Outcomes of partially covered self-expandable metal stents with different uncovered lengths in endoscopic ultrasound-guided hepaticogastrostomy: a Japanese retrospective study
- Okamoto T
 1
1 - Sasaki T1
- Takeda T1
- Hirai T1
- Ishitsuka T1
- Yamada M1
- Nakagawa H1
- Mie T1
- Furukawa T1
- Kasuga A1
- Ozaka M1
- Sasahira N1
- Affiliations
-
- 1Department of Hepato-Biliary-Pancreatic Medicine, Cancer Institute Hospital of Japanese Foundation for Cancer Research, Tokyo, Japan
- KMID: 2558109
- DOI: http://doi.org/10.5946/ce.2023.142
Abstract
- Background/Aims
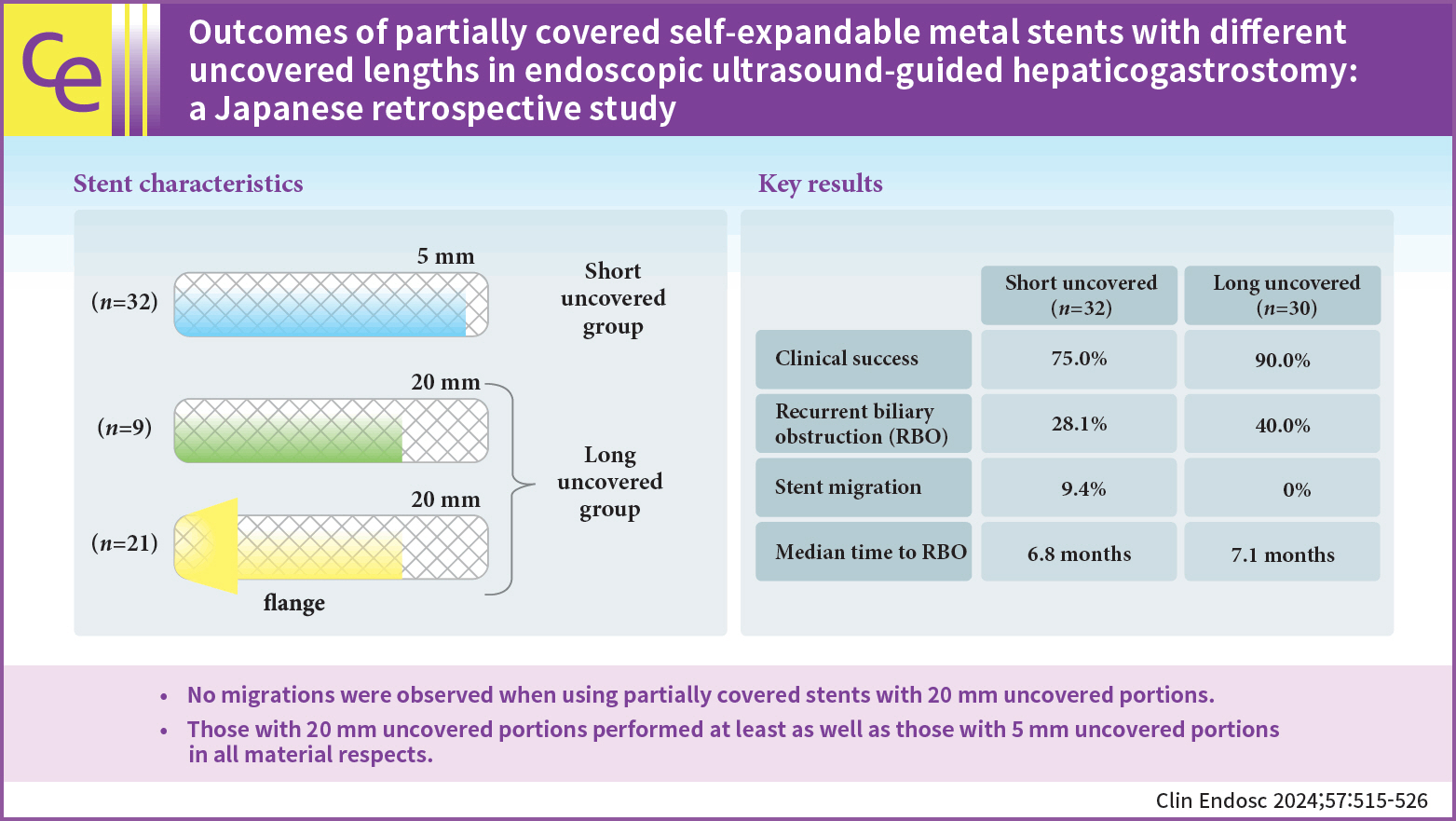
The optimal length of the uncovered portion of partially covered self-expandable metal stents (PCSEMSs) used in endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) remains unclear. This study investigated the safety and efficacy of PCSEMSs with different uncovered lengths, with a focus on stent migration and time to recurrent biliary obstruction (RBO).
