Supraorbital Approaches for Anterior Skull Base and Parasellar Lesions: Insights From a Single-Center Experience
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea
- KMID: 2558435
- DOI: http://doi.org/10.14791/btrt.2024.0026
Abstract
- Background
Modern neurosurgery has undergone significant evolution to include minimally inva-sive procedures, with the supraorbital approach (SOA) being a prime example. In this study, we aim to explore the surgical techniques and outcomes of this approach in the surgical treatment of frontal lobe, anterior skull base, and parasellar lesions.
Methods
This study included 33 patients aged 36–83 years who underwent surgery using the SOA for lesions in the inferior frontal lobe, anterior skull base, and parasellar area between 2015 and 2024. There were 25 cases of meningioma, 2 cases of brain abscess, 2 cases of glioma, and one case each of craniopharyngioma, hemangioma, metastasis, and Rathke’s cleft cyst. The medical data and follow-up results were retrospectively analyzed.
Results
The mean size of lesion was 3.38±3.05 cm. The mean follow-up period was 48.8 months. Gross total resection was achieved in 25 patients (75.8%). There were no perioperative deaths, cases of cerebrospinal fluid rhinorrhea, or infections. Two cases of morbidity were reported as complications: one case of delayed intracerebral hemorrhage and one case of infarction due to vascular injury. All patients exhibited satisfactory cosmetic results.
Conclusion
In comparison to the conventional pterional approach, the SOA represents a safe and effective keyhole method for the removal of both extra-axial and intra-axial skull base tumors. This is particularly beneficial for lesions in the orbitofrontal region and parasellar area, as it allows for minimal disruption of normal brain parenchyma. Moreover, the SOA promotes a swift recovery and short hospital stay. Additionally, the SOA yields superior cosmetic results, including the prevention of temporalis muscle atrophy.
Figure
-
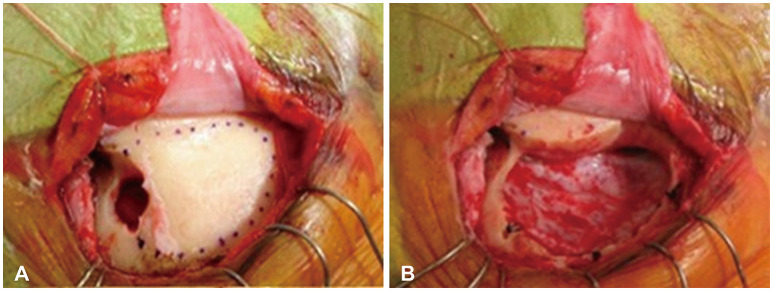
Fig. 1 Intraoperative close-up of MacCarty’s keyhole. A: Intraoperative close-up of MacCarty’s keyhole after reflection of periosteal flap and anterior portion of temporlis muscle. B: Removal of the bone flap exposes the dura mater.
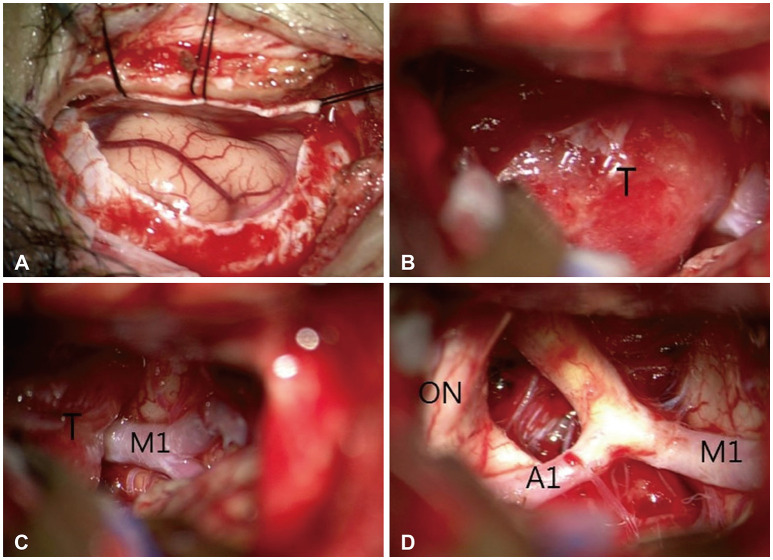
Fig. 2 Intraoperative microscopic images with a surgical microscope during surgery on olfactory groove meningioma using the supraorbital approach approach. A: C-shape durotomy was made after supraorbital craniotomy. B and C: Exposure of a tumor (T) mass after frontal lobe retraction. D: After removal of tumor, exposure of optic nerve (ON), anterior cerebral artery (A1), and middle cerebral artery (M1).
