Congenital Intracranial Vascular Malformations in Children : Radiological Overview
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul, Korea
- 2Department of Radiology, Seoul National University College of Medicine, Seoul, Korea
- 3Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea
- 4Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2554864
- DOI: http://doi.org/10.3340/jkns.2024.0033
Abstract
- Prompt medical attention is crucial for congenital intracranial vascular malformations in children and newborns due to potential severe outcomes. Imaging is pivotal for accurate identification, given the diverse risks and treatment strategies. This article aims to enhance the identification and understanding of congenital intracranial vascular abnormalities including arteriovenous malformation, arteriovenous fistula, cavernous malformation, capillary telangiectasia, developmental venous anomaly, and sinus pericranii in pediatric patients.
Keyword
Figure
-
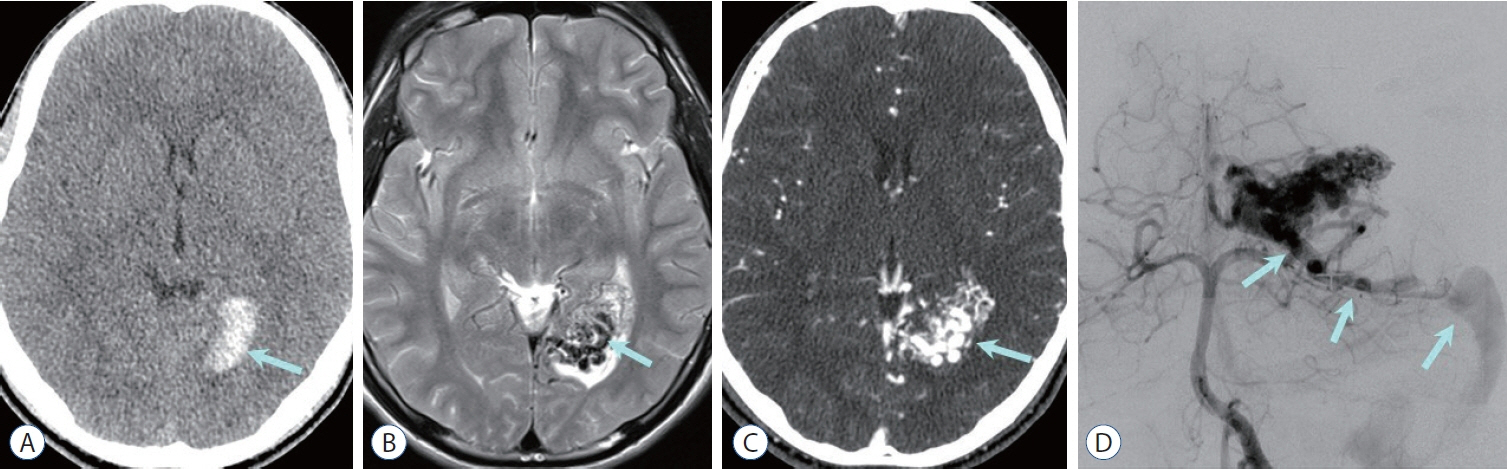
Fig. 1. Arteriovenous malformation (AVM) with compact nidus. A : Non-contrast computed tomography (CT) image shows high density hematoma in the left occipital lobe (arrow). B : Axial T2-weighted image shows compactly entangled flow voids mass (nidus, arrow) without any interposed normal brain tissue, which is surrounded by edematous parenchyma associated with hemorrhage. C : The nidus (arrow) is intensely enhanced on CT angiography. D : Vertebral arteriography reveals densely packed vascular nidus supplied by the left posterior cerebral artery, and early draining vein to the transverse sinus via superior cerebellar vein (arrows).
