Differentiation of Recently Infarcted Myocardium from Chronic Myocardial Scar: The Value of Contrast-Enhanced SSFP-Based Cine MR Imaging
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. seojb@amc.seoul.kr
- KMID: 753911
- DOI: http://doi.org/10.3348/kjr.2006.7.1.14
Abstract
- The purpose of this study is to demonstrate whether the signal intensity (SI) of myocardial infarction (MI) on contrast enhanced (CE)-cine MRI is useful for differentiating recently infarcted myocardium from chronic scar. This study included 24 patients with acute MI (36-84 years, mean age: 57) and 19 patients with chronic MI (44-80 years, mean age: 64). The diagnosis of acute MI was based on the presence of typical symptoms, i.e. elevation of the cardiac enzymes and the absence of any remote infarction history. The diagnosis of chronic MI was based on a history of MI or coronary artery disease of more than one month duration and on the absence of any recent MI within the previous six months. Retrospectively, the ECG-gated breath-hold cine imaging was performed in the short axis plane using a segmented, balanced, turbo-field, echo-pulse sequence two minutes after the administration of Gd-DTPA at a dose of 0.2 mmol/kg body weight. Delayed contrast-enhanced MRI (DCE MRI) in the same plane was performed 10 to 15 minutes after contrast administration, and this was served as the gold standard of reference. The SI of the infarcted myocardium on the CE-cine MRI was compared with that of the normal myocardium on the same image. The area of abnormal SI on the CE-cine MRI was compared with the area of hyperenhancement on the DCE MRI. The area of high SI on the CE-cine MRI was detected in 23 of 24 patients with acute MI (10 with homogenous high SI, 13 high SI with subendocardial low SI, and one with iso SI). The area of high SI on the CE-cine MRI was larger than that seen on the DCE MRI (p < 0.05). In contrast, the areas of chronic MI were seen as iso-SI with thin subendocardial low SI on the CE-cine MR in all the chronic MI patients. The presence of high SI on both the CE-cine MRI and the DCE MRI is more sensitive (95.8%) for determining the age of a MI than the presence of myocardial thinning (66.7%). This study showed the different SI patterns between recently infarcted myocardium and chronic scar on the CE-cine MRI. CE-cine MRI is thought to be quite useful for determining the age of myocardial infarction, in addition to its utility for assessing myocardial contractility.
MeSH Terms
Figure
-
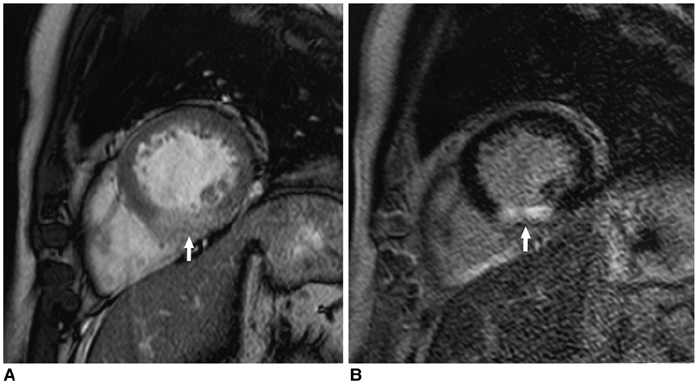
Fig. 1 Both the contrast-enhanced cine (A) and delayed contrast-enhanced (B) MR images in a 71-year-old male who had a history of chest pain for three days. The images show an area of high signal intensity in the middle inferior and inferoseptal wall (arrows). Note that the area of abnormal signal intensity on the contrast-enhanced-cine MR is larger than that on the delayed contrast-enhanced MR.
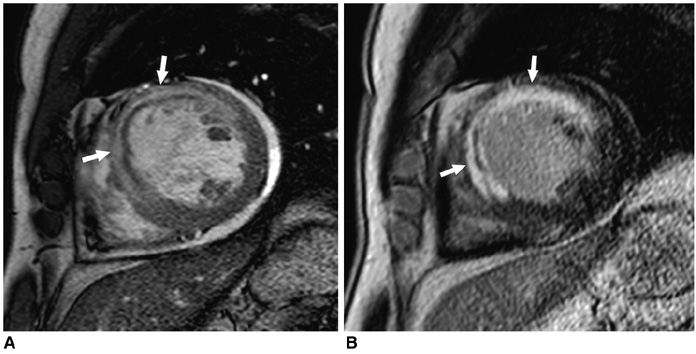
Fig. 2 The MR scan obtained on a 64-year-old male with acute myocardial infarction. The contrast-enhanced cine MR scan on the mid-diastolic phase (A) shows an area of high signal intensity with internal low signal intensity in the anterior and anteroseptal wall (arrows), and this lesion was confirmed as an area of myocardial infarction with a subendocardial no-reflow zone on the delayed contrast-enhanced MR scanning (B).
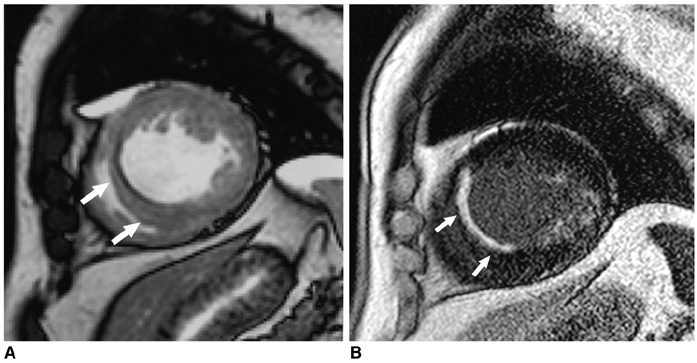
Fig. 3 The MR scan obtained in a 62-year-old male who was scheduled for coronary bypass surgery. The contrast-enhanced cine MR scan on the mid-diastolic phase (A) shows an area of low signal intensity lining the subendocardial surface of the interventricular septum (arrows). The lesion is seen as having high signal intensity on the delayed contrast-enhanced MR imaging (B).
