Imaging Findings of Castleman's Disease Localized in the Axilla: A Case Report
- Affiliations
-
- 1Department of Diagnostic Radiology, Korea University Hospital, Korea. ssbk@dreamwiz.com
- 2Department of Pathology, Korea University Hospital, Korea.
- 3Department of General Surgery, Korea University Hospital, Korea.
- KMID: 754074
- DOI: http://doi.org/10.3348/kjr.2002.3.2.136
Abstract
- Castleman's disease is a rare benign lymphoproliferative disorder of uncertain origin which most commonly involves the mediastinum but rarely affects the axilla. We report a case of localized Castleman's disease involving the axillary lymph node. Mammography revealed a well-defined, homogeneously dense ovoid mass, 3 cm in size, in the left axilla, while gray-scale ultrasonography (US) demonstrated a well-defined, uniformly hypoechoic ovoid mass with good through transmission. Peripheral hypervascularity was observed at power Dopper US, and early rapid homogeneous enhancement at contrast-enhanced dynamic CT.
MeSH Terms
Figure
-
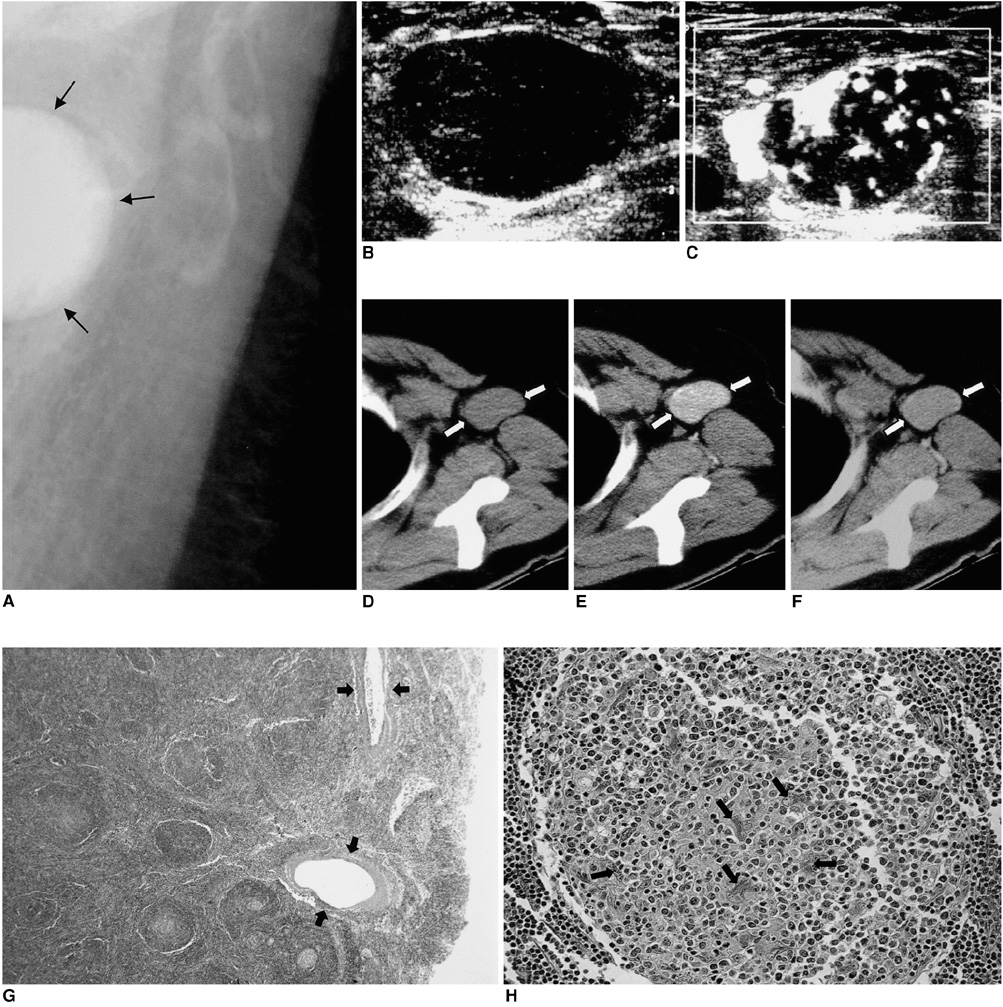
Fig. 1 45-year-old woman with localized Castleman's disease. A. Mediolateral oblique mammogram depicts a well-defined, high-density ovoid mass (arrows) in the left axilla. B, C. Transverse gray-scale US reveals a well-defined, homogeneously hypoechoic ovoid mass with good through transmission (B), while power Doppler US shows that vascularity is more prominent at the periphery than in the central portion of the lymph node. Both linear and branching vascularity are seen along the periphery (C). D-F. At triphasic CT performed after the injection of intravenous contrast material, the lymph node (arrows) appears isodense to chest wall muscle at precontrast scanning (D), shows homogeneous rapid enhancement at the early phase (E), and is washed out at the delayed phase (F). G, H. Pathologic examination revealed characteristic tight concentric layering of lymphocytes at the periphery of the lymphoid follicles, with penetration by small capillaries. The peripheral portion of the node has larger and many more blood vessels (arrows) than the central portion (G) (original magnification, ×4; hematoxylin-eosin staining). In the germinal center, multinucleated and pleomorphic follicular dendritic cells (arrows) are present, indicating follicular dendritic cell dysplasia (H) (original magnification, ×200; hematoxylin-eosin staining).