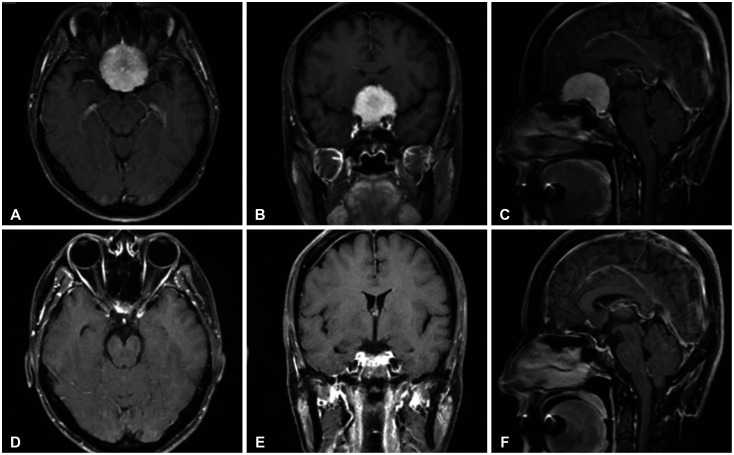
Fig. 3 Preoperative MRI, including axial (A), coronal (B), and sagittal (C) views, demonstrates a homogeneously enhancing large frontal-based tumor measuring 4.1×3.1 cm with suprasellar extension, suggestive of an olfactory groove meningioma. Postoperative MRI, including axial (D), coronal (E), and sagittal (F) views, demonstrate complete tumor removal.
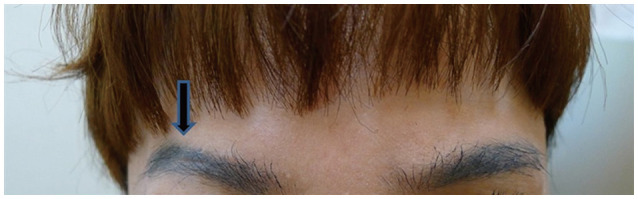
Fig. 4 A photograph taken 6 months after the operation. The arrow points to the postoperative scar.

Fig. 5 Intraoperative surgical images. A: To enhance exposure of the temporal area, the skin incision was extended from the right eyebrow to the lateral orbital rim, avoiding the supraorbital nerve (black arrow: supraorbital nerve direction). B: The image depicts the skull bone exposed following a skin incision. C: After opening the dura, the proximal Sylvian fissure was opened to minimize brain retraction. D: After tumor removal, the tumor was found to be tightly adhered to the right optic nerve. The tumor at the temporal pole was also adequately excised. Arrow, supraorbital notch; F, frontal; T, temporal; Tm, tumor; SV, Sylvian vein; LON, left optic nerve; RON, right optic nerve; ICA, internal carotid artery.
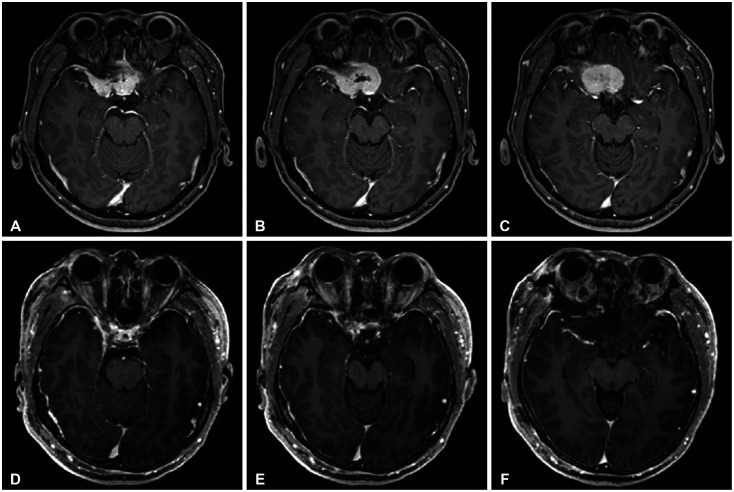
Fig. 6 Pre- and postoperative MRI images. A-C: Preoperative MRI images; A broad-based extra-axial enhancing lesion, measuring approximately 3.6×2.1×3.1 cm, is primarily located on the right side of the anterior cranial fossa, involving the planum sphenoidale through the tuberculum sella and extending to the right sphenoid ridge, with encasement of the right orbital apex. D-F: The MRI images post-tumor removal show that the tumor located at the sphenoid ridge has also been excised.
