Optimizing genicular nerve chemical ablation
- Rocha-Romero A
 1
1 - Ng TKT2,3,4,6,7,
- Lam KHS3,4,5,6,7
- Affiliations
-
- 1Department of Anesthesia and Pain Medicine, National Rehabilitation Center, San José, Costa Rica
- 2Frankston Pain Management, Melbourne, Australia
- 3The Faculty of Medicine, The University of Hong Kong, Hong Kong
- 4The Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong
- 5The Board of Clinical Research, The Hong Kong Institute of Musculoskeletal Medicine, Hong Kong
- 6Center for Regional Anesthesia and Pain Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan
- 7Center for Regional Anesthesia and Pain Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan
- 8Department of Anaesthesia and Operating Theatre Services, Tuen Mun Hospital, Hong Kong
- 9Department of Anaesthesia, Boxhill Hospital, Melbourne, Australia
- KMID: 2557731
- DOI: http://doi.org/10.3344/kjp.24021
Figure
-
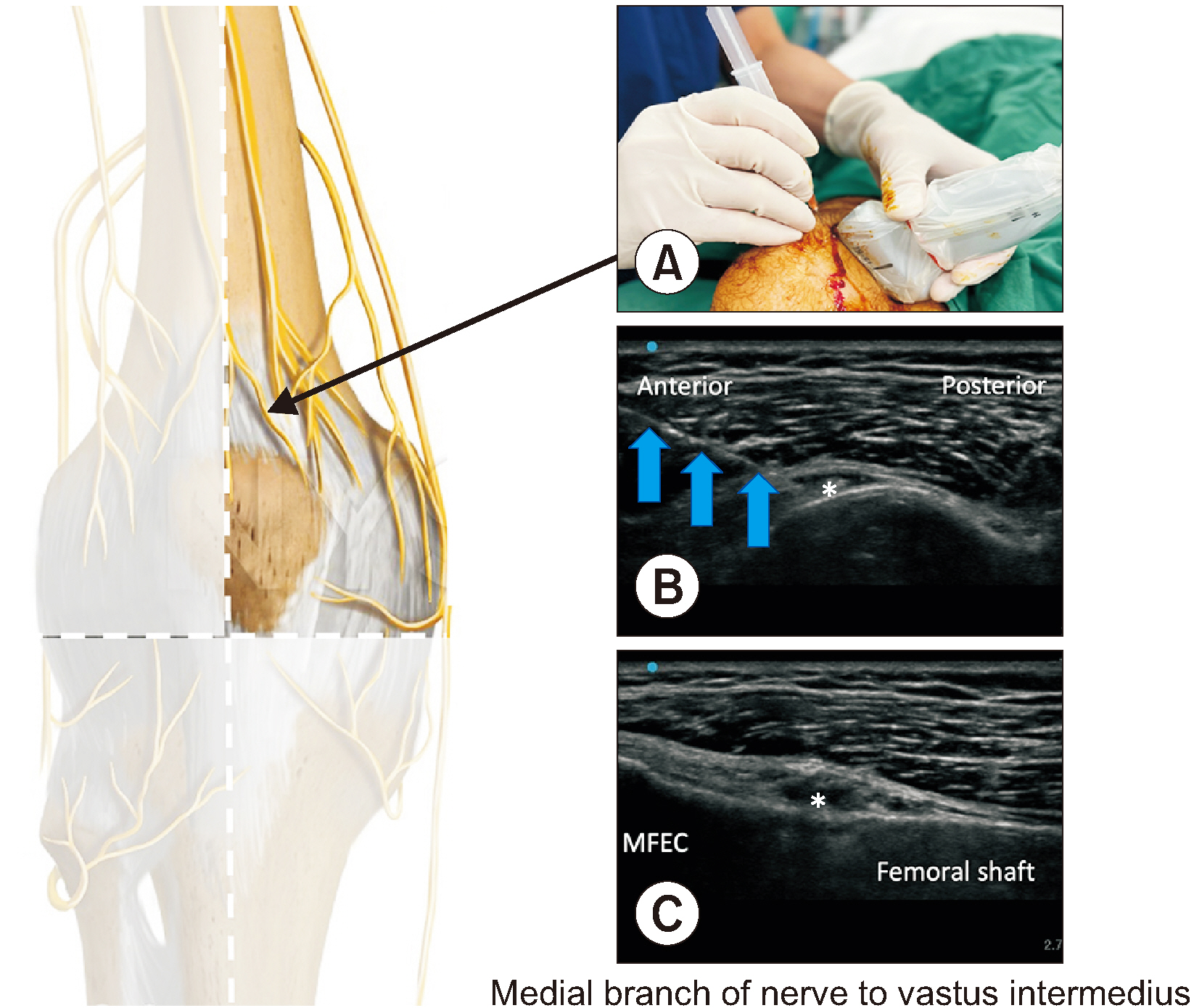
Fig. 1 Medial branch of nerve to vastus intermedius. Fig. 1A indicates the probe position. Fig. 1B is transverse view of ultrasound image. Fig. 1C is coronal view. Note the importance of bi-plane confirmation of this final needle position. The needle tip is at around 30% of the anterior cortex of femoral shaft. MFEC: medial femoral epicondyle, Asterisk: final needle position with phenol, Blue arrows: needle.
