Choroid Plexus Hyperplasia : Report of Two Cases with Unique Radiologic Findings
- Affiliations
-
- 1Division of Pediatric Neurosurgery, Seoul National University Children’s Hospital, Seoul National University College of Medicine, Seoul, Korea
- 2Jikei University School of Medicine, Tokyo, Japan
- KMID: 2554875
- DOI: http://doi.org/10.3340/jkns.2023.0126
Abstract
- Choroid plexus hyperplasia (CPH), also known as diffuse villous hyperplasia of choroid plexus, is a rare condition characterized by excessive production of cerebrospinal fluid (CSF), resulting in hydrocephalus. Diagnosing CPH can be challenging due to the absence of clear imaging criteria for choroid plexus hypertrophy and the inability to assess CSF production non-invasively. As a result, many CPH patients are initially treated with a ventriculoperitoneal (VP) shunt, but subsequently require additional surgical intervention due to intractable ascites. In our study, we encountered two CPH patients who presented with significantly enlarged subarachnoid spaces, reduced parenchymal volume, and prominent choroid plexus. Initially, we treated these patients with a VP shunt, but eventually opted for endoscopic choroid plexus cauterization (CPC) to address the intractable ascites. Following the treatment with endoscopic CPC, we observed a gradual reduction in subarachnoid spaces and an increase in parenchymal volume. In cases where bilateral prominent choroid plexus, markedly enlarged subarachnoid spaces, and cortical atrophy are present, CPH should be suspected. In these cases, considering initial treatment with combined endoscopic CPC and shunt may help minimize the need for multiple surgical interventions.
