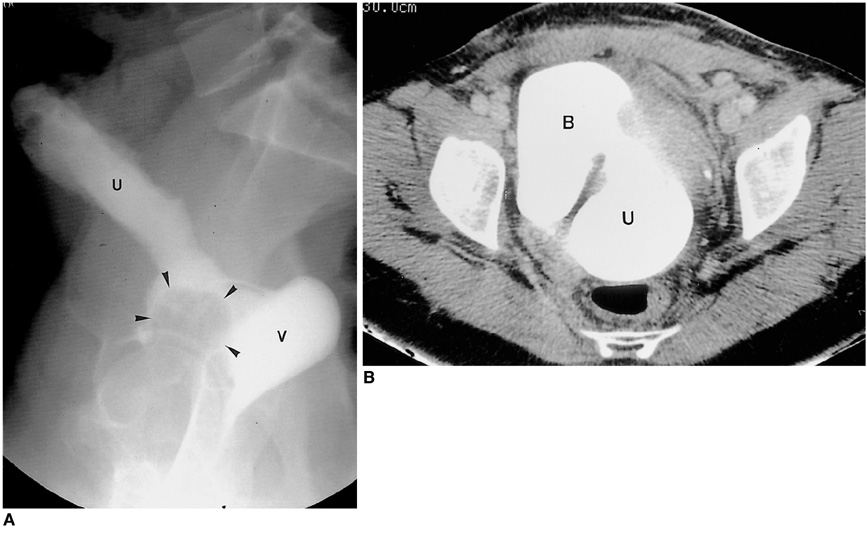
Fig. 5 Vesicouterine fistula in a patient with urinary incontinence and hematuria after a cesarean section. A. Post-voiding cystogram shows air-balloon (arrowheads) of a Foley catheter in contracted bladder and contrast filling of the uterus and vagina via the vesicouterine fistulous tract. B. CT of the pelvis performed immediately after cystography shows extensive communication between the bladder and lower body of the uterus (B, bladder; U, uterus; V, vagina).

Fig. 6 Vesicoileal fistula in a patient who had undergone irradiation on account of bladder cancer. A. Small bowel series shows two fistulous tracts (arrows) between the ileal loop and bladder. B-D. Serial CT sections obtained after a small bowel series reveal an irregular enhancing fistulous tract (arrow) and the retention of leaked contrast medium in the bladder (B, bladder).

Fig. 7 Vesicocolic fistula in a patient with Crohn's disease. A. Colon study reveals four fistulous tracts between the rectosigmoid colon and bladder. B-D. Serial CT sections of the pelvis show irregular infiltration of the sigmoid mesocolon around the fistulous tracts and air collection in the bladder (B, bladder; arrow, fistula).

Fig. 8 Vesicocolic fistula in a patient who underwent palliative radiation therapy due to recurrent bladder cancer. Cystogram shows trabeculated bladder deformity and immediately opacified sigmoid colon. The presence of a fistulous tract between the bladder and sigmoid colon may be observed (B, bladder; arrow, fistula).
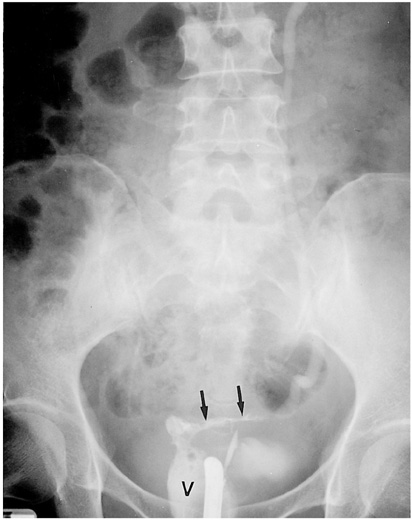
Fig. 9 Ureterovaginal fistula in a patient who underwent hysterectomy due to uterine myoma. Retrograde urogram shows contrast leakage from the left ureter to the vagina (V, vagina; arrows, fistula).