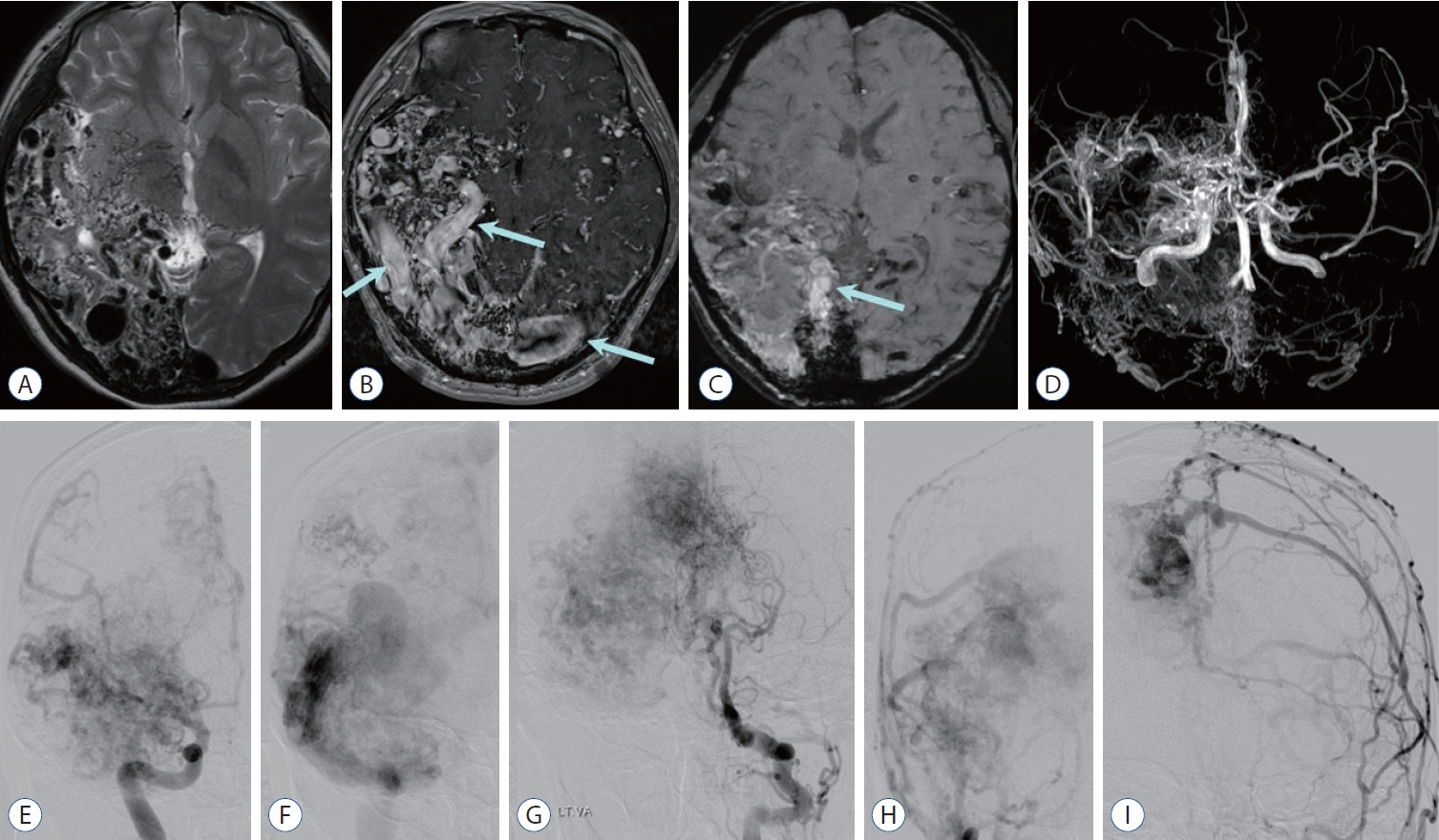
Fig. 2. Cerebral proliferative angiopathy : diffuse or proliferative type arteriovenous malformation. A : Axial T2-weighted image shows diffuse or proliferative type of nidus and interspersion of normal brain parenchyma involving right temporo-occipital lobes and basal ganglia. B : Contrast enhanced T1-weighted image shows diffuse network of enhancing vascular nidus and dilated draining veins (arrows). C : Susceptibility-weighted image shows multifocal blood products of dark signal intensity and dilated veins exhibiting high signal intensities reflecting rapid arteriovenous shunting (arrow). D : Magnetic resonance angiography reveals scattered nidus fed by multiple arteries (absence of a dominant feeder) including both anterior and posterior circulation, and transdural supplies from the external carotid artery (ECA) branches. E-I : Anterior-posterior projection of angiographic images obtained after contrast injection at the right internal cerebral artery (E and F), left vertebral artery (G), and both ECAs (H and I) reveal fuzzy appearance of nidus and scattered “puddling” of contrast which persists into the late arterial and venous phases. There are numerous feeders of normal size or moderately enlarged from internal cerebral artery, posterior cerebral artery, and ECA branches, and paucity of early venous drainage.