Figure
-
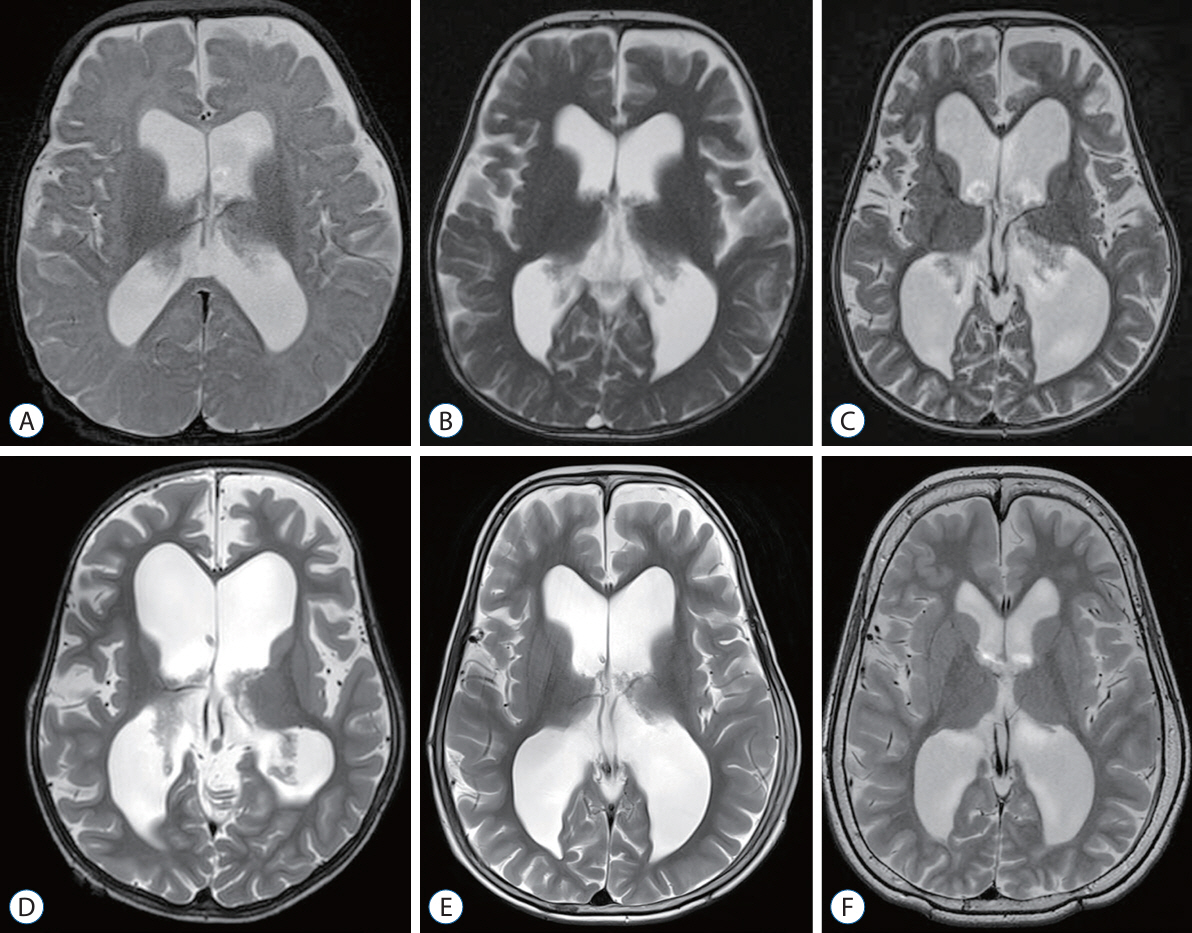
Fig. 1. Radiologic findings of patient 1. A 5-month-old girl presented with a large head circumference. A : The initial magnetic resonance imaging (MRI) shows a slight enlarged subarachnoid space. B : At 14-month of age, a prominent choroid plexus is observed. C : At 31-month of age, ventriculoperitoneal (VP) shunt was performed due to significant progression of ventriculomegaly, enlargement of the subarachnoid space, and decreased parenchymal volume. D : After the VP shunt, the patient experienced intractable ascites, and at 44-month of age, progressive ventriculomegaly is evident, leading to endoscopic choroid plexus cauterization. E and F : The MRI scans at 63-month of age and 10-year follow-ups show recovery of the parenchymal volume and resolution of ventriculomegaly.
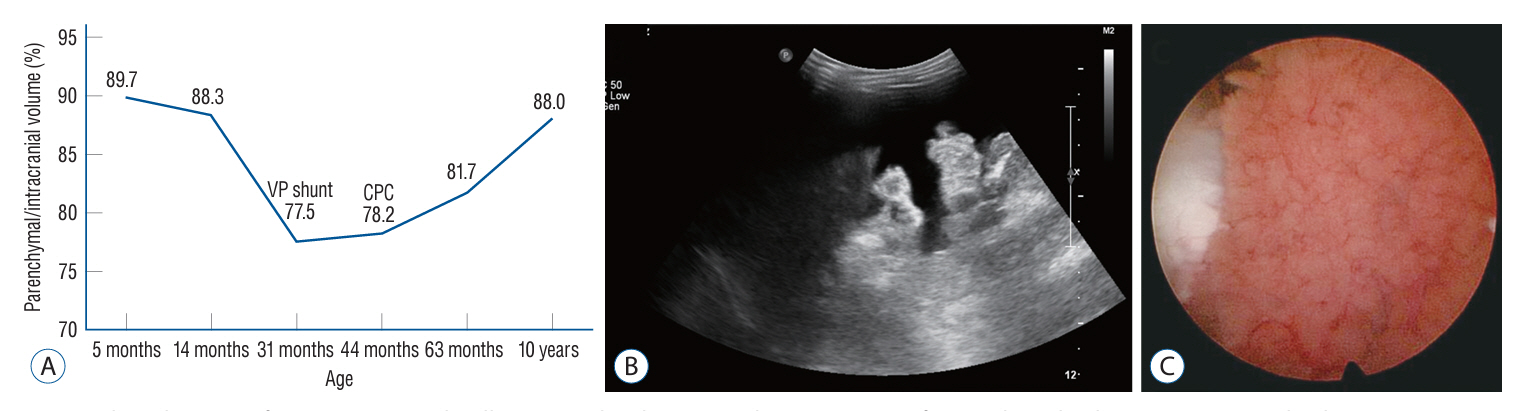
Fig. 2. Clinical course of patient 1. A : A plot illustrating the changes in the percentage of parenchymal volume to intracranial volume over time in patient 1. B : Abdomen ultrasonography shows intractable ascites occurred following the ventriculo-peritoneal shunt. C : Intraoperative photo during the endoscopic choroid plexus cauterization displaying the hyperplastic choroid plexus during endoscopic choroid plexus cauterization. VP : ventriculo-periotneal, CPC : choroid plexus cauterization.