Fig. 10 Ureterovaginal fistula in a patient with watery vaginal discharge after hysterectomy due to cervical cancer. Intravenous urogram shows leakage of contrast medium from the left ureter, resulting in a triangular-shaped collection of contrast medium and continuous leakage of this through the vaginal canal (V, vagina; arrow, fistula).
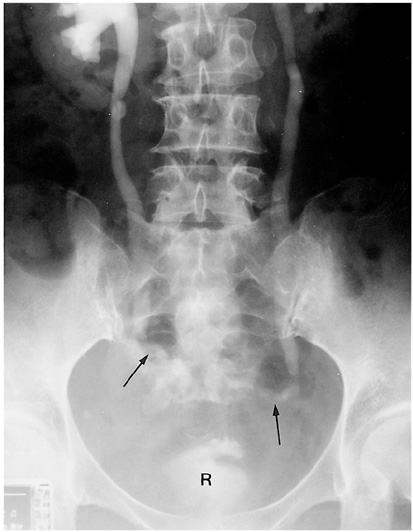
Fig. 11 Ureterorectal fistula in a patient who underwent hysterectomy due to cervical cancer. Intravenous urogram shows bilateral hydroureteronephrosis and the irregular leakage of contrast medium from the bilateral distal ureter to the rectum (R, rectum; arrows, fistula).
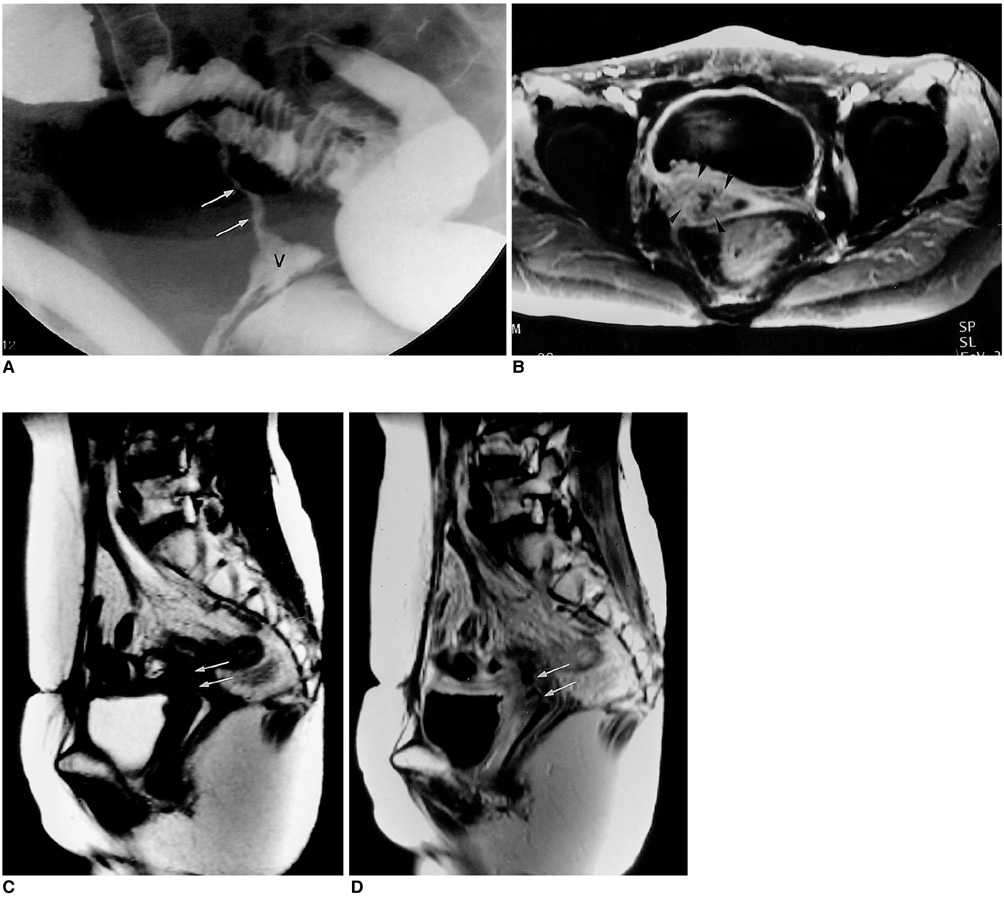
Fig. 12 Ileovaginal fistula in a patient with recurrent ovarian cancer who underwent hysterectomy, bilateral oophorectomy and adjuvant radiation therapy. A. Colon study shows a linear fistulous tract between the ileal loop and vaginal stump. B. Contrast-enhanced T1-weighted fat-suppressed MRI demonstrates an irregular enhancing polypoid mass (arrowheads) in the right aspect of the vaginal stump attached to the distal ileal loop. C, D. T2-weighted and contrast-enhanced T1-weighted sagittal images reveal the presence of a linear fistulous tract between the vaginal stump and ileal lumen (V, vagina; arrows, fistula).
Reference
-
1. Kuhlman JE, Fishman EK. CT evaluation of enterovaginal and vesicovaginal fistulas. J Comput Assist Tomogr. 1990. 14:390–394.2. Nagy V, Valansky L, Milichovsky I. Urologic complications of gynecologic surgery and their treatment in our clinical data. Ceska Gynekol. 1998. 63:192–195.3. Park BK, Kim SH, Cho JY, Sim JS, Seong CK. Vesicouterine fistula after cesarean section: ultrasonographic findings in two cases. J Ultrasound Med. 1999. 18:441–443.4. Adetiloye VA, Dare FO. Obstetric Fistula: evaluation with ulrasonography. J Ultrasound Med. 2000. 19:243–249.5. Emmert C, Kohler U. Management of genital fistula in patients with cervical cancer. Arch Gynecol Obstet. 1996. 259:19–24.6. Murphy JM, Lee G, Sharma SD, Doble A, Lomas DJ. Vesicouterine fistula: MRI diagnosis. Eur Radiol. 1999. 9:1876–1878.7. Tancer ML. Vesicouterine fistula: a review. Obstet Gynecol Surv. 1986. 41:743–753.8. Iloabachie GC, Njoku O. Vesico-uterine fistula. Br J Urol. 1985. 57:438–439.9. Alapont Perez FM, Gil Salom M, Esclapez Valero JP, et al. Acquired enterovesical fistulas. Arch Esp Urol. 1994. 47:973–979.10. Hwang JC, Ha HK, Weon YC, et al. CT findings of enteric fistula. J Korean Radiol Soc. 1997. 37:1091–1096.11. Bennett JK, Trulock TS, Finnerty DP. Urachal adenocarcinoma presenting as vesicoenteric fistula. Urology. 1985. 25:297–299.12. Selzman AA, Patrick Spirnak J, Kursh ED. The changing management of ureterovaginal fistulas. J Urol. 1995. 153:626–628.13. Cirocco WC, Priolo SR, Golub RW. Spontaneous ureterocolic fistula; a rare complication of colonic diverticular disease. Am Surg. 1994. 60:832–835.14. Husted JW. An unusual case of pyelonephritis: Nephrocolic fistula owing to a ruptured colonic diverticulum. J Urol. 1974. 111:724–726.15. Lee BH, Choe DH, Lee JH, et al. Device for occlusion of rectovaginal fisula: clinical trials. Radiology. 1997. 203:65–69.
