Conservative enucleation for physiologic space closure in adenomatoid odontogenic tumor
- Affiliations
-
- 1Departments of Oral and Maxillofacial Surgery, Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
- 2Departments of Oral Pathology, Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
- KMID: 2557635
- DOI: http://doi.org/10.5125/jkaoms.2024.50.3.170
Abstract
- Adenomatoid odontogenic tumor (AOT) is a rare, asymptomatic, slow-growing benign tumor that can be divided into three variants: follicular, extrafollicular, and peripheral. By treating AOT using an enucleation and curettage approach, recurrence can be avoided. We report a case of a 24-year-old female who presented with a lump in the right mandibular premolar area along with diastema between displaced teeth #43 and #44 and was diagnosed with extrafollicular AOT. The patient was managed with enucleation-curettage surgery without additional bone graft procedure along with routine follow-up. A successful outcome without recurrence was achieved, and diastema closure with repositioning of the displaced teeth did not require orthodontic treatment. AOT should be managed via enucleation and curettage to obtain successful outcomes without recurrence. Spontaneous bone regeneration following enucleation can be achieved without guided bone regeneration. Also, diastema closure and repositioning of displaced teeth can occur without orthodontic interventions through physiologic drift.
Keyword
Figure
-
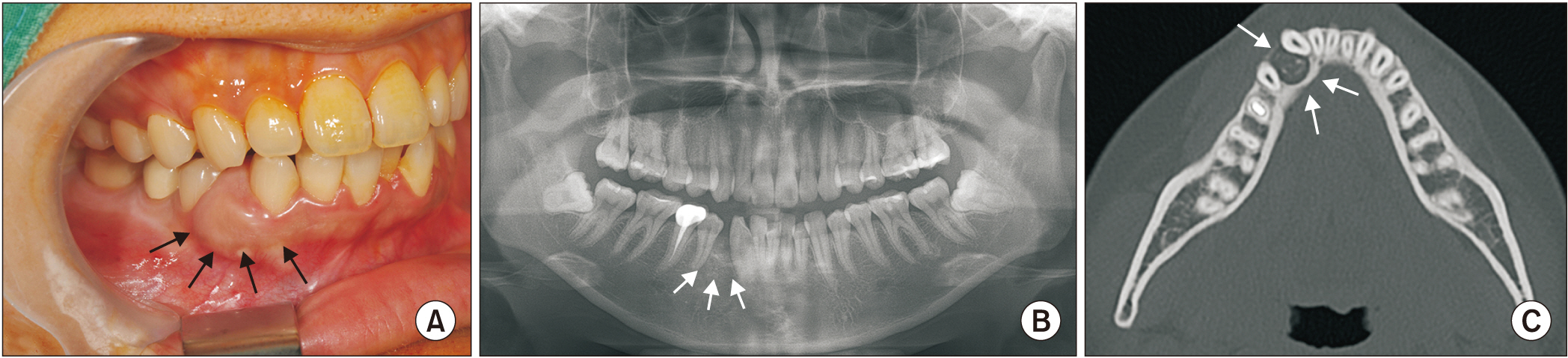
Fig. 1 A. Intraoral view demonstrated a round mass with diastema between displaced teeth #43 and #44 (arrows). B. Panoramic radiograph showed a semi-circular radiolucency with a coarse corticated margin in the upper part of the alveolar bone between teeth #43 and #44 roots (arrows). C. Axial computed tomography view showed a round, soft tissue attenuated lesion with a rough and thick corticated margin in the alveolar bone between the roots of teeth #43 and #44 (arrows).
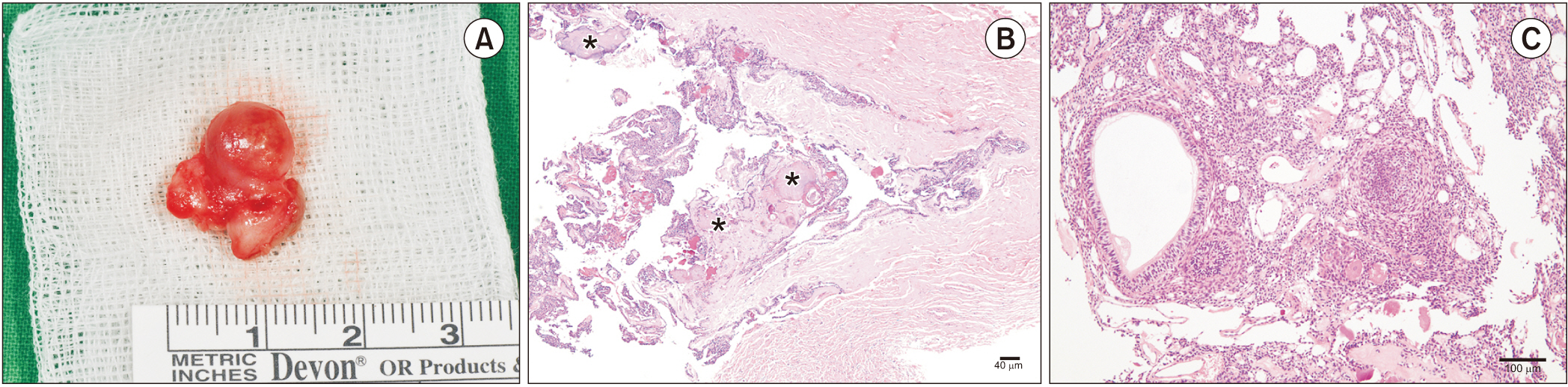
Fig. 2 A. The retrieved 1.5-cm-diameter circumscribed round mass. Representative histopathological features of adenomatoid odontogenic tumor. B. The tumor is surrounded by a thick fibrous capsule and contains small amounts of calcification (asterisks). H&E staining; scale bar=40 μm. C. Sheets of spindle-shaped tumor cells showing whorled areas or duct-like and tubular structures. H&E staining; scale bar=100 μm.