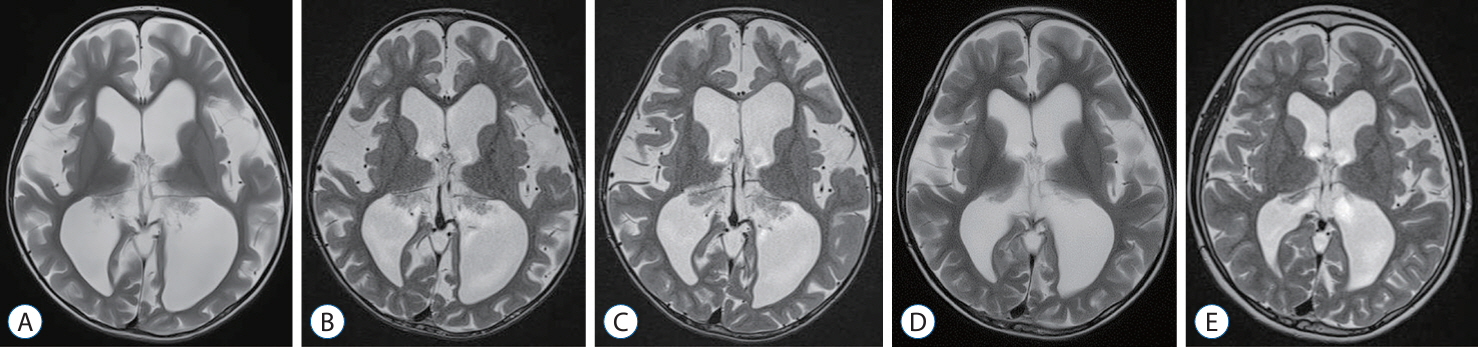
Fig. 3. Radiologic findings of patient 2. A 31-month-old girl presented with a large head circumference and gross motor developmental delay. A : Her initial magnetic resonance imaging (MRI) reveals a prominent choroid plexus with marked enlargement of the subarachnoid space and cortical atrophy. B : At 38-month of age, no changes in the enlarged subarachnoid space and decreased parenchymal volume are observed. C : At 44-month of age, enlarged subarachnoid space and decreased parenchymal volume is still present and the endoscopic choroid plexus cauterization was performed. D : At 51-month of age, the MRI shows a slight increase in parenchymal volume. E : At the latest follow-up at 8 years old, the patient fully recovered from the developmental delay, and the MRI reveals a marked increase in parenchymal volume.
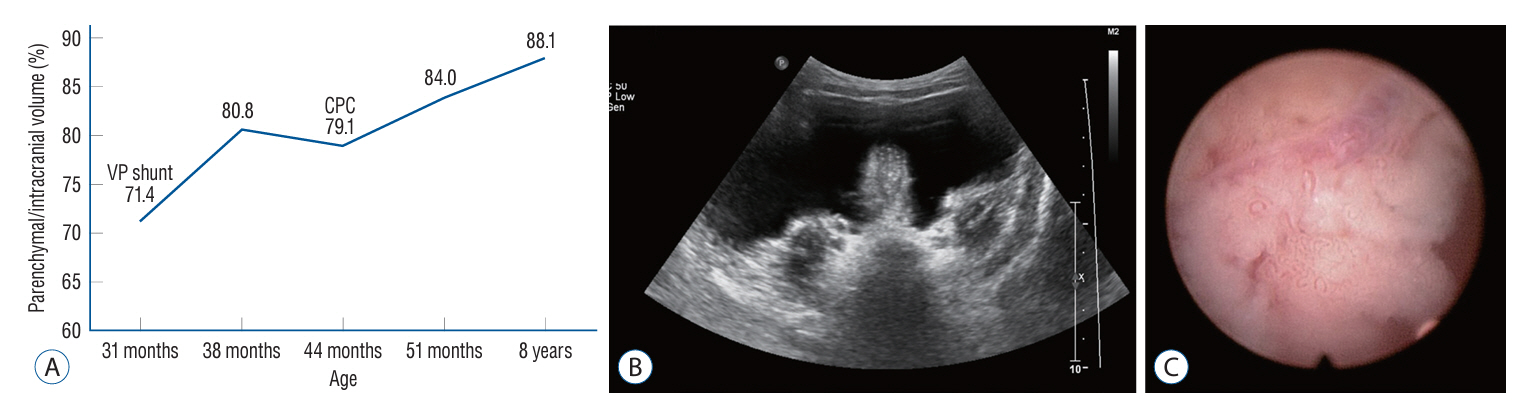
Fig. 4. Clinical course of patient 2. A : A plot illustrating the changes in the percentage of parenchymal volume to intracranial volume over time in patient 2. B : Abdomen ultrasonography demonstrates intractable ascites occurred following the ventriculo-peritoneal shunt. C : Intraoperative photo the endoscopic choroid plexus cauterization showing the hyperplastic choroid plexus with choroidal vessel. VP : ventriculo-periotneal, CPC : choroid plexus cauterization.
