MR Imaging of Central Diabetes Insipidus: A Pictorial Essay
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine. hklee2@www.amc.seoul.kr
- 2Department Neurosurgery, Asan Medical Center, University of Ulsan College of Medicine.
- 3Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine.
- 4Department of Radiology , Samsung Medical Center, Sungkyunkwan University College of Medicine.
- KMID: 754092
- DOI: http://doi.org/10.3348/kjr.2001.2.4.222
Abstract
- Central diabetes insipidus (DI) can be the outcome of a number of diseases that affect the hypothalamic-neurohypophyseal axis. The causes of the condition can be classified as traumatic, inflammatory, or neoplastic. Traumatic causes include postoperative sella or transection of the pituitary stalk, while infectious or inflammatory causes include meningitis, lymphocytic hypophysitis, and granulomatous inflammations such as sarcoidosis and Wegener's granulomatosis. Various neoplastic conditions such as germinoma, Langerhans cell histiocytosis, metastasis, leukemic infiltration, lymphoma, teratoma, pituitary adenoma, craniopharyngioma, Rathke cleft cyst, hypothalamic glioma, and meningioma are also causes of central DI. In affected patients, careful analysis of these MR imaging features and correlation with the clinical manifestations can allow a more specific diagnosis, which is essential for treatment.
MeSH Terms
Figure
-
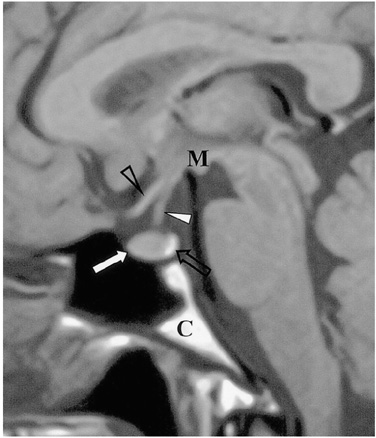
Fig. 1 Sagittal T1-weighted MR image shows the normal anatomy of the sella turcica and juxtasellar region. The anterior lobe (thick arrow), posterior lobe (open arrow), pituitary stalk (thick arrowhead), optic chiasm (open arrowhead), mamillary body (M), and clivus (C) are indicated.

Fig. 2 Transection of the pituitary stalk caused by a fall in a 17-year-old male. The signs and symptoms of DI developed two months after trauma. Sagittal T1-weighted MR image (600/15) reveals diffuse atrophy of the pituitary gland (arrows). The high signal intensity normally seen in the posterior lobe is absent, and the normal pituitary stalk is not seen. Two foci of high signal intensity anterior and posterior to the pituitary fossa represent the fat marrow of the sella turcica.
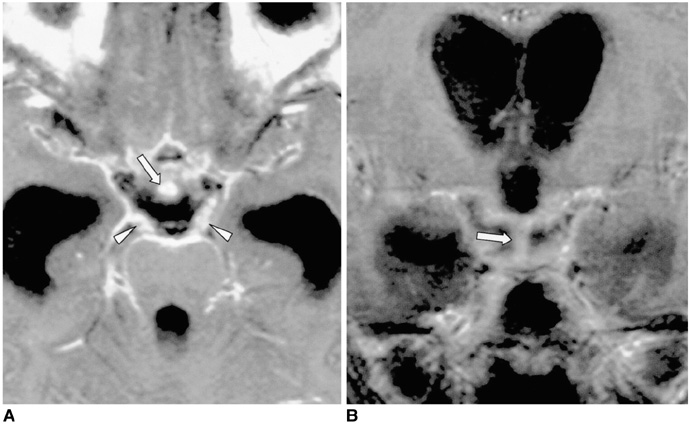
Fig. 3 Tuberculous meningitis in a 10-year-old boy with multiple cranial nerve palsy. A, B. Contrast-enhanced axial (A) and coronal (B) T1-weighted MR images (600/20) depict enhancement of the uniformly thickened pituitary stalk (arrows) and diffuse leptomeningeal enhancement in the basal cistern. Strong enhancement of the bilateral thickened third nerves (arrowheads in A) and severe communicating hydrocephalus are noted. Tuberculous meningitis was confirmed by cerebrospinal fluid analysis.

Fig. 4 Epidemic hemorrhagic fever in a 52-year-old man. Sagittal fat-suppressed T1-weighted MR image (600/20) shows diffuse atrophy of the pituitary gland. The focal high signal intensities observed (arrows) suggest hemorrhage in the pituitary gland, which may occur in the course of this disease.