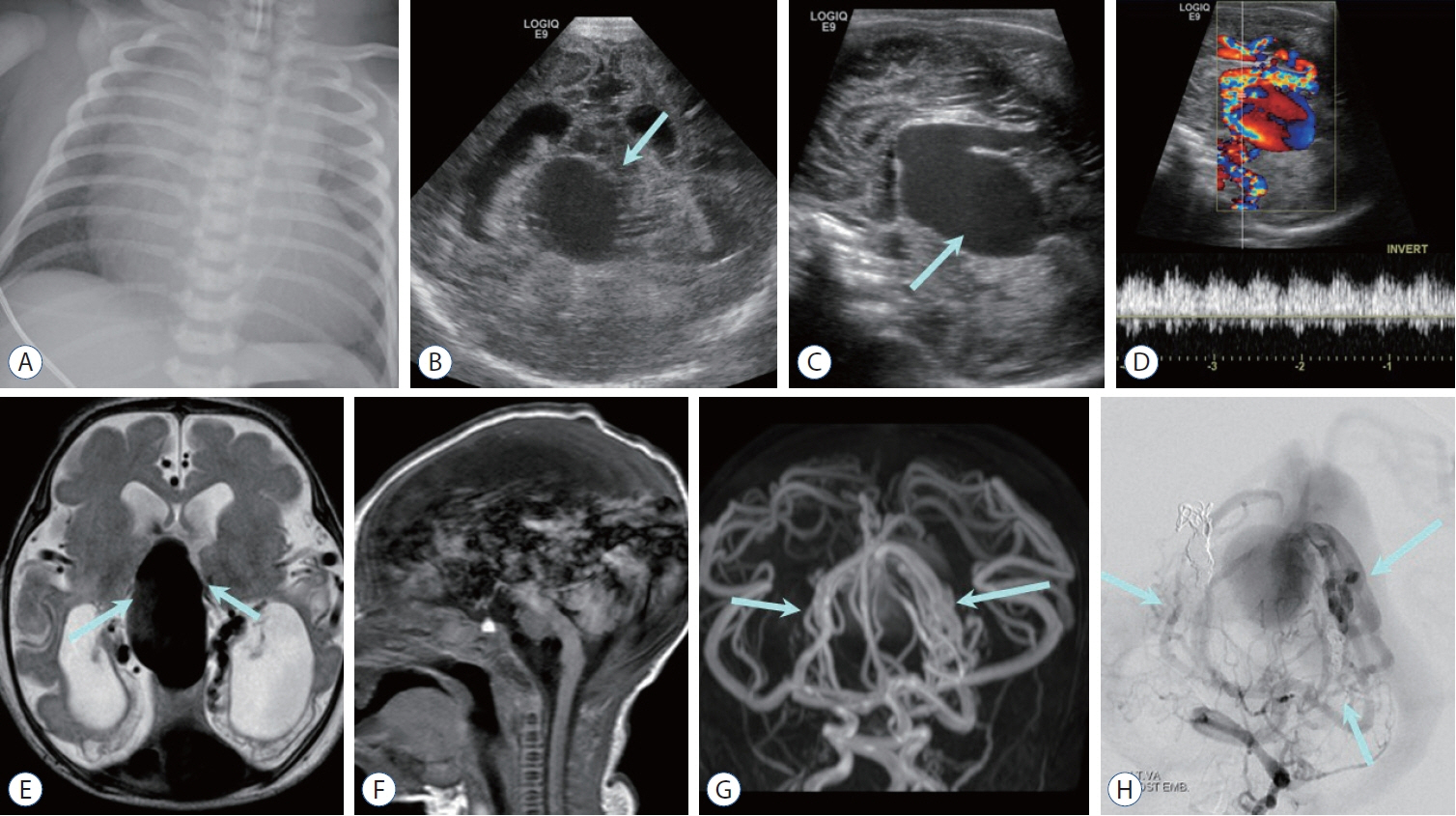
Fig. 3. Choroidal type vein of Galen aneurysmal malformation (VGAM) in a neonate with congestive heart failure. A : Chest radiography shows enlarged heart in keeping with congestive heart failure. Coronal (B) and sagittal (C) cranial sonographic images show midline vascular mass (arrow) and distended ventricles. D : Color Doppler image demonstrates vein of Galen aneurysm with turbulent vascular flow. E : Axial T2-weighted image shows large midline varix with adjacent multiple feeders (arrows), ventriculomegaly, and encephalomalacia in bilateral occipital lobes presumed from venous congestion and arterial steal from VGAM. F : Sagittal T1-weighted image shows prominent phase encoding pulsating artifact from the varix. Magnetic resonance angiography (G) reveals numerous small feeding arteries (arrows), which is more apparent on left vertebral artery angiography (H, arrows).
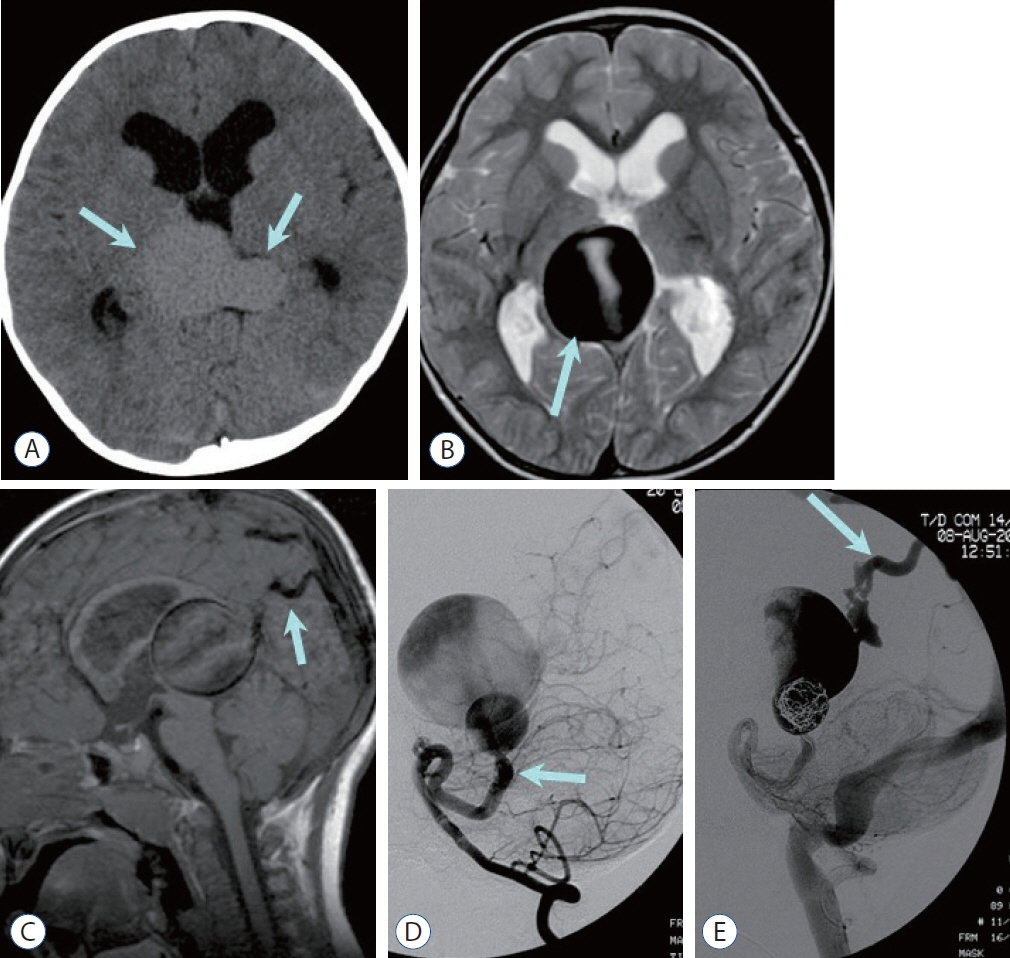
Fig. 4. Mural type vein of Galen aneurysmal malformation in a 3-year-old boy. A : Noncontrast computed tomography image shows large central venous varix (arrows) and enlarged ventricles. B : T2-weighted image demonstrates dark signal intensity of the dilated vein (arrow) with phase misregistration artifact due to the vascular flow. C : Sagittal T1-weighted image demonstrates markedly dilated central vein (vein of Galen) connected to the falcine sinus (arrow) and prominent phase misregistration artifact. Note