Reference
-
References
1. Anei R, Hayashi Y, Hiroshima S, Mitsui N, Orimoto R, Uemori G, et al. Hydrocephalus due to diffuse villous hyperplasia of the choroid plexus. Neurol Med Chir (Tokyo). 51:437–441. 2011.2. Aziz AA, Coleman L, Morokoff A, Maixner W. Diffuse choroid plexus hyperplasia: an under-diagnosed cause of hydrocephalus in children? Pediatr Radiol. 35:815–818. 2005.
Article3. Bering EA Jr, Sato O. Hydrocephalus: changes in formation and absorption of cerebrospinal fluid within the cerebral ventricles. J Neurosurg. 20:1050–1063. 1963.
Article4. Bernstock JD, Tafel I, Segar DJ, Dowd R, Kappel A, Chen JA, et al. Complex management of hydrocephalus secondary to choroid plexus hyperplasia. World Neurosurg. 141:101–109. 2020.
Article5. Boxill M, Becher N, Sunde L, Thelle T. Choroid plexus hyperplasia and chromosome 9p gains. Am J Med Genet A. 176:1416–1422. 2018.
Article6. Cataltepe O, Liptzin D, Jolley L, Smith TW. Diffuse villous hyperplasia of the choroid plexus and its surgical management. J Neurosurg Pediatr. 5:518–522. 2010.7. Davis LE. A physio-pathologic study of the choroid plexus with the report of a case of villous hypertrophy. J Med Res. 44:521–534.11. 1924.8. Hallaert GG, Vanhauwaert DJ, Logghe K, Van den Broecke C, Baert E, Van Roost D, et al. Endoscopic coagulation of choroid plexus hyperplasia. J Neurosurg Pediatr. 9:169–177. 2012.9. Hussain ZB, Hussain AB, Mitchell P. Extra-axial cerebrospinal fluid spaces in children with benign external hydrocephalus: a case-control study. Neuroradiol J. 30:410–417. 2017.10. Iplikcioglu AC, Bek S, Gökduman CA, Bikmaz K, Cosar M. Diffuse villous hyperplasia of choroid plexus. Acta Neurochir (Wien). 148:691–694. discussion 694. 2006.
Article11. Li D, Shokuhfar T, Pantalone J, Rothstein B, Alden TD, Shaibani A, et al. Choroidal artery embolization in the management of cerebrospinal fluid overproduction: case report and review of the literature. J Neurosurg Pediatr. 23:737–748. 2019.
Article12. Paez-Nova M, Andaur K, Campos G, Garcia-Ballestas E, Moscote-Salazar LR, Koller O, et al. Bilateral hyperplasia of choroid plexus with severe CSF production: a case report and review of the glymphatic system. Childs Nerv Syst. 37:3521–3529. 2021.
Article13. Philips MF, Shanno G, Duhaime AC. Treatment of villous hypertrophy of the choroid plexus by endoscopic contact coagulation. Pediatr Neurosurg. 28:252–256. 1998.
Article14. Tamburrini G, Caldarelli M, Di Rocco F, Massimi L, D’Angelo L, Fasano T, et al. The role of endoscopic choroid plexus coagulation in the surgical management of bilateral choroid plexuses hyperplasia. Childs Nerv Syst. 22:605–608. 2006.
Article15. Thomale UW. Integrated understanding of hydrocephalus - a practical approach for a complex disease. Childs Nerv Syst. 37:3313–3324. 2021.
Article16. Welch K, Strand R, Bresnan M, Cavazzuti V. Congenital hydrocephalus due to villous hypertrophy of the telencephalic choroid plexuses. Case report. J Neurosurg. 59:172–175. 1983.
Article17. Zahl SM, Egge A, Helseth E, Wester K. Clinical, radiological, and demographic details of benign external hydrocephalus: a population-based study. Pediatr Neurol. 96:53–57. 2019.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MR Findings of Choroid Plexus Papilloma: Case Report
- A Case of Choroid Plexus Carcinoma with Rapid Dissemination after Gross Total Resection
- A Case of Lateral Ventricle Choroid Plexus Papilloma in a Child
- A Choroid Plexus Papilloma in Cerebellopontine Angle: Case Report
- A Case of Lateral Ventricle Choroid Plexus Papilloma in an Infant
