Anesth Pain Med.
2024 Apr;19(2):109-116. 10.17085/apm.23097.
Opioid-free anesthesia using a combination of ketamine and dexmedetomidine in patients undergoing laparoscopic cholecystectomy: a randomized controlled trial
- Affiliations
-
- 1Department of Anaesthesiology, All India Institute of Medical Sciences Patna, Patna, India
- KMID: 2555247
- DOI: http://doi.org/10.17085/apm.23097
Abstract
- Background
Opioids administered as bolus doses or continuous infusions are widely used by anesthesiologists worldwide for major and day care surgeries. Opioid-free anesthesia is a multimodal anesthesia and analgesia technique that does not use opioid drugs, thereby benefitting patients from opioid-related adverse effects. In this study, we compared the postoperative analgesic requirements of patients scheduled for elective laparoscopic cholecystectomy under opioid-free and opioid-based anesthesia.
Methods
This study included 88 patients aged 18–60 years with American Society of Anesthesiologists physical status 1 and 2 who underwent elective laparoscopic cholecystectomy. Participants were randomly divided into two groups with forty-four participants in each group. The opioid-free anesthesia group was administered an intravenous bolus of ketamine and dexmedetomidine, whereas the opioid-based group was administered fentanyl with conventional general anesthesia. The primary outcome was to compare the total amount of fentanyl consumed by both groups during the 6 h postoperative period following extubation. Episodes of postoperative nausea and vomiting (PONV) and vital signs were noted throughout the postoperative period to analyze the secondary outcomes.
Results
Both the groups had similar demographic characteristics. The opioid-free group required less postoperative analgesia within the first 2 h (61.4 ± 17.4 vs. 79.0 ± 19.4 of fentanyl, P < 0.001), which was statistically significant. However, fentanyl consumption was comparable between the groups at the sixth postoperative hour (opioid-free group 152 ± 28.2 vs. opioid group 164 ± 33.4, P = 0.061). Compared with 4.5% of the participants in the opioid-free group, 34% of those in the opioid-based group developed moderate PONV.
Conclusions
The opioid-free anesthesia technique in patients undergoing laparoscopic cholecystectomy reduced the requirement of analgesia in the first two hours of the postoperative period and was associated with decreased PONV.
Keyword
Figure
-
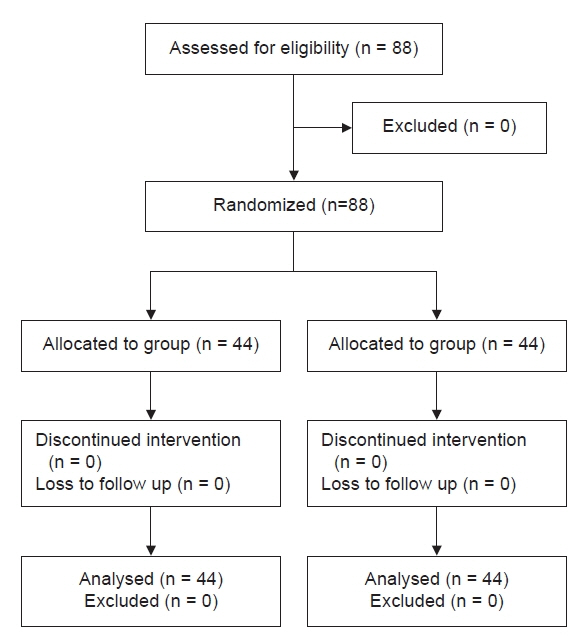
Fig. 1. Flow diagram of the study participants.