Reference
-
1. Castleman B, Iverson L, Menendez VP. Localized mediastinal lymph-node hyperplasia resembling thymoma. Cancer. 1956. 9:822–830.2. Elizalde JM, Eizaguirre B, Lopez JI. Angiofollicular giant lymph node hyperplasia that presented with an axillary mass. Eur J Surg. 1993. 159:183–184.3. McCarthy MJ, Vukelja SJ, Banks PM, Weiss RB. Angiofollicular lymph node hyperplasia (Castleman's disease). Cancer Treat Rev. 1995. 21:291–310.4. Keller AR, Hochholzer L, Castleman B. Hyaline vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer. 1972. 29:670–681.5. Weisenburger DD, Nathwani BN, Winberg CD, Rappaport H. Multicentric angiofollicular lymph node hyperplasia: a clinicopathologic study of 16 cases. Hum Pathol. 1985. 16:162–172.6. Danon AD, Krishnan J, Frizzera G. Morpho-immunophenotypic diversity of Castleman's disease, hyaline-vascular type: with emphasis on a stroma-rich variant and a new pathogenetic hypothesis. Virchows Arch A Pathol Anat Histopathol. 1993. 423:369–382.7. Moon WK, Kim WS, Kim IO, Yeon KM, Han MC. Castleman's disease in the child: CT and ultrasound findings. Pediatr Radiol. 1994. 24:182–184.8. Bui-Mansfield LT, Chew FS, Myers CP. Angiofollicular lymphoid hyperplasia (Castleman's disease) of the axilla. AJR. 2000. 174:1060.9. Yang WT, Chang J, Metreweli C. Patients with breast cancer: differences in color Doppler flow and gray-scale US features of benign and malignant axillary lymph nodes. Radiology. 2000. 215:568–573.10. Tschammler A, Ott G, Schang T, Seelbach-Goebel B, Schwager K, Hahn D. Lymphadenopathy: differentiation of benign from malignant disease-color Doppler US assessment of intranodal angioarchitecture. Radiology. 1998. 208:117–123.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MRI findings of castleman disease (Giant lymph node hyperplasia): case report
- Castleman's Disease in the Sigmoid Mesocolon: A Case Report
- A Case of Localized Castleman's Disease in a Patient with Rheumatoid Arthritis
- Hyaline-vascular Variant of Castleman's Disease in Retroperitoneum
- Castleman Disease Arising from IVlesentery: A Case Report