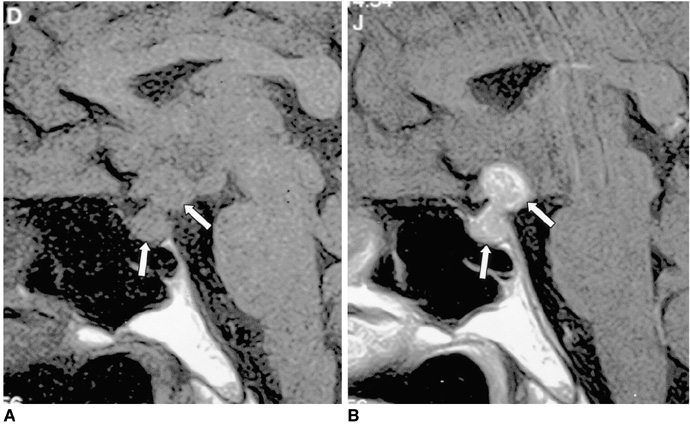
Fig. 5 Lymphocytic infundibulohypophysitis in a 43-year-old man. A. Sagittal T1-weighted MR image (500/25) depicts an isointense mass comprising the hypothalamus, the pituitary stalk, and the pituitary gland (arrows). The posterior lobe no longer shows high signal intensity. B. Contrast-enhanced sagittal T1-weighted MR image (500/25) shows strong enhancement of the mass (arrows). Lymphocytic infundibulohypophysitis was pathologically proven.
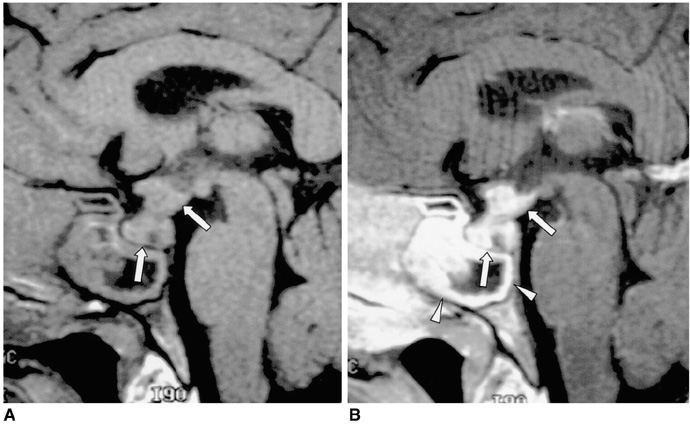
Fig. 6 Churg-Strauss syndrome in a 38-year-old man. A. Sagittal T1-weighted MR image (600/15) reveals an isointense mass involving the hypothalamus, pituitary stalk and pituitary gland (arrows). The posterior lobe no longer shows high signal intensity. Prominent mucosal thickening of the sphenoid sinus is apparent. B. Contrast-enhanced sagittal T1-weighted MR image (600/15) demonstrates strong enhancement of the mass (arrows), and there is a non-enhancing portion. The thickened mucosa of the sphenoid sinus is intensely enhanced, representing sphenoid sinusitis (arrowheads). Churg-Strauss syndrome was pathologically proven.
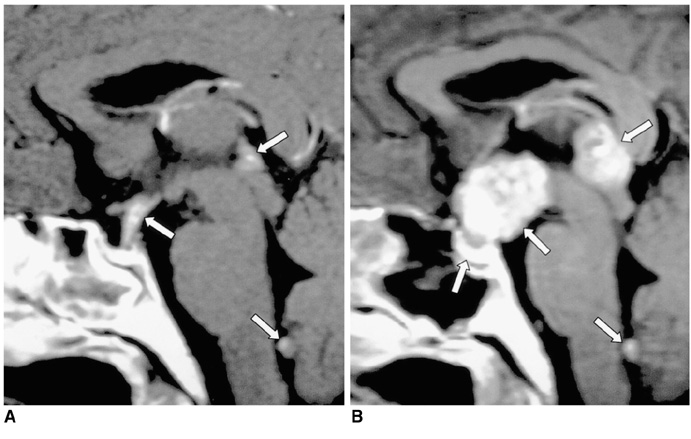
Fig. 7 Germinoma in a 29-year-old man. A. Initial contrast-enhanced sagittal T1-weighted MR image (600/15) depicts mild thickening and homogeneous enhancement of the pituitary stalk. In addition, small nodular enhancing lesions are seen in the pineal gland outlet of the fourth ventricle (arrows). B. Contrast-enhanced sagittal T1-weighted MR image (480/14) obtained one year later, without treatment, shows a marked increase in the size and inhomogeneous enhancement of those lesions, and also of the pituitary gland (arrows). The focal enhancing lesion seen within the fourth ventricle appears to be cerebrospinal seeding. Germinoma was pathologically proven.