Methods
Outcomes of patients undergoing EUS-HGS using PCSEMSs with 5-mm and 20-mm uncovered portions at our institution from January 2016 to December 2021 were compared.
Results
Sixty-two patients underwent EUS-HGS using PCSEMS (5/20-mm uncovered portions: 32/30). Stent migration occurred only in the 5-mm group. There were no differences in RBO rates (28.1% vs. 40.0%) or median time to RBO (6.8 vs. 7.1 months) between the two groups. Median overall survival (OS) was longer in the 20-mm group (3.1 vs. 4.9 months, p=0.037) due to the higher number of patients that resumed chemotherapy after EUS-HGS (56.7% vs. 28.1%, p=0.029). Good performance status, absence of hepatic metastases, and chemotherapy after EUS-HGS were independent predictors of longer OS.
Conclusions
No migration was observed in patients treated with PCSEMS with 20-mm uncovered portions. Patients treated with PCSEMS with 20-mm uncovered portions performed at least as well as those treated with 5-mm uncovered portions in all material respects.
Keyword
Figure
-
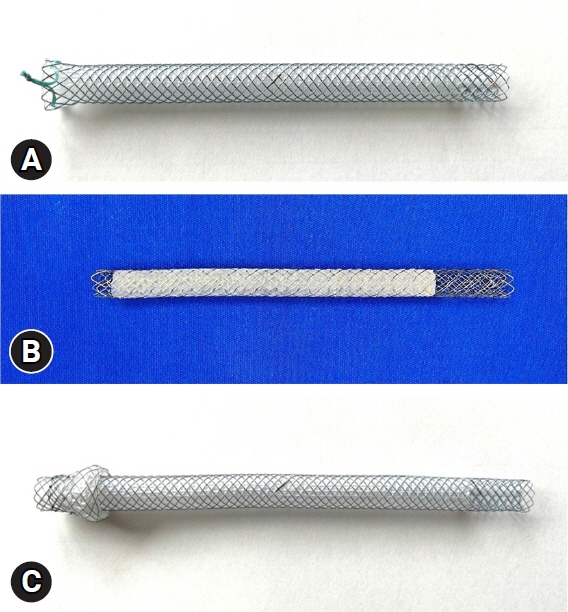
Fig. 1. (A) Niti-S Biliary S-type Stent, a partially covered self-expandable metal stent (PCSEMS) with a 5-mm uncovered portion on the liver side (right) and a short, 2-mm flare on the stomach side (left). (B) Modified EGIS Biliary Stent, Double Covered, a PCSEMS modified to extend the short uncovered portion on the liver side (right) to 20 mm. (C) Niti-S S-type Spring Stopper Stent, a PCSEMS with a 20-mm uncovered portion on the liver side (right) and a flange on the stomach side (left).
