Posterior Lumbar Element Enforcement by Decompression Alone with Interspinous Fixation without Interbody Fusion for the Surgical Management of Lumbar Spondylolisthesis
- Affiliations
-
- 1Department of Neurosurgery, Gwangju Heemang Hospital, Gwangju, Korea
- 2Department of Neurosurgery, Chonnam National University Medical School & Research Institute of Medical Sciences, Gwangju, Korea
- 3Division of Rheumatology, Department of Internal Medicine, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Korea
- KMID: 2565273
- DOI: http://doi.org/10.3340/jkns.2024.0172
Abstract
Objective
: In degenerative lumbar spondylolisthesis, interbody fusion surgery (IFS) has long been recommended as the gold standard of surgical management. However, IFS is less recommended for high-risk patients such as the elderly because it involves extensive surgery, with a long operation time and high volumes of blood loss, which lead to marked perioperative morbidity. We report an alternative primary and salvage treatment technique for high-risk lumbar spondylolisthesis through posterior lumbar element reinforcement using interspinous fixation and decompression alone without interbody fusion.
Methods
: Plain radiographs, computed tomography scans, and magnetic resonance imaging, taken at different intervals, were used to measure local disc height (DH), vertebral body slippage (BS), and segmental motion angle (SMA). A Visual analogue scale and the Oswestry disability index (ODI) were applied pre-operation and at the last follow-up.
Results
: The local SMA decreased significantly by 3.46°±3.07°, from 10.61°±3.42° preoperatively to 7.15±3.70 at the last follow-up (p<0.001). The DH decreased from 8.61±2.88 mm preoperatively to 8.41±2.48 mm at the last follow-up (p=0.074). The BS decreased from 3.49±4.29 mm preoperatively to 3.41±4.91 mm at the last follow-up (p=0.092). None of the patients reported worsening pain or an increased ODI after surgery, and there were no surgery-related complications.
Conclusion
: Posterior lumbar element reinforcement by decompression alone with SPIRE™ fixation is an alternative primary and salvage treatment option for select patients with spondylolisthesis.
Keyword
Figure
-

Fig. 1. A : Radiological measurements in the sagittal view of the CA and lumbar disk height. Disc height was measured by (Ant-DH + Post-DH) / 2. B : Body slippage (BS) of the segmental vertebral bodies. BS was defined as the distance between the line drawn on the posterior of the two spondylolisthetic vertebral bodies in the plane sagittal view. CA : Cobb angle, Ant-DH : disc height anterior, Post-DH : disc height posterior.

Fig. 2. Intraoperative photographs. A : A small hole was mad into the interspinous ligament at the target level using right angle-Kelly forceps. B : The spinous process construct is fixed to the insertion instrument and inserted. One half of the construct is placed on each side of the spinous processes, with the sliding post lying in the space between the spinous processes. C : Hand-held compression instruments are used to clamp the plates toward each other, driving the spikes into the bone. D : A locking screw is inserted and tightened to a predetermined torque.

Fig. 3. Interspinous fixation device (SPIRE; Medtronic, Dublin, Ireland) made up of two titanium plates with spikes.