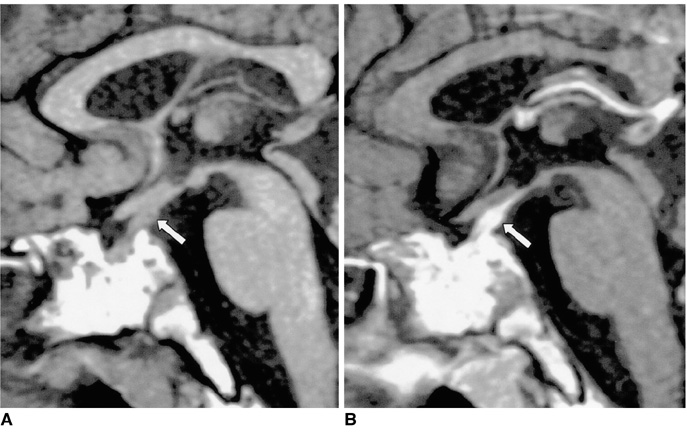
Fig. 8 Langerhans cell histiocytosis in a 15-year-old boy. A. Sagittal T1-weighted MR image (600/15) demonstrates a uniformly thickened pituitary stalk (arrow). The posterior lobe no longer shows high signal intensity. B. Contrast-enhanced sagittal T1-weighted MR image (600/15) shows strong enhancement of the lesion (arrow). The high signal intensity in the sphenoid sinus presumably represents fat marrow associated with poor pneumatization. Langerhans cell histiocytosis was pathologically proven.
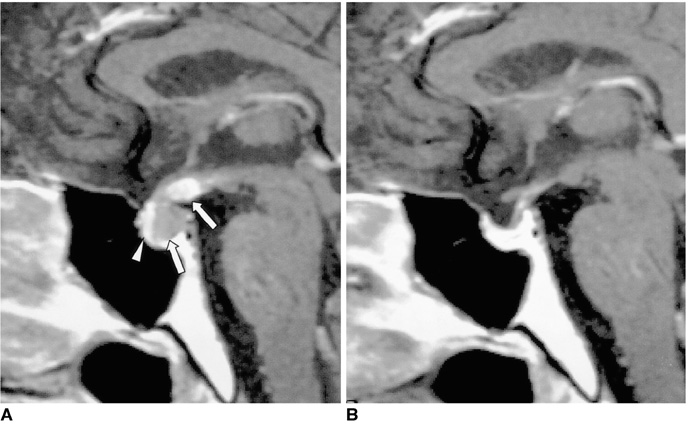
Fig. 9 Metastasis from lung cancer in a 41-year-old man. A. Contrast-enhanced sagittal T1-weighted MR image (600/16) depicts the markedly enhancing thickened median eminence and pituitary stalk, and less enhancing posterior lobe (arrows). The posterior lobe no longer shows high signal intensity, and the normally enhanced anterior lobe (arrowhead) is compressed and displaced anteriorly by the enlarged posterior lobe. B. Contrast-enhanced sagittal T1-weighted MR image (600/23) obtained two months after radiotherapy shows near disappearance of the lesion. The clinical symptoms of DI were also much improved.
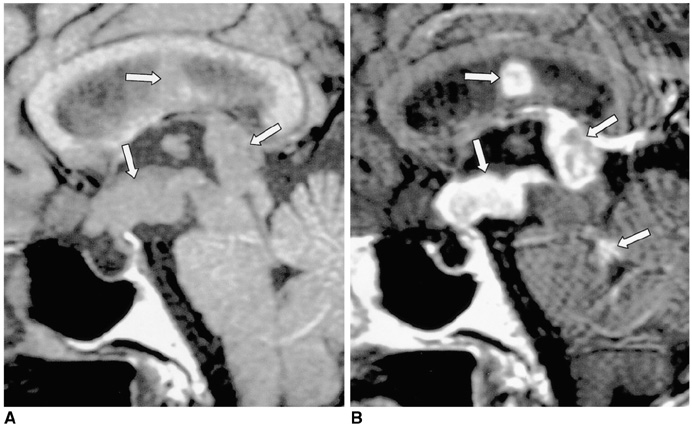
Fig. 10 Primary intraventricular lymphoma (non-Hodgkin's lymphoma) in a 77-year-old woman. A. Sagittal T1-weighted MR image (600/15) depicts multiple masses in the hypothalamus, floor and posterior wall of the third ventricle and septum pellucidum (arrows). The posterior lobe no longer shows high signal intensity. B. Contrast-enhanced sagittal T1-weighted MR image (600/15) shows strong enhancement of the above mentioned lesions and of the superior portion of the fourth ventricle (arrows), indicating lymphomatous involvement. Lymphoma was pathologically proven.