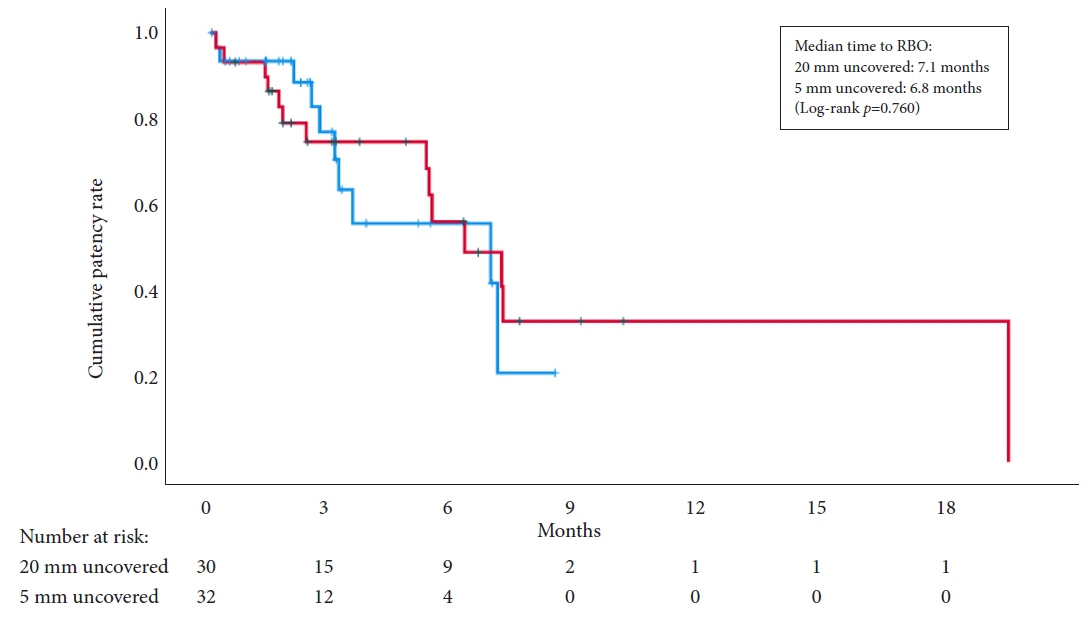
Fig. 2. Kaplan-Meier curve for time to recurrent biliary obstruction (RBO), stratified by length of the uncovered portion.
Cited by 1 articles
-
Migration of covered expandable metal stents after endoscopic ultrasound-guided hepaticogastrostomy: stent covering versus stent design?
Todd H. Baron
Clin Endosc. 2024;57(4):471-472. doi: 10.5946/ce.2024.158.
Reference
-
1. Isayama H, Nakai Y, Itoi T, et al. Clinical practice guidelines for safe performance of endoscopic ultrasound/ultrasonography-guided biliary drainage: 2018. J Hepatobiliary Pancreat Sci. 2019; 26:249–269.
Article2. van der Merwe SW, van Wanrooij RL, Bronswijk M, et al. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2022; 54:185–205.
Article3. Khashab MA, Messallam AA, Penas I, et al. International multicenter comparative trial of transluminal EUS-guided biliary drainage via hepatogastrostomy vs. choledochoduodenostomy approaches. Endosc Int Open. 2016; 4:E175–E181.
Article4. Ochiai K, Fujisawa T, Ishii S, et al. Risk factors for stent migration into the abdominal cavity after endoscopic ultrasound-guided hepaticogastrostomy. J Clin Med. 2021; 10:3111.
Article5. Martins FP, Rossini LG, Ferrari AP. Migration of a covered metallic stent following endoscopic ultrasound-guided hepaticogastrostomy: fatal complication. Endoscopy. 2010; 42 Suppl 2:E126–E127.
Article6. Okuno N, Hara K, Mizuno N, et al. Stent migration into the peritoneal cavity following endoscopic ultrasound-guided hepaticogastrostomy. Endoscopy. 2015; 47 Suppl 1 UCTN:E311.
Article7. Nakai Y, Isayama H, Yamamoto N, et al. Safety and effectiveness of a long, partially covered metal stent for endoscopic ultrasound-guided hepaticogastrostomy in patients with malignant biliary obstruction. Endoscopy. 2016; 48:1125–1128.
Article8. Nakai Y, Sato T, Hakuta R, et al. Long-term outcomes of a long, partially covered metal stent for EUS-guided hepaticogastrostomy in patients with malignant biliary obstruction (with video). Gastrointest Endosc. 2020; 92:623–631.
Article9. Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010; 71:446–454.10. Isayama H, Hamada T, Yasuda I, et al. TOKYO criteria 2014 for transpapillary biliary stenting. Dig Endosc. 2015; 27:259–264.11. Asai S, Takeshita K, Ichinona T, et al. A novel partially covered metallic stent with a 20-mm long distal bare portion for EUS-guided hepaticogastrostomy. VideoGIE. 2021; 6:322–324.
Article12. Ishii S, Isayama H, Sasahira N, et al. A pilot study of Spring Stopper Stents: novel partially covered self-expandable metallic stents with anti-migration properties for EUS-guided hepaticogastrostomy. Endosc Ultrasound. 2023; 12:266–272.
Article13. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009; 45:228–247.