Fig. 4. Case illustration. A and B : Radiological findings of the lumbar spine show an L 4/5 spondylolisthesis grade I. C and D : The disc height (DH) and body slippage (BS) were measured as 11.2 mm and 6.3 mm, respectively, and the segmental motion angle (SMA) was measured as 10.4°. E : Postoperative lateral whole-spine lateral radiography. F and G : At the last follow-up, DH and BS were measured as 9.0 mm and 6.2 mm, respectively, and the SMA was measured as 8.5°.
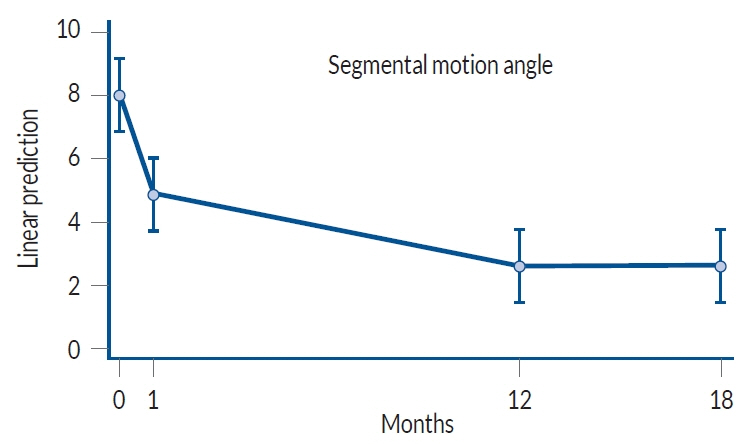
Fig. 5. Changes in the segmental motion angle recorded preoperatively, immediately after surgery, at 1 year post-operatively, and at the last follow-up.
Reference
-
References
1. Austevoll IM, Hermansen E, Fagerland MW, Storheim K, Brox JI, Solberg T, et al. Decompression with or without fusion in degenerative lumbar spondylolisthesis. N Engl J Med. 385:526–538. 2021.
Article2. Chan AK, Sharma V, Robinson LC, Mummaneni PV. Summary of guidelines for the treatment of lumbar spondylolisthesis. Neurosurg Clin N Am. 30:353–364. 2019.
Article3. DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 16:130–139. 2008.
Article4. Kaibara T, Karahalios DG, Porter RW, Kakarla UK, Reyes PM, Choi SK, et al. Biomechanics of a lumbar interspinous anchor with transforaminal lumbar interbody fixation. World Neurosurg. 73:572–577. 2010.
Article5. Karahalios DG, Kaibara T, Porter RW, Kakarla UK, Reyes PM, Baaj AA, et al. Biomechanics of a lumbar interspinous anchor with anterior lumbar interbody fusion. J Neurosurg Spine. 12:372–380. 2010.
Article6. Kim HJ, Bak KH, Chun HJ, Oh SJ, Kang TH, Yang MS. Posterior interspinous fusion device for one-level fusion in degenerative lumbar spine disease : comparison with pedicle screw fixation - preliminary report of at least one year follow up. J Korean Neurosurg Soc. 52:359–364. 2012.
Article7. Koslosky E, Gendelberg D. Classification in brief: the Meyerding classification system of spondylolisthesis. Clin Orthop Relat Res. 478:1125–1130. 2020.
Article8. Lin PM. Posterior lumbar interbody fusion technique: complications and pitfalls. Clin Orthop Relat Res. 193:90–102. 1985.9. Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 1:2–18. 2015.10. Okuda S, Oda T, Miyauchi A, Haku T, Yamamoto T, Iwasaki M. Surgical outcomes of posterior lumbar interbody fusion in elderly patients. J Bone Joint Surg Am. 88:2714–2720. 2006.
Article11. Steiger F, Becker HJ, Standaert CJ, Balague F, Vader JP, Porchet F, et al. Surgery in lumbar degenerative spondylolisthesis: indications, outcomes and complications. A systematic review. Eur Spine J. 23:945–973. 2014.
Article12. Stillerman CB, Schneider JH, Gruen JP. Evaluation and management of spondylolysis and spondylolisthesis. Clin Neurosurg. 40:384–415. 1993.13. Wang JC, Haid RW Jr, Miller JS, Robinson JC. Comparison of CD HORIZON SPIRE spinous process plate stabilization and pedicle screw fixation after anterior lumbar interbody fusion: invited submission from the Joint Section Meeting on Disorders of the Spine and Peripheral Nerves, March 2005. J Neurosurg Spine. 4:132–136. 2006.
Article14. Wang JC, Spenciner D, Robinson JC. SPIRE spinous process stabilization plate: biomechanical evaluation of a novel technology: invited submission from the joint section meeting on disorders of the spine and peripheral nerves, March 2005. J Neurosurg Spine. 4:160–164. 2006.
Article15. Watters WC 3rd, Bono CM, Gilbert TJ, Kreiner DS, Mazanec DJ, Shaffer WO, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 9:609–614. 2009.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Lumbar Interbody Fusion and Graf Band Fixation for Lumbar Isthmic Spondylolisthesis
- Intertransverse Fusion in Spondylolisthesis: Report of a Case
- A Comparison of Posterolateral and Posterior Interbody Fusion in the Surgical Treatment of Lumbar Spondylolisthesis
- Comparison between Posterior Lumbar Interbody Fusion with Pedicle Screw Fixation and Posterolateral Fusion with Pedicle Screw Fixation in Spondylolytic Spondylolisthesis in Adults
- Posterior Lumbar Interbody Fusion