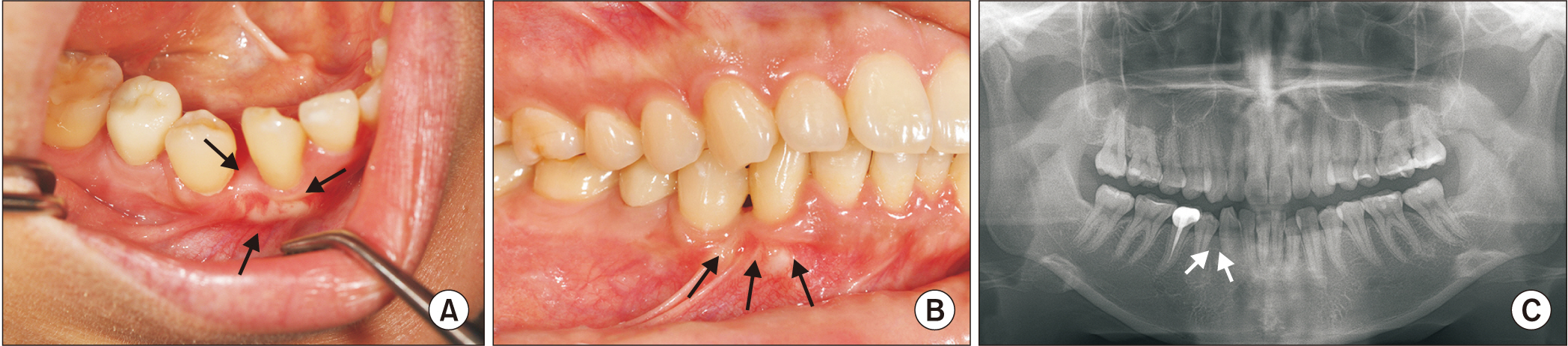
Fig. 3 A. Two months following surgery, the soft tissue was in the healing process and the space between teeth #43 and #44 was reduced (arrows). B. Lateral intraoral view showed tooth #43 repositioning and diastema closure without orthodontic interference (arrows). C. Panoramic view nine months following surgery revealed full bone healing with no recurrence of the adenomatoid odontogenic tumor and proximal contact of teeth #43 and #44 (arrows).
Reference
-
References
1. Al-Shimari F, Chandra S, Oda D. 2017; Adenomatoid odontogenic tumor: case series of 14 with wide range of clinical presentation. J Clin Exp Dent. 9:e1315–21. https://doi.org/10.4317/jced.54216. DOI: 10.4317/jced.54216. PMID: 29302284. PMCID: PMC5741845.
Article2. Philipsen HP, Reichart PA, Zhang KH, Nikai H, Yu QX. 1991; Adenomatoid odontogenic tumor: biologic profile based on 499 cases. J Oral Pathol Med. 20:149–58. https://doi.org/10.1111/j.1600-0714.1991.tb00912.x. DOI: 10.1111/j.1600-0714.1991.tb00912.x. PMID: 2061853.
Article3. Thakur A, Tupkari JV, Joy T, Hanchate AV. 2016; Adenomatoid odontogenic tumor: what is the true nature? Med Hypotheses. 97:90–3. https://doi.org/10.1016/j.mehy.2016.10.024. DOI: 10.1016/j.mehy.2016.10.024. PMID: 27876138.
Article4. Philipsen HP, Srisuwan T, Reichart PA. 2002; Adenomatoid odontogenic tumor mimicking a periapical (radicular) cyst: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 94:246–8. https://doi.org/10.1067/moe.2002.124767. DOI: 10.1067/moe.2002.124767. PMID: 12221394.
Article5. Lang MJ, Wang YP, Lin HP, Chen HM, Kuo YS. 2015; Adenomatoid odontogenic tumor-report of a posterior mandibular case with the presence of ghost cells. J Dent Sci. 10:216–22. https://doi.org/10.1016/j.jds.2012.03.027. DOI: 10.1016/j.jds.2012.03.027.