Article14. Artifon EL, Marson FP, Gaidhane M, et al. Hepaticogastrostomy or choledochoduodenostomy for distal malignant biliary obstruction after failed ERCP: is there any difference? Gastrointest Endosc. 2015; 81:950–959.
Article15. Cho DH, Lee SS, Oh D, et al. Long-term outcomes of a newly developed hybrid metal stent for EUS-guided biliary drainage (with videos). Gastrointest Endosc. 2017; 85:1067–1075.
Article16. De Cassan C, Bories E, Pesenti C, et al. Use of partially covered and uncovered metallic prosthesis for endoscopic ultrasound-guided hepaticogastrostomy: results of a retrospective monocentric study. Endosc Ultrasound. 2017; 6:329–335.
Article17. Miyano A, Ogura T, Yamamoto K, et al. Clinical impact of the intra-scope channel stent release technique in preventing stent migration during EUS-guided hepaticogastrostomy. J Gastrointest Surg. 2018; 22:1312–1318.
Article18. Emmanuel J, Omar H, See LT. Endoscopic ultrasound-guided hepaticogastrostomy using a partially covered metal stent in patients with malignant biliary obstruction after failed endoscopic retrograde cholangiopancreatography. JGH Open. 2020; 4:1059–1064.
Article19. Yamamura M, Ogura T, Ueno S, et al. Partially covered self-expandable metal stent with antimigratory single flange plays important role during EUS-guided hepaticogastrostomy. Endosc Int Open. 2022; 10:E209–E214.
Article20. Paik WH, Park DH. Outcomes and limitations: EUS-guided hepaticogastrostomy. Endosc Ultrasound. 2019; 8(Suppl 1):S44–S49.
Article21. Ogura T, Yamamoto K, Sano T, et al. Stent length is impact factor associated with stent patency in endoscopic ultrasound-guided hepaticogastrostomy. J Gastroenterol Hepatol. 2015; 30:1748–1752.
Article22. Wang K, Zhu J, Xing L, et al. Assessment of efficacy and safety of EUS-guided biliary drainage: a systematic review. Gastrointest Endosc. 2016; 83:1218–1227.
Article23. Bories E, Pesenti C, Caillol F, et al. Transgastric endoscopic ultrasonography-guided biliary drainage: results of a pilot study. Endoscopy. 2007; 39:287–291.
Article24. Paik WH, Park DH, Choi JH, et al. Simplified fistula dilation technique and modified stent deployment maneuver for EUS-guided hepaticogastrostomy. World J Gastroenterol. 2014; 20:5051–5059.
Article25. Ogura T, Kurisu Y, Masuda D, et al. Novel method of endoscopic ultrasound-guided hepaticogastrostomy to prevent stent dysfunction. J Gastroenterol Hepatol. 2014; 29:1815–1821.
Article26. Panpimanmas S, Ratanachu-ek T. Endoscopic ultrasound-guided hepaticogastrostomy for advanced cholangiocarcinoma after failed stenting by endoscopic retrograde cholangiopancreatography. Asian J Surg. 2013; 36:154–158.
Article27. Attasaranya S, Netinasunton N, Jongboonyanuparp T, et al. The spectrum of endoscopic ultrasound intervention in biliary diseases: a single center’s experience in 31 cases. Gastroenterol Res Pract. 2012; 2012:680753.
Article28. Kim TH, Kim SH, Oh HJ, et al. Endoscopic ultrasound-guided biliary drainage with placement of a fully covered metal stent for malignant biliary obstruction. World J Gastroenterol. 2012; 18:2526–2532.
Article29. Ramírez-Luna MA, Téllez-Ávila FI, Giovannini M, et al. Endoscopic ultrasound-guided biliodigestive drainage is a good alternative in patients with unresectable cancer. Endoscopy. 2011; 43:826–830.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Migration of covered expandable metal stents after endoscopic ultrasound-guided hepaticogastrostomy: stent covering versus stent design?
- Stepwise Algorithmic Approach to Endoscopic Removal of Biliary Partially Covered and Uncovered Self-Expanding Metal Stents (with Videos)
- Advances in self-expandable metal stents for endoscopic ultrasound-guided interventions
- Follow-up computed tomography can prevent stent migration after endoscopic ultrasound-guided hepaticogastrostomy
- Management of Occluded Biliary Uncovered Metal Stents: Covered Self Expandable Metallic Stent vs. Uncovered Self Expandable Metallic Stent