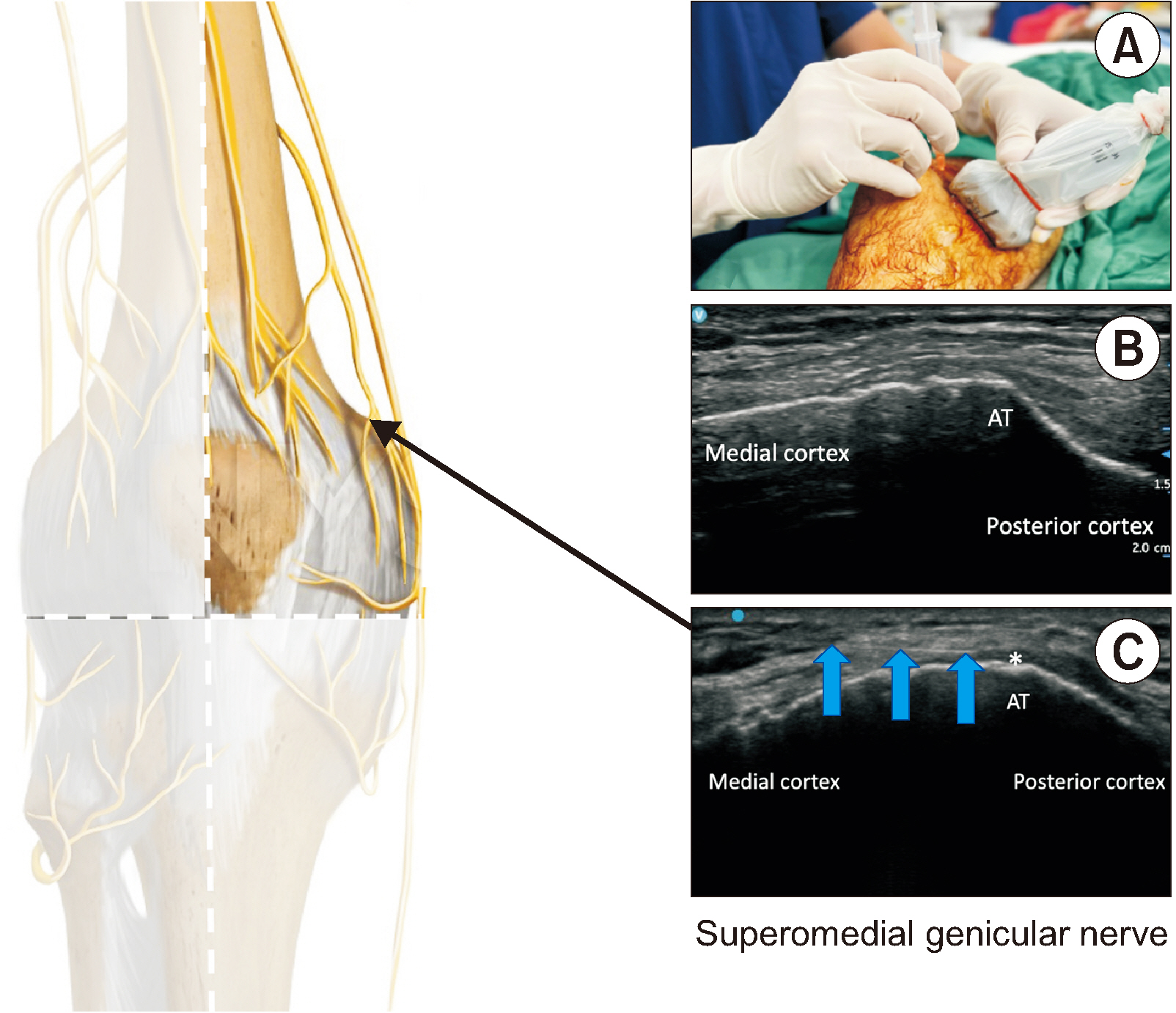
Fig. 2 Superomedial genicular nerve. Fig. 2A indicates the probe position. Fig. 2B is transverse view of the adductor tubercle (AT) as the landmark. Fig. 2C showing that the actual plane of needle insertion is slightly proximal to the AT until the AT becomes less sharp. This modification can reduce the risk of adductor tendon irritation by phenol. Asterisk: final needle position with phenol, Blue arrows: needle.
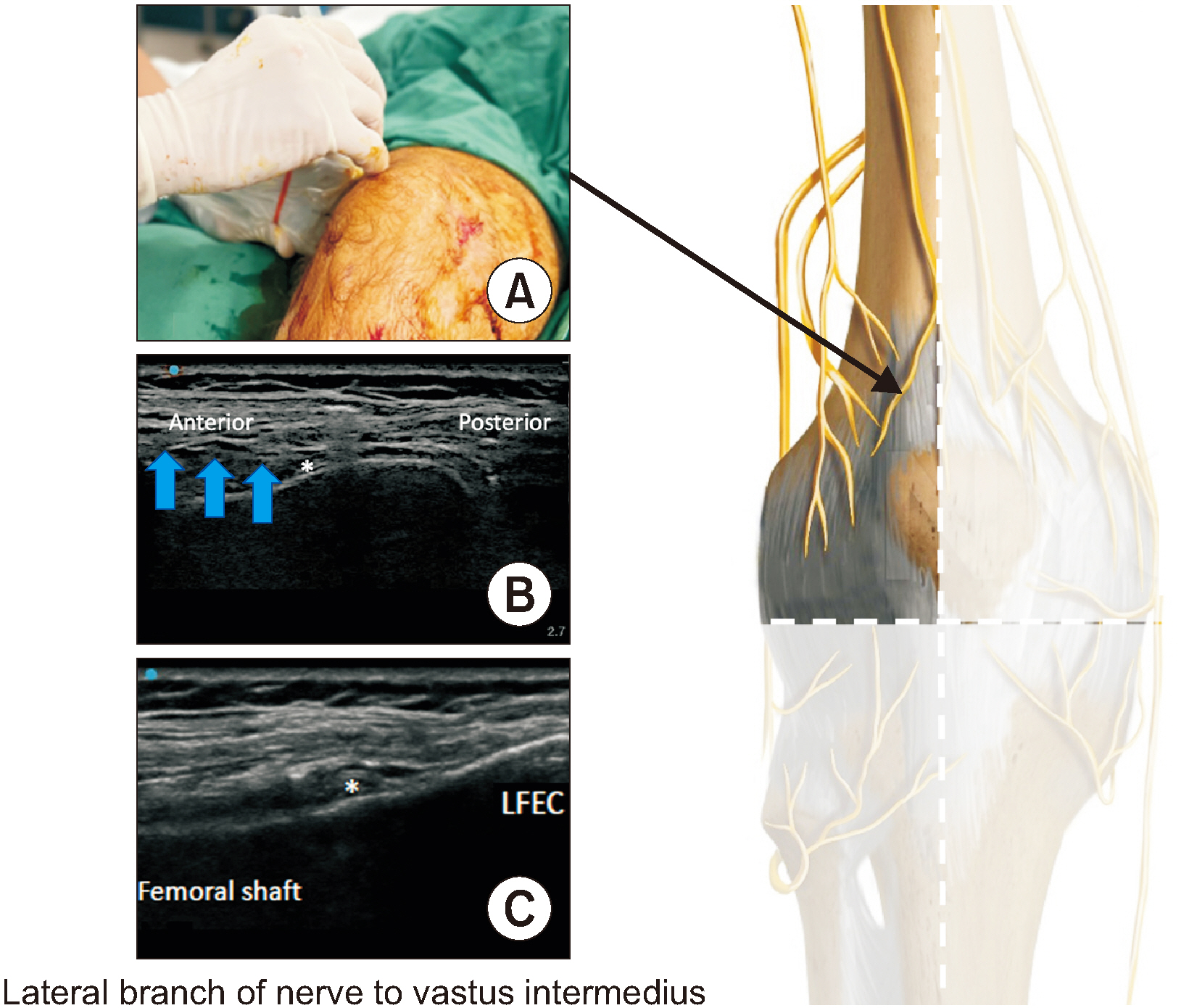
Fig. 3 Lateral branch of nerve to vastus intermedius. Fig. 3A indicates the probe position. Fig. 3B is transverse