the hydrocephalus caused by mass effect of dilated central vein on cerebral aqueduct. D : Lateral projection of the left vertebral arteriography at the arterial phase shows connection (mural type) between the dilated left superior cerebellar artery (arrow) and dilated median prosencephalic vein of Markovski (vein of Galen). E : Lateral projection of the left vertebral arteriography after coil embolization reveals contrast filling the vein of Galen drained into the transverse sinus and jugular vein via the falcine sinus (arrow). Note the absence of the straight sinus.
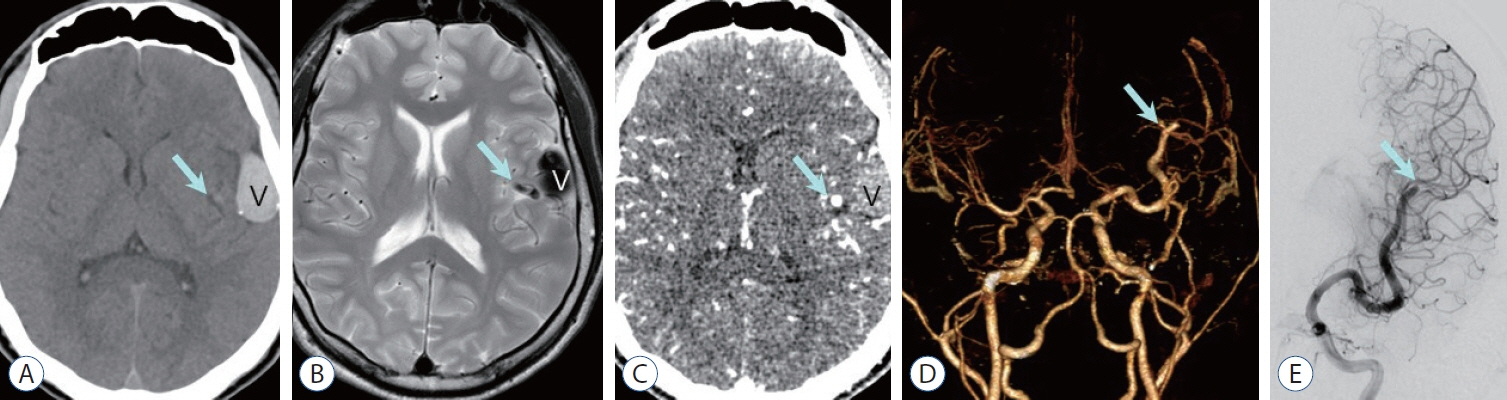
Fig. 5. Pial arteriovenous fistula in a 2-year-old boy. Non-contrast computed tomography (CT) (A) shows high density venous pouch (V) on the surface of the left insula and a small round high density medially (arrow in A), which is traced as a signal void tubular structure (arrow in B) on T2-weighted image suggesting dilated high-flow feeder. The dilated venous pouch is also seen as dark signal intensity on T2-weighted image (B). an axial image (C) and a 3D-reconstruction image (D) of CT angiography demonstrate dilatated left distal middle cerebral artery (MCA) as a feeder artery (arrow, C and D) with intense enhancement (C), while the venous pouch is not enhanced suggesting thrombotic occlusion (V). E : anterior-posterior projection of the left internal cerebral angiography shows dilated MCA feeder (arrow) and non-visualized venous pouch.
