Cardiomyopathy Without Amyloid Deposit in Systemic Light Chain Deposition Disease
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea
- 2Department of Internal Medicine, School of Medicine, Kyungpook National University, Daegu, Korea
- 3Division of Cardiology, Department of Internal Medicine, Kyungpook National University Chilgok Hospital, Daegu, Korea
- KMID: 2555535
- DOI: http://doi.org/10.4070/kcj.2024.0022
Figure
-
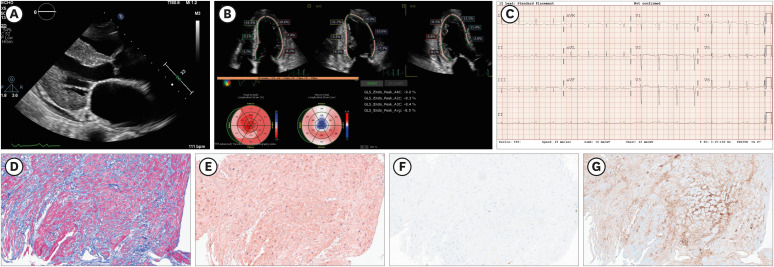
Figure 1 Images and histological analyses in a case with cardiac light chain deposition disease. (A) Transthoracic echocardiographic image showing left ventricular wall thickness with disproportionate interventricular septal enlargement, resulting in a ‘speckled’ appearance and small pericardial effusion (parasternal long-axis view). (B) Regional longitudinal strain, assessed by 2-dimensional speckle-tracking echocardiography. The reduction in global longitudinal strain is particularly observed in the basal and mid-ventricular segments, manifesting as an ‘apical sparing’ pattern. The mean global longitudinal strain was −8.5%. (C) Electrocardiogram; The electrocardiogram of the patient reveals characteristic findings, including low voltage in the limb leads (QRS amplitude <5 mm in leads II, III, aVR, aVF) and a pseudo-infarct pattern (pathologic Q waves in V1, V2, V3, accompanied by the loss of R wave progression). (D, G) Histological analyses of endomyocardial biopsy specimens. (D) Trichrome staining: The blue areas signify significant interstitial fibrosis, original magnification ×100. (E) Congo red staining; The Congo red stain did not show extracellular deposition of amyloid fibrils in the myocardial interstitium, original magnification ×100. (F) Immunofluorescence using anti-κ light chain antibody; the myocardial interstitium shows a negative reaction, original magnification ×100. (G) Immunofluorescence using anti-λ light chain antibody; The immunostaining with anti-λ light chain antibodies reveals intense positivity in the myocardial interstitium, original magnification ×100.aVR = augmented vector right; aVF = augmented vector foot.
Reference
-
1. Falk RH, Alexander KM, Liao R, Dorbala S. AL (light-chain) cardiac amyloidosis: a review of diagnosis and therapy. J Am Coll Cardiol. 2016; 68:1323–1341. PMID: 27634125.2. Cheng Z, Zhu K, Tian Z, Zhao D, Cui Q, Fang Q. The findings of electrocardiography in patients with cardiac amyloidosis. Ann Noninvasive Electrocardiol. 2013; 18:157–162. PMID: 23530486.3. Nakamura M, Satoh M, Kowada S, et al. Reversible restrictive cardiomyopathy due to light-chain deposition disease. Mayo Clin Proc. 2002; 77:193–196. PMID: 11838655.4. Nishioka R, Yoshida S, Takamatsu H, Kawano M. Cardiac light-chain deposition disease and hints at diagnosing: a case report. Eur Heart J Case Rep. 2023; 7:ytad049. PMID: 36860729.5. Mohan M, Buros A, Mathur P, et al. Clinical characteristics and prognostic factors in multiple myeloma patients with light chain deposition disease. Am J Hematol. 2017; 92:739–745. PMID: 28383130.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pericardial Amyloidosis Associated with Light-chain Myeloma
- A Case of Primary Nodular Cutaneous Amyloidosis
- A Case of Amyloid Goiter Masquerading as Graves' Disease
- A Case of Macroglossia due to Amyloidosis Associated with Multiple Myeloma
- A Case of Localized Amyloid Light-Chain Amyloidosis in the Small Intestine