view of ultrasound image. Fig. 3C is coronal view. It is a mirror image of that of the medial branch of nerve to vastus intermedius. LFEC: lateral femoral epicondyle, Asterisk: final needle position with phenol, Blue arrows: needle.
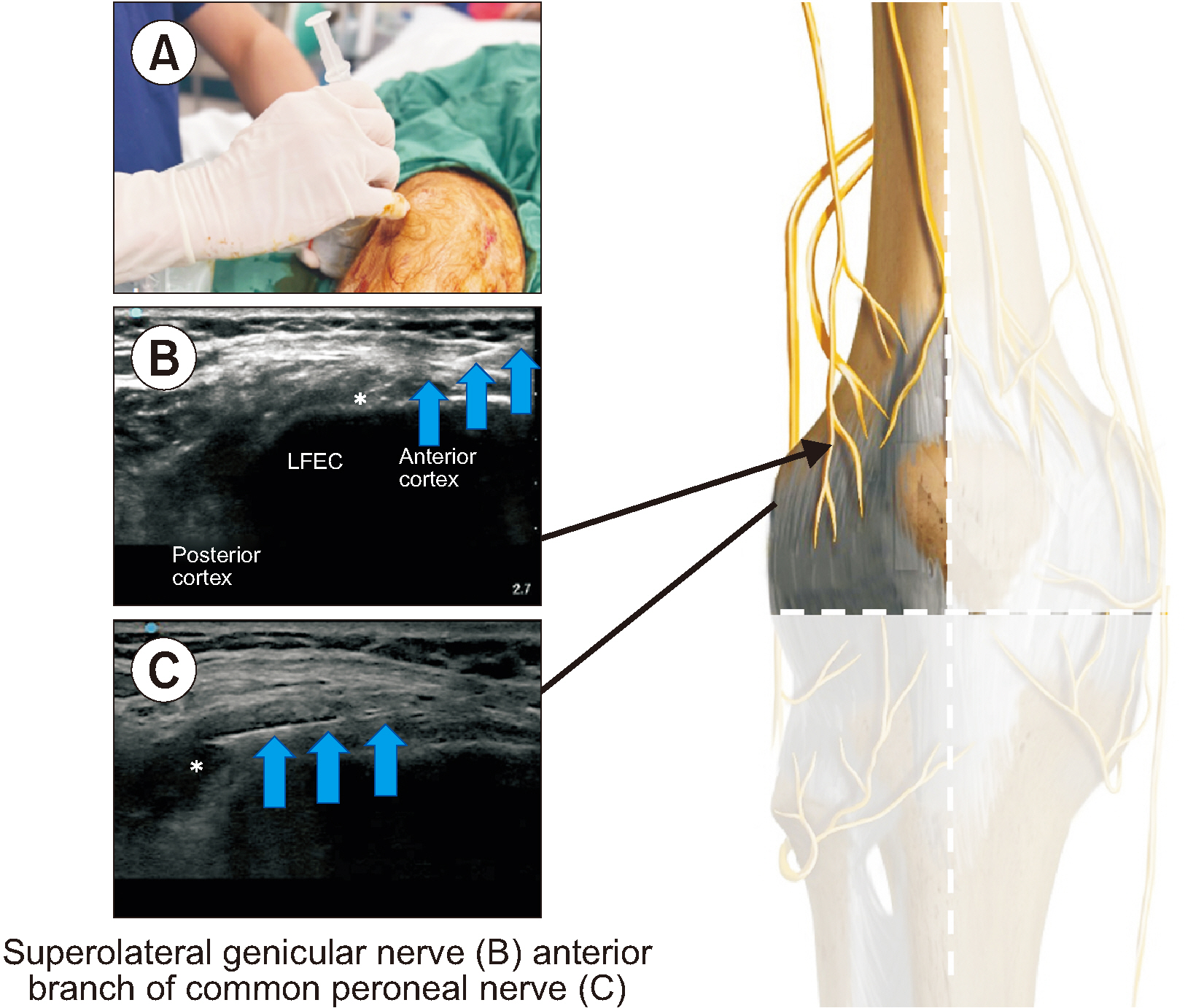
Fig. 4 Superolateral genicular nerve and anterior branch of common peroneal nerve. Fig. 4A indicates the probe position. Fig. 4B is transverse view of ultrasound image for the superolateral genicular nerve. Fig. 4C showing that the needle trajectory is redirected to the posterior cortex for the anterior branch of common peroneal