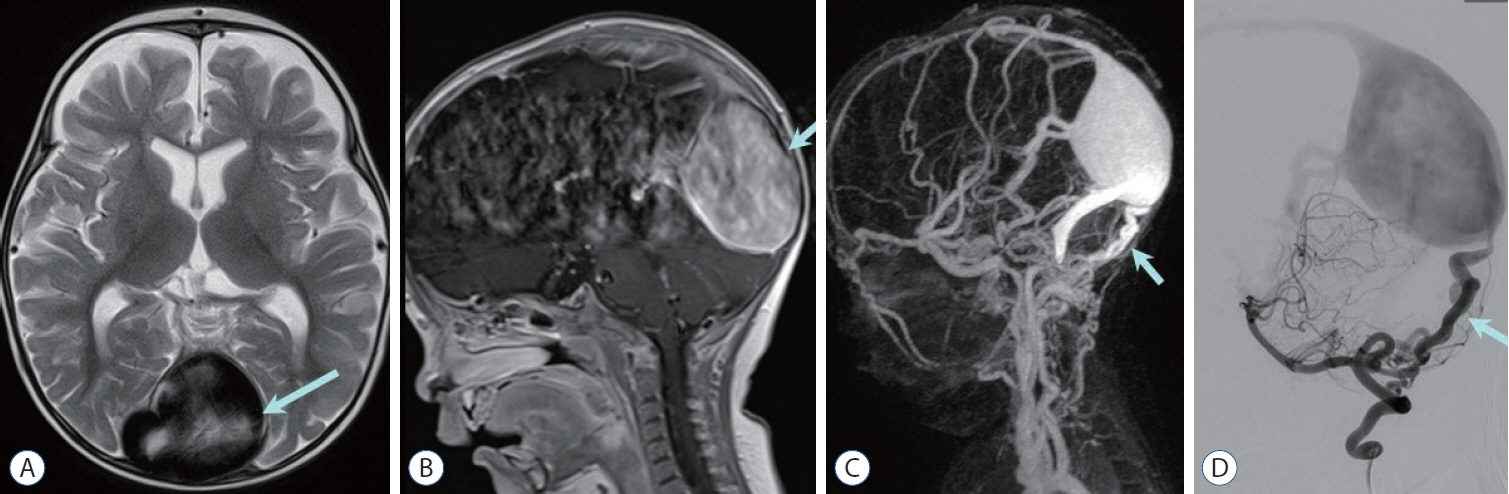
Fig. 6. Dural arteriovenous fistula with dural sinus malformation in a 7-month-old boy. a massively dilated torcular herophilli (arrow) is visualized on axial T2-weighted image (A) and sagittal contrast enhanced T1-weighted image (B). C : Contrast enhanced magnetic resonance venography shows tortuous vertebral artery branches (arrow) supplying dilated torcular herophilli and transverse sinus. D : Lateral projection of left vertebral arteriography shows engorged posterior meningeal branches (arrow) communicating to the torcula herophilli with reflux to superior sagittal sinus.
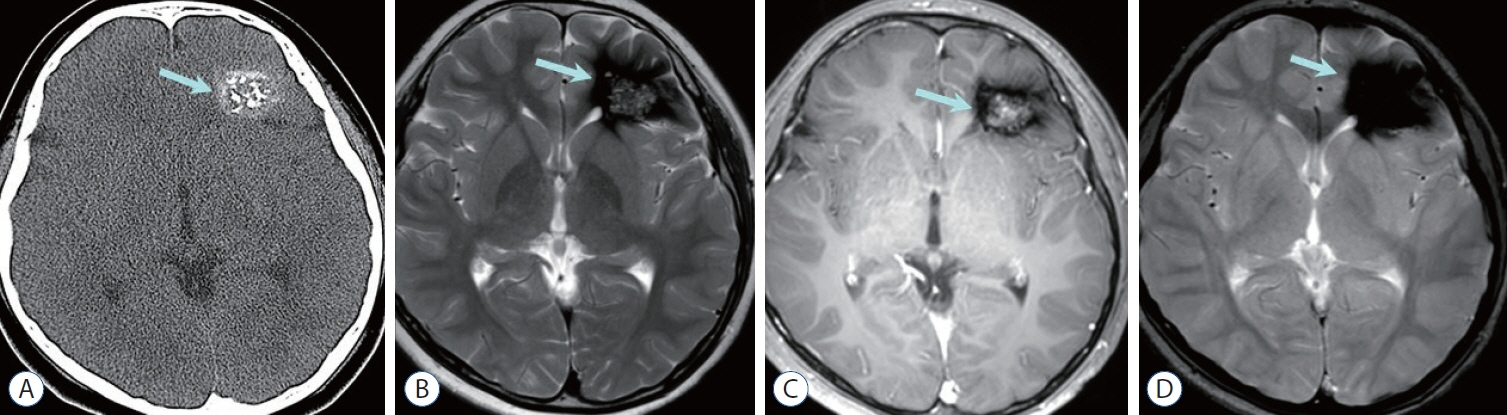
Fig. 7. Cavernous malformation. A : Non-contrast computed tomography shows high-attenuated mass containing multiple calcifications in the left frontal lobe (arrow). B : Left frontal mass is seen as central heterogeneous high signal intensity surrounded by dark area of hemosiderin deposition, so called popcorn-like appearance (arrow) on axial T2-weighted image. C : Central portion of the mass (arrow) shows heterogeneous enhancement on contrast enhanced T1-weighted image. D : Prominent blooming dark signal intensity (arrow) is seen on gradient echo image suggesting blood product.