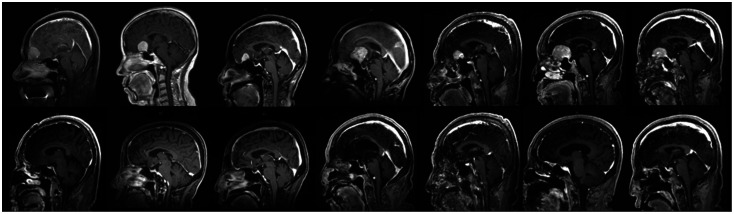
Fig. 7 Representative preoperative sagittal contrast-enhanced T1-weighted MR images obtained in 7 patients with olfactory groove meningiomas included in this study (upper) and 3 cases overlying the cribriform plate and anterior to the insertion of the sphenoid sinus. Lower images indicate MRI images after the removal of a tumor.
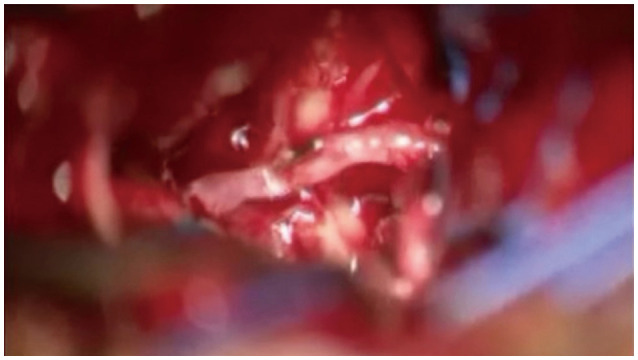
Fig. 8 This image depicts the control of arterial bleeding with mini-hemoclips, which was caused by cutting the feeding artery from the anterior cerebral artery to the tumor during the removal of an olfactory groove meningioma.
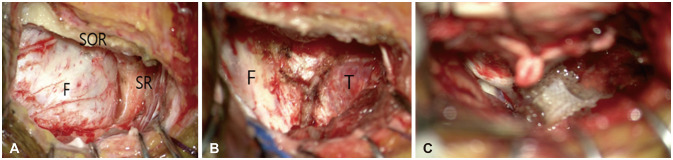
Fig. 9 Intraoperative surgical images for temporal pole meningioma. A: The image illustrates that, following the removal of the frontal bone, the frontal dura was exposed utilizing a right supraorbital approach. To expose the temporal pole, additional drilling of the sphenoid ridge (SR) is necessary. B: After the removal of the sphenoid ridge, the temporal dura was additionally exposed. C: This image demonstrates that following the resection of the tumor, the tumor located at the temporal pole was completely excised. F, frontal; T, temporal; SOR, superior orbital rim; SR, sphenoid ridge.
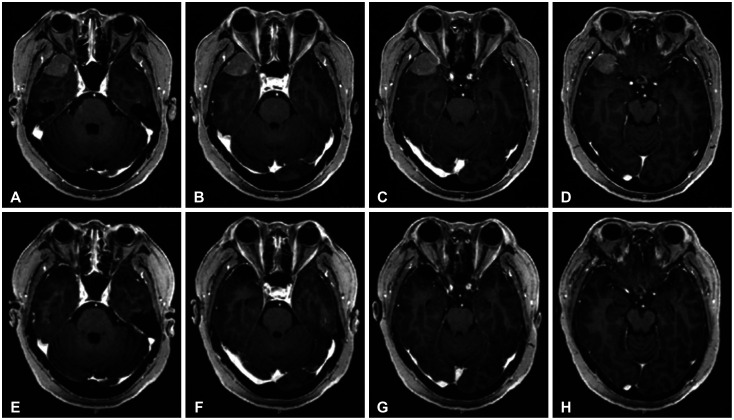
Fig. 10 Preoperative MRI images (A-D) show a homogeneously enhancing mass measuring approximately 2.9×2.4×2.2 cm in the right temporal convexity. Postoperative MRI images (E-H) show complete tumor removal using the supraorbital approach.