nerve, this distal branch is not depicted in the diagram because is posterior. The landmark is the lateral femoral epicondyle (LFEC). Blue arrows: needle, Asterisk: final needle position with phenol.
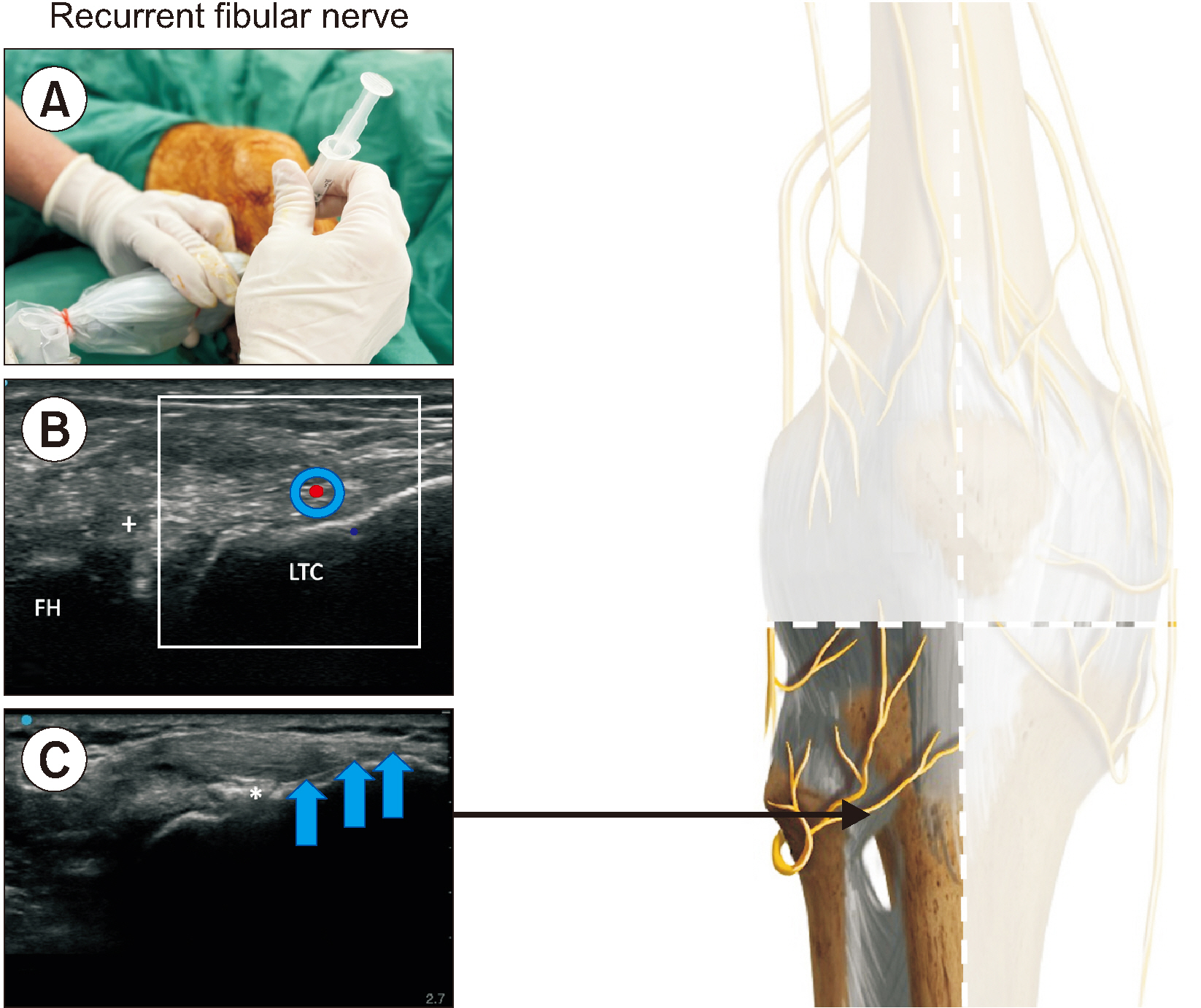
Fig. 5 Recurrent fibular nerve. Fig. 5A indicates the probe position. Fig. 5B is doppler image of transverse view depicting the anterior tibial recurrent artery. Fig. 5C showing that the needle trajectory is along the bony surface of the lateral tibial condyle (LTC) to minimize the chance of phenol extravasation to the superficial structure, particularly skin. The final