Diffusion-Weighted MR Imaging in Biopsy-Proven Creutzfeldt-Jakob Disease
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, and Institute of Radiation Medicine, SNUMRC, Seoul, Korea. changkh@radcom.snu.ac.kr
- 2Department of Neurology, Seoul National University College of Medicine.
- KMID: 754087
- DOI: http://doi.org/10.3348/kjr.2001.2.4.192
Abstract
OBJECTIVE
To compare conventional and diffusion-weighted MR imaging in terms of their depiction of the abnormalities occurring in Creutzfeldt-Jakob disease. MATERIALS AND METHODS: We retrospectively analyzed the findings of conventional (T2-weighted and fluid-attenuated inversion recovery) and diffusion-weighted MR imaging in four patients with biopsy-proven Creutzfeldt-Jakob disease. The signal intensity of the lesion was classified by visual assessment as markedly high, slightly high, or isointense, relative to normal brain parenchyma. RESULTS: Both conventional and diffusion-weighted MR images demonstrated bilateral high signal intensity in the basal ganglia in all four patients. Cortical lesions were observed on diffusion-weighted MR images in all four, and on fluid-attenuated inversion recovery MR images in one, but in no patient on T2-weighted images. Conventional MR images showed slightly high signal intensity in all lesions, while diffusion-weighted images showed markedly high signal intensity in most. CONCLUSION: Diffusion-weighted MR imaging is more sensitive than its conventional counterpart in the depiction of Creutzfeldt-Jakob disease, and permits better detection of the lesion in both the cerebral cortices and basal ganglia.
Keyword
MeSH Terms
Figure
-
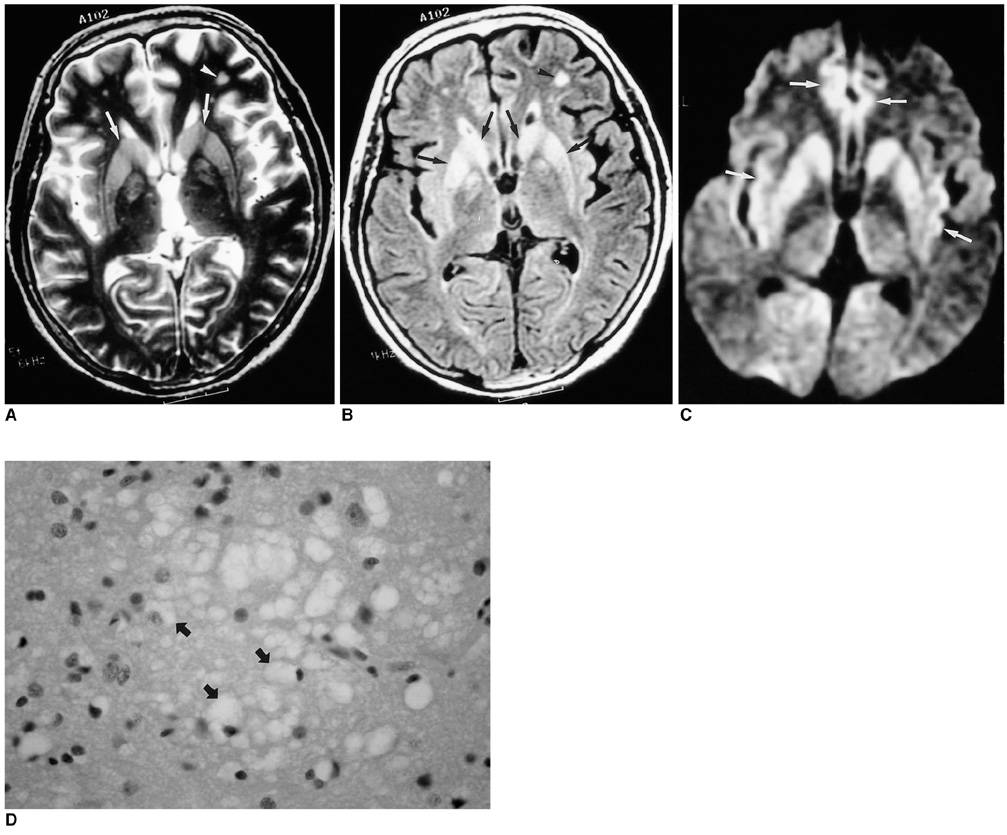
Fig. 1 Case 1, a 63-year-old woman with Creutzfeldt-Jakob disease. A and B. T2-weighted (A) and fluid-attenuated inversion recovery (B) MR images show bilateral high signal intensity in the putamen and caudate nucleus (arrows). There are small foci of high signal intensity in the frontal white matter (arrowhead), suggesting focal ischemia due to small vessel disease. C. Diffusion-weighted MR image demonstrates bilateral high signal intensity in the frontal and insular cortices (arrows), as well as the basal ganglia. D. Photomicrograph of the cerebral cortex shows numerous small vacuoles (arrows), indicating spongiform change and a reduced number of nerve cells (original magnification ×400; hematoxylin-eosin staining).