Reference
-
1. Adappa ND, Lee JY, Chiu AG, Palmer JN. Olfactory groove meningioma. Otolaryngol Clin North Am. 2011; 44:965–980. PMID: 21819883.2. Rychen J, Croci D, Roethlisberger M, Nossek E, Potts M, Radovanovic I, et al. Minimally invasive alternative approaches to pterional craniotomy: a systematic review of the literature. World Neurosurg. 2018; 113:163–179. PMID: 29452317.3. Gazzeri R, Nishiyama Y, Teo C. Endoscopic supraorbital eyebrow approach for the surgical treatment of extraaxialand intraaxial tumors. Neurosurg Focus. 2014; 37:E20.4. Robinow ZM, Peterson C, Waldau B, Shahlaie K. Supraorbital keyhole craniotomy via eyebrow incision: a systematic review and meta-analysis. World Neurosurg. 2022; 158:e509–e542. PMID: 34775096.5. Youngerman BE, Shtayer L, Gerges MM, Larsen AG, Tomasiewicz HC, Schwartz TH. Eyebrow supraorbital keyhole craniotomy for olfactory groove meningiomas with endoscope assistance: case series and systematic review of extent of resection, quantification of postoperative frontal lobe injury, anosmia, and recurrence. Acta Neurochir (Wien). 2021; 163:101–112. PMID: 32888076.6. Reisch R, Perneczky A, Filippi R. Surgical technique of the supraorbital key-hole craniotomy. Surg Neurol. 2003; 59:223–227. PMID: 12681560.7. Zumofen DW, Rychen J, Roethlisberger M, Taub E, Kalbermatten D, Nossek E, et al. A review of the literature on the transciliary supraorbital keyhole approach. World Neurosurg. 2017; 98:614–624. PMID: 27989977.8. Pepper JP, Hecht SL, Gebarski SS, Lin EM, Sullivan SE, Marentette LJ. Olfactory groove meningioma: discussion of clinical presentation and surgical outcomes following excision via the subcranial approach. Laryngoscope. 2011; 121:2282–2289. PMID: 21994142.9. Sade B, Lee JH. High incidence of optic canal involvement in tuberculum sellae meningiomas: rationale for aggressive skull base approach. Surg Neurol. 2009; 72:118–123. PMID: 19147207.10. Chen HC, Tzaan WC. Microsurgical supraorbital keyhole approach to the anterior cranial base. J Clin Neurosci. 2010; 17:1510–1514. PMID: 20817469.11. Tatarli N, Ceylan D, Şeker A, Solmaz B, Çavdar S, Kiliç T. The supraorbital keyhole approach. J Craniofac Surg. 2015; 26:1663–1667. PMID: 26114521.12. Eroglu U, Shah K, Bozkurt M, Kahilogullari G, Yakar F, Dogan İ, et al. Supraorbital keyhole approach: lessons learned from 106 operative cases. World Neurosurg. 2019; 124:e667–e674. PMID: 30659969.13. Iacoangeli M, Nocchi N, Nasi D, DI Rienzo A, Dobran M, Gladi M, et al. Minimally invasive supraorbital key-hole approach for the treatment of anterior cranial fossa meningiomas. Neurol Med Chir (Tokyo). 2016; 56:180–185. PMID: 26804334.14. Wiedemayer H, Sandalcioglu IE, Wiedemayer H, Stolke D. The supraorbital keyhole approach via an eyebrow incision for resection of tumors around the sella and the anterior skull base. Minim Invasive Neurosurg. 2004; 47:221–225. PMID: 15346318.15. Wilson DA, Duong H, Teo C, Kelly DF. The supraorbital endoscopic approach for tumors. World Neurosurg. 2014; 82:e243–e256. PMID: 23395805.16. Bander ED, Pandey A, Yan J, Giantini-Larsen AM, Schwartz A, Estin J, et al. Olfactory groove meningiomas: supraorbital keyhole versus orbitofrontal, frontotemporal, or bifrontal approaches. J Neurosurg. 2023; 140:1568–1575. PMID: 38064694.17. Cai M, Hou B, Luo L, Zhang B, Guo Y. Trans-eyebrow supraorbital keyhole approach to tuberculum sellae meningiomas: a series of 30 cases with long-term visual outcomes and recurrence rates. J Neurooncol. 2019; 142:545–555. PMID: 30796744.18. Singh H, Essayed WI, Jada A, Moussazadeh N, Dhandapani S, Rote S, et al. Contralateral supraorbital keyhole approach to medial optic nerve lesions: an anatomoclinical study. J Neurosurg. 2017; 126:940–944. PMID: 27257841.19. Troude L, Boucekine M, Baucher G, Farah K, Boissonneau S, Fuentes S, et al. Ipsilateral vs controlateral approach in tuberculum sellae meningiomas surgery: a retrospective comparative study. Neurosurg Rev. 2021; 44:3581–3591. PMID: 33890190.20. Beseoglu K, Lodes S, Stummer W, Steiger HJ, Hänggi D. The transorbital keyhole approach: early and long-term outcome analysis of approach-related morbidity and cosmetic results. J Neurosurg. 2011; 114:852–856. PMID: 21029037.