needle position is around the midway of the LTC. FH: fibular head, Asterisk: final needle position with phenol, Blue arrows: needle, (+): anterior tibiofibular ligament, Red dot: anterior tibial recurrent artery.
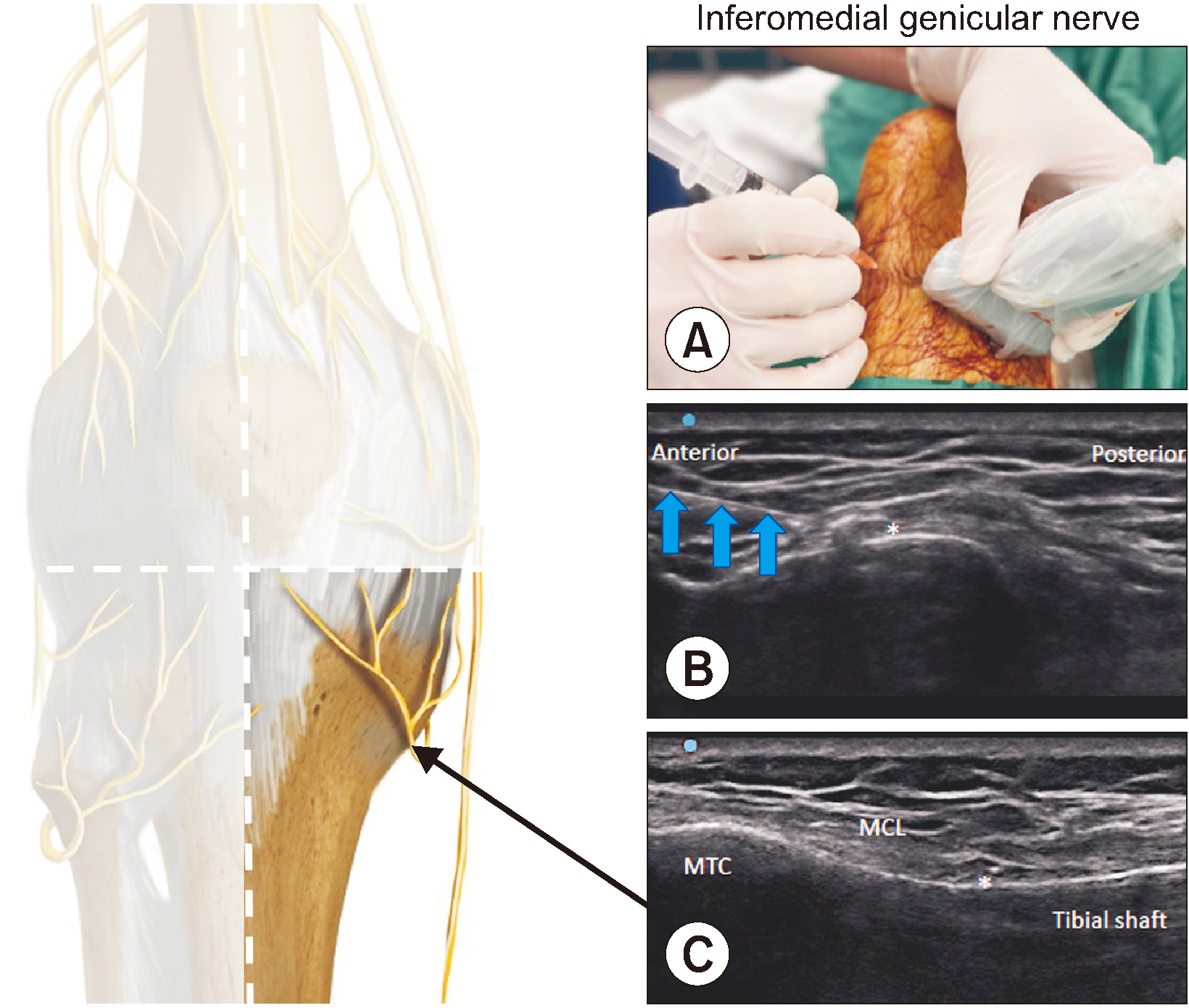
Fig. 6 Inferomedial genicular nerve. Fig. 6A indicates the probe position. Fig. 6B is transverse view of ultrasound image with needle tip around 50% of the anterior cortex of tibial shaft. Fig. 6C is coronal view, showing needle tip underneath the medial collateral ligament (MCL). Inferomedial genicular nerve. Note the dual-plane confirmation of the