Article6. Ide F, Kikuchi K, Kusama K. 2017; Adenomatoid odontogenic tumor revisited. Med Hypotheses. 104:35. https://doi.org/10.1016/j.mehy.2017.05.016. DOI: 10.1016/j.mehy.2017.05.016. PMID: 28673585.
Article7. Chrcanovic BR, Gomez RS. 2019; Adenomatoid odontogenic tumor: an updated analysis of the cases reported in the literature. J Oral Pathol Med. 48:10–6. https://doi.org/10.1111/jop.12783. DOI: 10.1111/jop.12783. PMID: 30256456.
Article8. Chuan-Xiang Z, Yan G. 2007; Adenomatoid odontogenic tumor: a report of a rare case with recurrence. J Oral Pathol Med. 36:440–3. https://doi.org/10.1111/j.1600-0714.2007.00521.x. DOI: 10.1111/j.1600-0714.2007.00521.x. PMID: 17617839.
Article9. Raubenheimer EJ, Seeliger JE, van Heerden WF, Dreyer AF. 1991; Adenomatoid odontogenic tumour: a report of two large lesions. Dentomaxillofac Radiol. 20:43–5. https://doi.org/10.1259/dmfr.20.1.1884853. DOI: 10.1259/dmfr.20.1.1884853. PMID: 1884853.
Article10. Vitkus R, Meltzer JA. 1996; Repair of a defect following the removal of a maxillary adenomatoid odontogenic tumor using guided tissue regeneration. A case report. J Periodontol. 67:46–50. https://doi.org/10.1902/jop.1996.67.1.46. DOI: 10.1902/jop.1996.67.1.46. PMID: 8676273.
Article11. Chiapasco M, Rossi A, Motta JJ, Crescentini M. 2000; Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases. J Oral Maxillofac Surg. 58:942–8. discussion 949. https://doi.org/10.1053/joms.2000.8732. DOI: 10.1053/joms.2000.8732. PMID: 10981973.
Article12. Ettl T, Gosau M, Sader R, Reichert TE. 2012; Jaw cysts - filling or no filling after enucleation? A review. J Craniomaxillofac Surg. 40:485–93. https://doi.org/10.1016/j.jcms.2011.07.023. DOI: 10.1016/j.jcms.2011.07.023. PMID: 21890372.
Article13. Ide F, Mishima K, Kikuchi K, Horie N, Yamachika S, Satomura K, et al. 2011; Development and growth of adenomatoid odontogenic tumor related to formation and eruption of teeth. Head Neck Pathol. 5:123–32. https://doi.org/10.1007/s12105-011-0253-3. DOI: 10.1007/s12105-011-0253-3. PMID: 21380723. PMCID: PMC3098332.
Article14. Seo WG, Kim CH, Park HS, Jang JW, Chung WY. 2015; Adenomatoid odontogenic tumor associated with an unerupted mandibular lateral incisor: a case report. J Korean Assoc Oral Maxillofac Surg. 41:342–5. https://doi.org/10.5125/jkaoms.2015.41.6.342. DOI: 10.5125/jkaoms.2015.41.6.342. PMID: 26734563. PMCID: PMC4699937.
Article15. Terkawi MA, Matsumae G, Shimizu T, Takahashi D, Kadoya K, Iwasaki N. 2022; Interplay between inflammation and pathological bone resorption: insights into recent mechanisms and pathways in related diseases for future perspectives. Int J Mol Sci. 23:1786. https://doi.org/10.3390/ijms23031786. DOI: 10.3390/ijms23031786. PMID: 35163708. PMCID: PMC8836472.
Article16. Jonasson G, Skoglund I, Rythén M. 2018; The rise and fall of the alveolar process: dependency of teeth and metabolic aspects. Arch Oral Biol. 96:195–200. https://doi.org/10.1016/j.archoralbio.2018.09.016. DOI: 10.1016/j.archoralbio.2018.09.016. PMID: 30292055.
Article17. Teng F, Du FY, Chen HZ, Jiang RP, Xu TM. 2019; Three-dimensional analysis of the physiologic drift of adjacent teeth following maxillary first premolar extractions. Sci Rep. 9:14549. https://doi.org/10.1038/s41598-019-51057-4. DOI: 10.1038/s41598-019-51057-4. PMID: 31601925. PMCID: PMC6787091.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extensive Adenomatoid Odontogenic Tumor of the Maxilla: A Case Report of Conservative Surgical Excision and Orthodontic Alignment of Impacted Canine
- Recurrent Adenomatoid Odontogenic Tumor Arising From A Dentigerous Cyst
- A Case of Adenomatoid Odontogenic Tumor
- Adenomatoid odontogenic tumor associated with an unerupted mandibular lateral incisor: a case report
- Adenomatoid Odontogenic Tumor in the Posterior Mandible of a Young Child : A Case Report