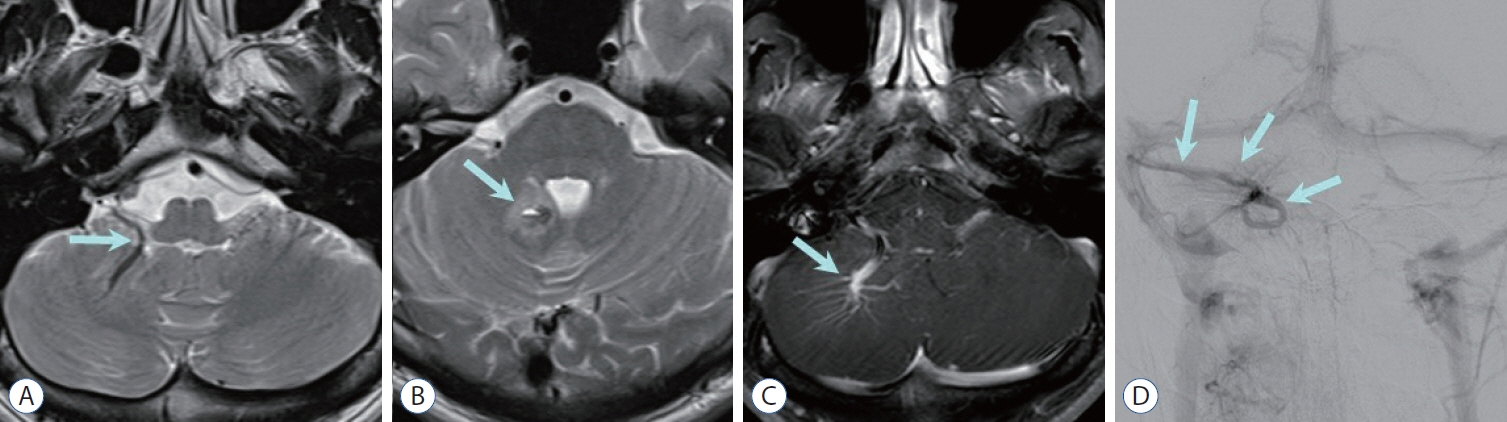
Fig. 8. Developmental venous anomaly (DVA). A and B : axial T2-weighted images show curvilinear collecting vein suggesting DVa (arrow in A) and adjacent small hemorrhagic cysts surrounded by edema (arrow in B) suggesting coexisting cavernous malformation. C : Contrast enhanced T1-weighted image reveals enhancing collecting vein and dilated medullary veins showing ‘caput medusa’ sign (arrow). D : Dilated medullary veins converging on transcortical collecting vein (arrows) are well demonstrated on a delayed phase of the vertebral arteriography.
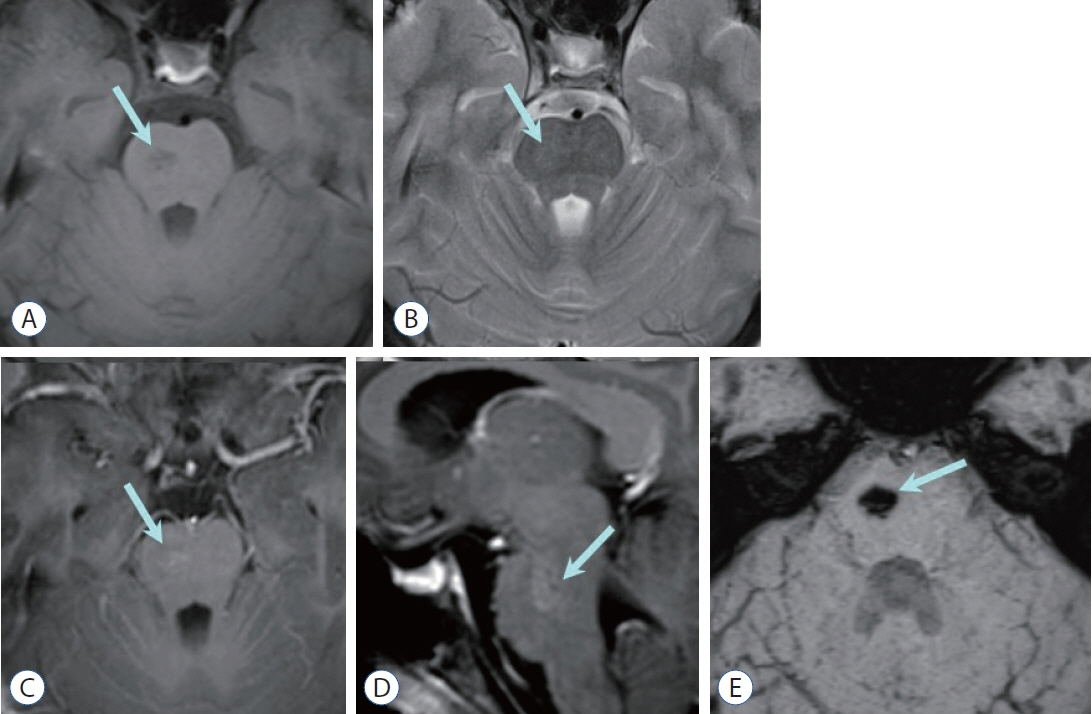
Fig. 9. Capillary telangiectasia. A : axial T1-weighted image shows a small, poorly marginated, pontine lesion (arrow) of low signal intensity without mass effect nor edema (arrow). B : The pontine lesion (arrow) is very subtle and faintly visualized on T2-weighted image. Contrast enhanced axial (C) and sagittal (D) T1-weighted images reveal stippled/brush-like enhancement (arrow). E : Profound hypointense pontine lesion (arrow) is well visualized on susceptibility-weighted image.