final needle position. MTC: medial tibial condyle, Asterisk: final needle position, Blue arrows: needle.
Cited by 1 articles
-
Genicular nerve radiofrequency ablation: proposal of a technical protocol for managing procedural pain
Andrés Rocha-Romero, Tony Kwun Tung Ng, Guilherme Ferreira-Dos-Santos
Korean J Pain. 2025;38(1):81-84. doi: 10.1136/rapm-2023-105127.
Reference
-
1. Yildiz G, Perdecioglu GRG, Yuruk D, Can E, Akkaya OT. 2023; Comparison of the efficacy of genicular nerve phenol neurolysis and radiofrequency ablation for pain management in patients with knee osteoarthritis. Korean J Pain. 36:450–7. DOI: 10.3344/kjp.23200. PMID: 37732409. PMCID: PMC10551393.
Article2. McCormick ZL, Cohen SP, Walega DR, Kohan L. 2021; Technical considerations for genicular nerve radiofrequency ablation: optimizing outcomes. Reg Anesth Pain Med. 46:518–23. DOI: 10.1136/rapm-2020-102117. PMID: 33483425.
Article3. Fonkoue L, Stoenoiu MS, Behets CW, Steyaert A, Kouassi JK, Detrembleur C, et al. 2021; Validation of a new protocol for ultrasound-guided genicular nerve radiofrequency ablation with accurate anatomical targets: cadaveric study. Reg Anesth Pain Med. 46:210–6. DOI: 10.1136/rapm-2020-101936. PMID: 33273065.