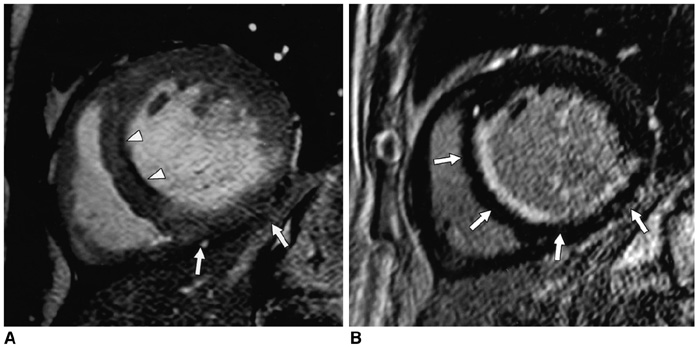
Fig. 4 The MR scan obtained in an 87-year-old male with acute myocardial infarction and a history of chronic myocardial infarction. The contrast-enhanced cine MR scan on the mid-diastolic phase (A) shows an area of high signal intensity in the inferior wall (arrows) and an area of low signal intensity lining the subendocardial surface of the interventricular septum (arrowheads). The lesions are all seen as subendocardial infarct with high signal intensity (arrows) on the delayed contrast-enhanced MR imaging (B).
Reference
-
1. Sandstede JJ. Assessment of myocardial viability by MR imaging. Eur Radiol. 2003. 13:52–61.2. Abdel-Aty H, Zagrosek A, Schulz-Menger J, Taylor AJ, Messroghli D, Kumar A, et al. Delayed enhancement and T2-weighted cardiovascular MRI differentiate acute form chronic myocardial infarction. Circulation. 2004. 109:2411–2416.3. Choi SI, Lee KW, Kang SK, Ryu WH, Lim C, Chou JH, et al. Usefulness of breath-hold T2-weighted MR imaging in patients with myocardial infarction: comparison with delayed enhancement. J Korean Soc Magn Reson Med. 2003. 7:132–136.4. Barkhausen J, Ruehm SG, Goyen M, Buck T, Laub G, Debatin JF. MR evaluation of ventricular function: True fast image with steady-state precession versus fast low angle shot cine MR imaging: Feasibility study. Radiology. 2001. 219:264–269.5. Choi B, Choe KO, Kim Y, Chung H, Chung N, Choi D. Contrast-enhanced cine magnetic resonance imaging with balanced turbo field echo in myocardial infarction. RSNA program book. 2003. 251–252.6. Chen Q, Storey P, Prased P, Li W, Mai V, Huang R, et al. Simultaneous imaging of myocardial function and viability. In : ISMRM 2003 Exhibition;7. Baer FM, Voth E, Schneider CA, Theissen P, Schicha H, Sechtem U. Comparison of low-dose dobutamine-gradient-echo magnetic resonance imaging and positron emission tomography with 18F-fluorodeoxyglucose in patients with chronic coronary artery disease. A functional and morphological approach to the detection of residual myocardial viability. Circulation. 1995. 91:1006–1015.8. Silver Malcolm D, Gotlieb A, Schoen FJ. Cardiovascular pathology. 2001. 3rd ed. Philadelphia: Churchill Livingstone;233–235.9. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, et al. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001. 218:215–223.10. Fuchs F, Laub G, Othomo K. True FISP-technical considerations and cardiovascular applications. Eur J Radiol. 2003. 46:28–32.11. Winer-Muram HT, Tann M, Aisen AM, Ford L, Jennings SG, Bretz R. Computed tomography demonstration of lipomatous metaplasia of the left ventricle following myocardial infarction. J Comput Assist Tomogr. 2004. 28:455–458.12. Oshinski JN, Yang Z, Jones JR, Mata JF, French BA. Imaging time after Gd-DTPA injection is critical in using delayed enhancement to determine infarct size accurately with magnetic resonance imaging. Circulation. 2001. 104:2838–2842.13. Thomson RJ, Kim RJ, Judd RM. MRI for the assessment of myocardial viability. J Magn Reson Imaging. 2004. 19:771–788.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Differentiation of Acute Myocardial Infarction from Chronic Myocardial Scar with MRI
- Feasibility of Three-Dimensional Balanced Steady-State Free Precession Cine Magnetic Resonance Imaging Combined with an Image Denoising Technique to Evaluate Cardiac Function in Children with Repaired Tetralogy of Fallot
- Single-Dose Gadoterate Meglumine for 3T Late Gadolinium Enhancement MRI for the Assessment of Chronic Myocardial Infarction: Intra-Individual Comparison with Conventional Double-Dose 1.5T MRI
- Usefulness of Breath-hold T2-w d T2-weighted MR Imaging in Patients with Myocardial Infarction: Comparison with Delayed Enhancement
- Advanced Cardiac MR Imaging for Myocardial Characterization and Quantification: T1 Mapping