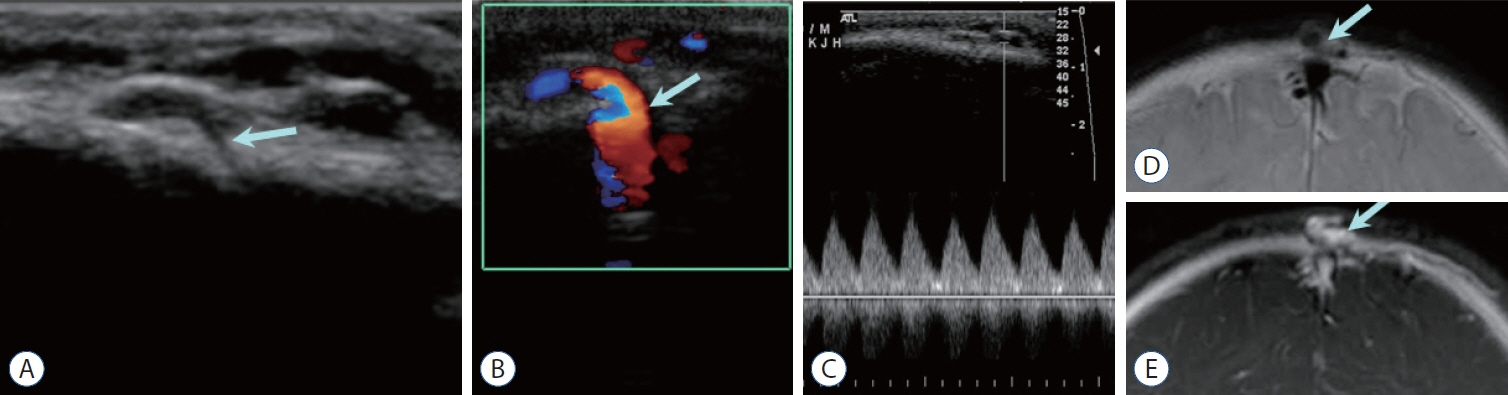
Fig. 10. Sinus pericranii. A : Sonography shows lobulated cystic lesions in the scalp at the vertex, with a connection to the underlying dural sinus (arrow). Color Doppler image (B) demonstrates prominent vascular flow (arrow in B) connecting the scalp lesion and dural sinus, with pulsatile spectral waves (C). Coronal T2-weighted image (D) and contrast enhanced T1-weighted image (E) show signal void (arrow in D) or enhancement (arrow in E) of the scalp vein connecting to the superior sagittal sinus.
Reference
-
References
1. Alvarez H, Garcia Monaco R, Rodesch G, Sachet M, Krings T, Lasjaunias P. Vein of galen aneurysmal malformations. Neuroimaging Clin N Am. 17:189–206. 2007.
Article2. Burch EA, Orbach DB. Pediatric central nervous system vascular malformations. Pediatr Radiol. 45 Suppl 3:S463–S472. 2015.
Article3. Chen CJ, Ding D, Derdeyn CP, Lanzino G, Friedlander RM, Southerland AM, et al. Brain arteriovenous malformations: a review of natural history, pathobiology, and interventions. Neurology. 95:917–927. 2020.4. Darsaut TE, Guzman R, Marcellus ML, Edwards MS, Tian L, Do HM, et al. Management of pediatric intracranial arteriovenous malformations: experience with multimodality therapy. Neurosurgery. 69:540–556. discussion 556. 2011.
Article5. Geibprasert S, Pongpech S, Jiarakongmun P, Shroff MM, Armstrong DC, Krings T. Radiologic assessment of brain arteriovenous malformations: what clinicians need to know. Radiographics. 30:483–501. 2010.
Article6. Hacein-Bey L, Konstas AA, Pile-Spellman J. Natural history, current concepts, classification, factors impacting endovascular therapy, and pathophysiology of cerebral and spinal dural arteriovenous fistulas. Clin Neurol Neurosurg. 121:64–75. 2014.