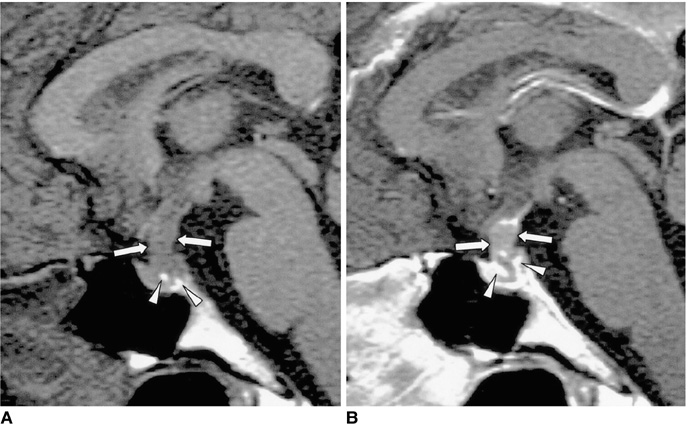
Fig. 11 Pituitary adenoma in a 42-year-old man. A. Sagittal T1-weighted MR image (600/15) shows marked thickening of the pituitary stalk (arrows). The posterior lobe, displaced by the lesion, is seen as several foci of high signal intensity (arrowheads). B. Contrast-enhanced sagittal T1-weighted MR image (600/15) demonstrates homogeneous mild enhancement of the thickened pituitary stalk, which extends into the pituitary fossa and displaces the normal pituitary gland to the left side. Due to strong enhancement, the displaced and compressed pituitary gland is seen as multiple foci of high signal intensity (arrows). Although the mass was found to completely encircle the pituitary stalk, at surgery the two were separated easily. Pituitary adenoma was pathologically proven.
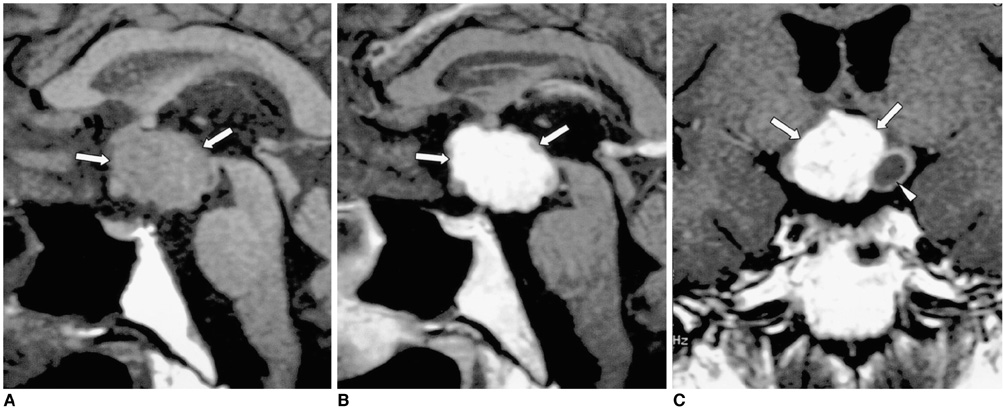
Fig. 12 Craniopharyngioma in a 34-year-old man. A. Sagittal T1-weighted MR image (600/15) shows a large lobulated mass (arrows) involving the suprasellar area and hypothalamus. The posterior lobe no longer shows high signal intensity. B, C. Contrast-enhanced sagittal (B) and coronal (C) T1-weighted MR images (600/15) show strong enhancement of the solid component of the tumor (arrows), which also has a smaller cystic component (arrowhead in C). Craniopharyngioma was pathologically proven.
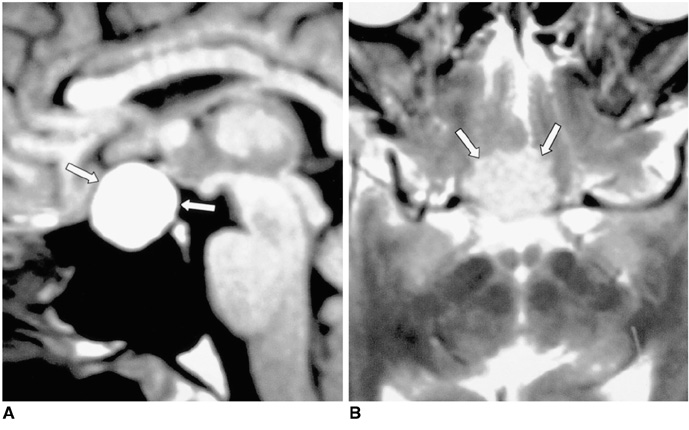
Fig. 13 Rathke cleft cyst in a 59-year-old woman. A. Sagittal T1-weighted MR image (600/15) depicts a well-defined, homogeneous high signal intensity mass (arrows) in the sella turcica and extending into the suprasellar cistern. B. Axial T2-weighted (3500/99) MR image indicates that the mass is isointense relative to gray matter (arrows), reflecting the high protein concentration of the cystic fluid. A Rathke cleft cyst was pathologically proven.