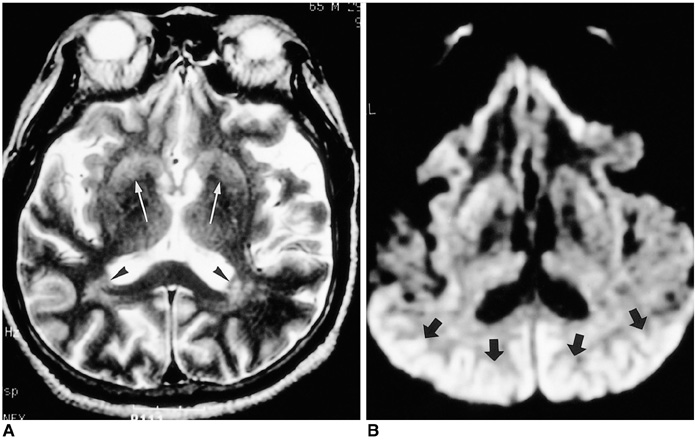
Fig. 2 Case 3, a 65-year-old man with Creutzfeldt-Jakob disease. A. T2-weighted MR images show slightly increased signal intensity (arrows) in the putamen and caudate nucleus, bilaterally. High signal intensity foci (arrowheads) are seen in the posterior periventricular areas, suggesting focal ischemia due to small vessel disease. B. Diffusion-weighted MR image demonstrates markedly increased signal intensity throughout the occipitotemporal cortex (arrows) and slightly increased signal intensity in the basal ganglia, bilaterally.
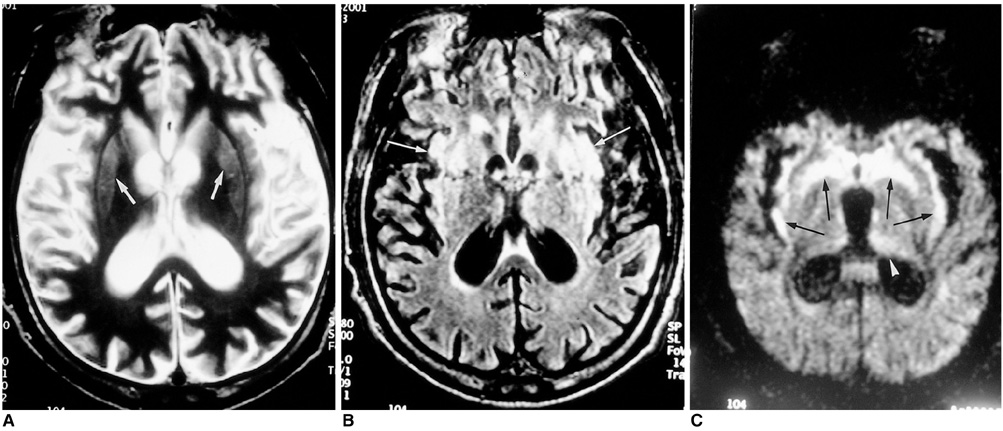
Fig. 3 Case 4, a 36-year-old man with Creutzfeldt-Jakob disease. A. T2-weighted MR image shows severe diffuse atrophy and slightly increased signal intensity in the basal ganglia, bilaterally (arrows). B. Fluid-attenuated inversion recovery MR image shows bilaterally increased signal intensity in both the insular cortex (arrows) and basal ganglia. C. Diffusion-weighted MR image demonstrates conspicuous bilateral high intensity in the insular cortex and basal ganglia (arrows). Subtle high signal intensity of the left thalamus (arrowhead) is also apparent.
Reference
-
1. Brown P, Cathala F, Castaigne P, Gajdusek DC. Creutzfeldt-Jakob disease: clinical analysis of a consecutive series of 230 neuropathologically verified cases. Ann Neurol. 1986. 20:597–602.2. Prusiner SB. Molecular biology of prion diseases. Science. 1991. 252:1515–1522.3. Finkenstaedt M, Szudra A, Zerr I, et al. MR imaging of Creutzfeldt-Jakob disease. Radiology. 1996. 199:793–798.4. Bahn MM, Kido DK, Lin W, Pearlman AL. Brain magnetic resonance diffusion abnormalities in Creutzfeldt-Jakob disease. Arch Neurol. 1997. 54:1411–1415.5. Bahn MM, Parchi P. Abnormal diffusion-weighted magnetic resonance images in Creutzfeldt-Jakob disease. Arch Neurol. 1999. 56:577–583.6. Na DL, Suh CK, Choi SH, et al. Diffusion-weighted magnetic resonance imaging in probable Creutzfeldt-Jakob disease. Arch Neurol. 1999. 56:951–957.7. Demaerel P, Heiner L, Robberecht W, Sciot R, Wilms G. Diffusion-weighted MRI in sporadic Creutzfeldt-Jakob disease. Neurology. 1999. 52:205–208.8. Stejskal EO, Tanner JE. Spin diffusion measurements: spin echoes in the presence of a time-dependent field gradient. J Chem Physiol. 1965. 42:288–292.9. Gideon P, Sorensen PS, Thomsen C, et al. Increased brain water self-diffusion in patients with idiopathic intracranial hypertension. AJNR. 1995. 16:381–387.10. Masters CL, Richardson EP Jr. Subacute spongiform encephalopathy (Creutzfeldt-Jakob disease): the nature and progression of spongiform change. Brain. 1978. 101:333–344.11. Zeidler M, Sellar RJ, Collie DA, et al. The pulvinar sign on magnetic resonance imaging in variant Creutzfeldt-Jakob disease. Lancet. 2000. 355:1412–1418.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Four Cases of Probable Creutzfeldt-Jacob Disease with High Signals in Cerebral Cortex on Diffusion Weighted MR Imaging
- Diffusion-Weighted MRI in Creutzfeldt-Jakob Disease: Focus on the Cerebral Cortex and Chronologic Change
- Rapidly Aggravated Creutzfeldt-Jacob Disease: Autopsy-Proven Case
- A case of Creutzfeldt-Jakob disease
- White Matter Lesions in a Patient With Creutzfeldt-Jakob Disease