Article7. Hetts SW, Moftakhar P, Maluste N, Fullerton HJ, Cooke DL, Amans MR, et al. Pediatric intracranial dural arteriovenous fistulas: age-related differences in clinical features, angioarchitecture, and treatment outcomes. J Neurosurg Pediatr. 18:602–610. 2016.
Article8. Jaimes C, Machado-Rivas F, Chen K, Bedoya MA, Yang E, Orbach DB. Brain injury in fetuses with vein of Galen malformation and nongalenic arteriovenous fistulas: static snapshot or a portent of more? AJNR Am J Neuroradiol. 43:1036–1041. 2022.
Article9. Krings T, Geibprasert S, Terbrugge K. Classification and endovascular management of pediatric cerebral vascular malformations. Neurosurg Clin N Am. 21:463–482. 2010.
Article10. Liby P, Lomachinsky V, Petrak B, Kyncl M, Charvat F, Padr R, et al. Torcular dural sinus malformations: a single-center case series and a review of literature. Childs Nerv Syst. 36:333–341. 2020.
Article11. LoPresti MA, Ravindra VM, Pyarali M, Goethe E, Gadgil N, Wagner K, et al. Pediatric intracranial arteriovenous malformations: a single-center experience. J Neurosurg Pediatr. 25:151–158. 2019.
Article12. Maleknia PD, Hale AT, Savage C, Blount JP, Rocque BG, Rozzelle CJ, et al. Characteristics and outcomes of pediatric dural arteriovenous fistulas: a systematic review. Childs Nerv Syst. 40:197–204. 2024.
Article13. Mansmann U, Meisel J, Brock M, Rodesch G, Alvarez H, Lasjaunias P. Factors associated with intracranial hemorrhage in cases of cerebral arteriovenous malformation. Neurosurgery. 46:272–279. discussion 279-281. 2000.
Article14. Mokin M, Dumont TM, Levy EI. Novel multimodality imaging techniques for diagnosis and evaluation of arteriovenous malformations. Neurol Clin. 32:225–236. 2014.
Article15. Montaser A, Smith ER. Intracranial vascular abnormalities in children. Pediatr Clin North Am. 68:825–843. 2021.
Article16. Mossa-Basha M, Chen J, Gandhi D. Imaging of cerebral arteriovenous malformations and dural arteriovenous fistulas. Neurosurg Clin N Am. 23:27–42. 2012.
Article17. Paddock M, Lanham S, Gill K, Sinha S, Connolly DJA. Pediatric cerebral cavernous malformations. Pediatr Neurol. 116:74–83. 2021.
Article18. Rai Y, Ogiwara H. Atretic cephalocele associated with sinus pericranii: a single-center analysis. Childs Nerv Syst. 40:543–547. 2024.
Article19. Ravindra VM, Bollo RJ, Eli IM, Griauzde J, Lanpher A, Klein J, et al. A study of pediatric cerebral arteriovenous malformations: clinical presentation, radiological features, and long-term functional and educational outcomes with predictors of sustained neurological deficits. J Neurosurg Pediatr. 24:1–8. 2019.
Article20. Recinos PF, Rahmathulla G, Pearl M, Recinos VR, Jallo GI, Gailloud P, et al. Vein of Galen malformations: epidemiology, clinical presentations, management. Neurosurg Clin N Am. 23:165–177. 2012.
Article21. Requejo F, Teplisky D, Dutra MLG, Mouratian DM, Kikano R, Nguyen TN, et al. Pediatric interventional neuroradiology. Semin Neurol. 43:408–418. 2023.
Article22. Ruíz DS, Yilmaz H, Gailloud P. Cerebral developmental venous anomalies: current concepts. Ann Neurol. 66:271–283. 2009.23. Sabayan B, Lineback C, Viswanathan A, Leslie-Mazwi TM, Shaibani A. Central nervous system vascular malformations: a clinical review. Ann Clin Transl Neurol. 8:504–522. 2021.24. Santos AN, Rauschenbach L, Saban D, Chen B, Herten A, Dinger TF, et al. Natural course of cerebral cavernous malformations in children: a five-year follow-up study. Stroke. 53:817–824. 2022.25. Sarma A, Martin D, Pruthi S, Jones R, Little SB. Imaging the cerebral veins in pediatric patients: beyond dural venous sinus thrombosis. Radiographics. 43:e220129. 2023.26. Shtaya A, Millar J, Sparrow O. Multimodality management and outcomes of brain arterio-venous malformations (AVMs) in children: personal experience and review of the literature, with specific emphasis on age at first AVM bleed. Childs Nerv Syst. 33:573–581. 2017.27. Zuniega RRA, Santos JA, Galsim RJG, Elevazo JS. Neonatal giant dural sinus ectasia: a multimodality imaging approach. BMJ Case Rep. 14:e242439. 2021.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pediatric Cerebral Vascular Malformations : Current and Future Perspectives
- 3 Cases of Surgically Treated Arteriovenous Malformations of the Brain
- Imaging of Intracranial Hemorrhage
- Spontaneous Intracranial Hemorrhage in Children: Analysis of Clinical Characteristics
- A Review of the Current State and Future Directions for Management of Scalp and Facial Vascular Malformations