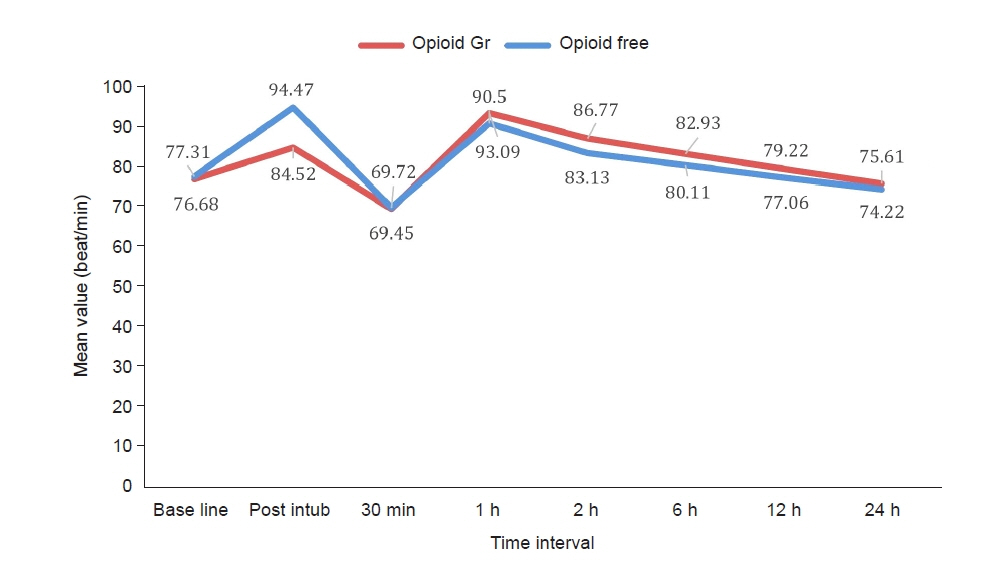
Fig. 2. Comparison of the mean heart rate between the two groups during the intraoperative and 24 postoperative periods.
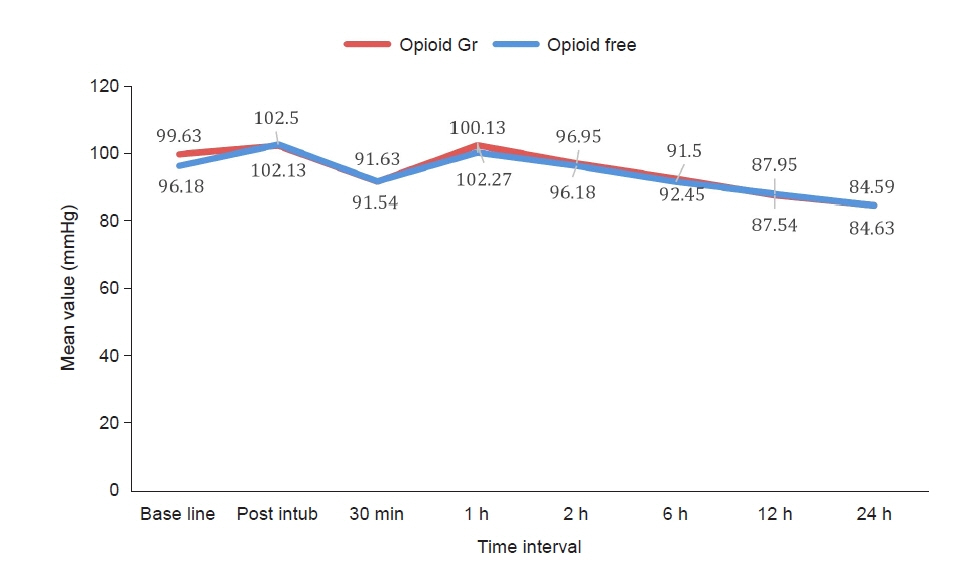
Fig. 3. Comparison of mean arterial pressure between the two groups during the intraoperative and 24 postoperative periods.
Cited by 1 articles
-
A message from the Editor-in-Chief and Editorial Board, 2024: journal metrics and statistics, and appreciation to reviewers
Jun Hyun Kim, Hyun Kang
Anesth Pain Med. 2025;20(1):1-4. doi: 10.17085/apm.25202.
Reference
-
1. Nagappa M, Weingarten TN, Montandon G, Sprung J, Chung F. Opioids, respiratory depression, and sleep disordered breathing. Best Pract Res Clin Anaesthesiol. 2017; 31:469–85.2. Fletcher D, Martinez V. Opioid-induced hyperalgesia in patients after surgery: a systematic review and meta-analysis. Br J Anaesth. 2014; 112:991–1004.
Article3. Roberts GW, Bekker TB, Carlsen HH, Moffatt CH, Slattery PJ, McClure AF. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth Analg. 2005; 101:1343–8.
Article4. Dinges HC, Otto S, Stay DK, Bäumlein S, Waldmann S, Kranke P, et al. Side-effect rates of opioids in equianalgesic doses via intravenous patient-controlled analgesia: a systematic review and network meta-analysis. Anesth Analg. 2019; 129:1153–62.5. Kuehn BM. Scientists, officials eye tools aimed at combating abuse of painkillers. JAMA. 2012; 307:19–21.