Cited by 1 articles
-
Pituitary Teratoma Presenting as Central Diabetes Insipidus with a Normal MRI Finding
Young Soo Kim, Seok Gu Kang, Young OK Kim
Yonsei Med J. 2010;51(2):293-294. doi: 10.3349/ymj.2010.51.2.293.
Reference
-
1. Ozata M, Tayfun C, Kurtaran K, et al. Magnetic resonance imaging of posterior pituitary for evaluation of the neurohypophyseal function in idiopathic and autosomal dominant neurohypophyseal diabetes insipidus. Eur Radiol. 1997. 7:1098–1102.2. Kucharczyk W, Lenkinski RE, Kucharczyk J, Henkelman RM. The effect of phospholipid vesicles on the NMR relaxation of water: an explanation for the MR appearance of the neurohypophysis? AJNR. 1990. 11:693–700.3. Ma L, Gao Y, Cai Y, Li T, Liang Y. MR evaluation of the brain in central diabetes insipidus. Chin Med J. 1996. 109:724–729.4. Tien R, Kucharczyk J, Kucharczyk W. MR imaging of the brain in patients with diabetes insipidus. AJNR. 1991. 12:533–542.5. Black PM, Zervas NT, Candia GL. Incidence and management of complications of transsphenoidal operation for pituitary adenomas. Neurosurgery. 1987. 20:920–924.6. Suh DC, Park JS, Park SK, Lee HK, Chang KH. Pituitary hemorrhage as a complication of hantaviral disease. AJNR. 1995. 16:175–178.7. Ahmed SR, Aiello DP, Page R, Hopper K, Towfighi J, Santen RJ. Necrotizing infundibulo-hypophysitis: a unique syndrome of diabetes insipidus and hypopituitarism. J Clin Endocrinol Metab. 1993. 76:1499–1504.8. Maghnie M. Lymphocytic hypophysitis and central diabetes insipidus during adolescence: what are the criteria for diagnosis? Eur J Pediatr. 1998. 157:693–694.9. Imura H, Nakao K, Shimatsu A, et al. Lymphocytic infundibuloneurohypophysitis as a cause of central diabetes insipidus. N Engl J Med. 1993. 329:683–689.10. Maghnie M, Genovese E, Sommaruga MG, et al. Evolution of childhood central diabetes insipidus into panhypopituitarism with a large hypothalamic mass: is lymphocytic 'infundibuloneurohypophysitis' in children a different entity? Eur J Endocrinol. 1998. 139:635–640.11. Vomacka Z, Ehrmann J, Skvarilova M, Krc I. Granulomatous vasculitis of Churg-Strauss type in a patient with diabetes insipidus. Acta Univ Palacki Olomuc Fac Med. 1993. 135:17–19.12. Tien RD, Newton TH, McDermott MW, Dillon WP, Kucharczyk J. Thickened pituitary stalk on MR images in patients with diabetes insipidus and Langerhans cell histiocytosis. AJNR. 1990. 11:703–708.13. Szuwart U, Konig HJ, Bennefeld H, Weritz C, Kleinhans G. Clinical aspects of hypophyseal metastases. Onkologie. 1988. 11:66–69.14. Ra'anani P, Shpilberg O, Berezin M, Ben-Bassat I. Acute leukemia relapse presenting as central diabetes insipidus. Cancer. 1994. 73:2312–2316.15. Balmaceda CM, Fetell MR, Selman JE, Seplowitz AJ. Diabetes insipidus as first manifestation of primary central nervous system lymphoma. Neurology. 1994. 44:358–359.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Central Diabetes Insipidus Associated with Brachycephaly
- Morphea and Verruca Plana Complicated in Central Diabetes Insipidus
- A Case of Central Diabetes Insipidus Developed during Puerperium
- Imaging Features of the Mesenchymal Tumors of the Breast according to WHO Classification: A Pictorial Essay
- A Case of Hyperglycemic Hyperosmolar Syndrome in a Patient with Central Diabetes Insipidus and Type 2 Diabetes Mellitus