Article4. Ng TK, Lam KHS, Allam AE. 2022; Motor-sparing neural ablation with modified techniques for knee pain: case series on knee osteoarthritis and updated review of the underlying anatomy and available techniques. Biomed Res Int. 2022:2685898. DOI: 10.1155/2022/2685898. PMID: 35686229. PMCID: PMC9173899.
Article5. Guven Kose S, Kirac Unal Z, Kose HC, Celikel F, Akkaya OT. 2023; Ultrasound-guided genicular nerve radiofrequency treatment: prospective randomized comparative trial of a 3-nerve protocol versus a 5-nerve protocol. Pain Med. 24:758–67. DOI: 10.1093/pm/pnad025. PMID: 36869680.
Article6. Forero M, Olejnik LJ, Stager SC. 2023; Six-target radiofrequency ablation of the genicular nerve for the treatment of chronic knee pain. Reg Anesth Pain Med. doi: 10.1136/rapm-2023-104643. DOI: 10.1136/rapm-2023-104643. PMID: 37316307.
Article7. Krijgh DD, List EB, Teunis T, Bleys RLAW, Coert JH. 2022; The origin and course of the infrapatellar branch of the saphenous nerve: an anatomical study. JPRAS Open. 34:144–51. DOI: 10.1016/j.jpra.2022.08.006. PMID: 36304072. PMCID: PMC9593300.
Article8. Tran J, Peng PWH, Lam K, Baig E, Agur AMR, Gofeld M. 2018; Anatomical study of the innervation of anterior knee joint capsule: implication for image-guided intervention. Reg Anesth Pain Med. 43:407–14. DOI: 10.1097/AAP.0000000000000778. PMID: 29557887.9. Rocha-Romero A, Juárez-Lemus ÁM, Hernández-Porras BC. 2021; A safer step-by-step approach for erector spinae plane phenol neurolytic blocks. Can J Anaesth. 68:585–6. DOI: 10.1007/s12630-020-01901-3. PMID: 33420676. PMCID: PMC7793616.10. Risso RC, Ferraro LHC, Nouer Frederico T, Peng PWH, Luzo MV, Debieux P, et al. 2021; Chemical ablation of genicular nerve with phenol for pain relief in patients with knee osteoarthritis: a prospective study. Pain Pract. 21:438–44. DOI: 10.1111/papr.12972. PMID: 33277760.
Article11. Tran J, Peng P, Agur A. 2020; Evaluation of nerve capture using classical landmarks for genicular nerve radiofrequency ablation: 3D cadaveric study. Reg Anesth Pain Med. 45:898–906. DOI: 10.1136/rapm-2020-101894. PMID: 32928998.12. Rocha-Romero A. 2023; Diagnosis and treatment of post-radiofrequency synovial knee fistula: case report. A A Pract. 17:e01731. DOI: 10.1213/XAA.0000000000001731. PMID: 37991193.
Article13. Cosman ER Jr, Dolensky JR, Hoffman RA. 2014; Factors that affect radiofrequency heat lesion size. Pain Med. 15:2020–36. DOI: 10.1111/pme.12566. PMID: 25312825.
Article14. Bordoni B, Varacallo MA, Morabito B, Simonelli M. 2019; Biotensegrity or fascintegrity? Cureus. 11:e4819. DOI: 10.7759/cureus.4819.
Article15. Bordoni B, Myers T. 2020; A review of the theoretical fascial models: biotensegrity, fascintegrity, and myofascial chains. Cureus. 12:e7092. DOI: 10.7759/cureus.7092.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of the efficacy of genicular nerve phenol neurolysis and radiofrequency ablation for pain management in patients with knee osteoarthritis
- Investigation of the existence of and a block technique for the inferior lateral genicular nerve: cadaveric study
- Predictive factors associated with successful response to utrasound guided genicular radiofrequency ablation
- Comparison of ultrasound guided pulsed radiofrequency of genicular nerve with local anesthetic and steroid block for management of osteoarthritis knee pain
- Retraction: Comparison of the efficacy of genicular nerve phenol neurolysis and radiofrequency ablation for pain management in patients with knee osteoarthritis