Article6. Casati A, Sedefov R, Pfeiffer-Gerschel T. Misuse of medicines in the European Union: A systematic review of the literature. Eur Addict Res. 2012; 18:228–45.
Article7. Tan M, Law LSC, Gan TJ. Optimizing pain management to facilitate enhanced recovery after surgery pathways. Can J Anesth. 2015; 62:203–18.
Article8. Gurbet A, Basagan-Mogol E, Turker G, Ugun F, Kaya FN, Ozcan B. Intraoperative infusion of dexmedetomidine reduces perioperative analgesic requirements. Can J Anesth. 2006; 53:646–52.
Article9. Loftus RW, Yeager MP, Clark JA, Brown JR, Abdu WA, Sengupta DK, et al. Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology. 2010; 113:639–46.
Article10. Waldron NH, Jones CA, Gan TJ, Allen TK, Habib AS. Impact of perioperative dexamethasone on postoperative analgesia and side effects: a systematic review and meta-analysis. Br J Anaesth. 2013; 110:191–200.
Article11. Weibel S, Jokinen J, Pace NL, Schnabel A, Hollmann MW, Hahnenkamp K. Efficacy and safety of intravenous lidocaine for postoperative analgesia and recovery after surgery: Aa systematic review with trial sequential analysis. Br J Anaesth. 2016; 116:770–83.12. Ong CK, Seymour RA, Lirk P, Merry AF. Combining paracetamol (acetaminophen) with nonsteroidal anti-inflammatory drugs: a qualitative systematic review of analgesic efficacy for acute postoperative pain. Anesth Analg. 2010; 110:1170–9.13. Collard V, Mistraletti G, Taqi A, Asenjo JF, Feldman LS, Fried GM, et al. Intraoperative esmolol infusion in the absence of opioids spares postoperative fentanyl in patients undergoing ambulatory laparoscopic cholecystectomy. Anesth Analg. 2007; 105:1255–62.
Article14. Blaudszun G, Lysakowski C, Elia N, Tramer MR. Effect of perioperative systemic alpha2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysis of randomized controlled trials. Anesthesiology. 2012; 116:1312–22.15. Brinck EC, Tiippana E, Heesen M, Bell RF, Straube S, Moore RA, et al. Perioperative intravenous ketamine for acute postoperative pain in adults. Cochrane Database Syst Rev. 2018; 12:CD012033.
Article16. McCartney CJ, Sinha A, Katz J. A qualitative systematic review of the role of N-methyl-D-aspartate receptor antagonists in preventive analgesia. Anesth Analg. 2004; 98:1385–400.
Article17. Bakan M, Umutoglua T, Topuza U, Uysala H, Bayram M, Kadioglu H, et al. [Opioid free total intravenous anesthesia with propofol, dexmedetomidine and lidocaine infusions for laparoscopic cholecystectomy: a prospective, randomized, double blinded study]. Rev Bras Anestesiol. 2015; 65:191–9. Portuguese.18. Bhardwaj S, Garg K, Devgan S. Comparison of opioid-based and opioid-free TIVA for laparoscopic urological procedures in obese patients. J Anaesthesiol Clin Pharmacol. 2019; 35:481–6.
Article19. Ziemann Gimmel P, Goldfarb AA, Koppman J, Marema RT. Opioid-free total intravenous anaesthesia reduces postoperative nausea and vomiting in bariatric surgery beyond triple prophylaxis. Br J Anaesth. 2014; 112:906–11.
Article20. Beloeil H, Garot M, Lebuffe G, Gerbaud A, Bila J, Cuvillon P, et al; POFA Study Group; SFAR Research Network. Balanced opioid-free anesthesia with dexmedetomidine versus balanced anesthesia with remifentanil for major or intermediate noncardiac surgery. Anesthesiology. 2021; 134:541–51.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preoperative dexmedetomidine and intraoperative bradycardia in laparoscopic cholecystectomy: a meta-analysis with trial sequential analysis
- Laparoscopic appendectomy under spinal anesthesia with dexmedetomidine infusion
- Comparison of effects of intraoperative esmolol and ketamine infusion on acute postoperative pain after remifentanil-based anesthesia in patients undergoing laparoscopic cholecystectomy
- A Double-blinded, Randomized, Placebo Controlled Study of the Effect a Small Dose of Ketamine has on Postoperative Pain of Sevoflurane-remifentanil Anesthesia
- Comparison of effects of intraoperative nefopam and ketamine infusion on managing postoperative pain after laparoscopic cholecystectomy administered remifentanil
