Treatment of a posterior cerebral artery aneurysm in the context of complex cardio-cerebrovascular variations using the Tubridge flow diverter
- Affiliations
-
- 1Neuroendovascular Program, Massachusetts General Hospital & Brigham and Women’s Hospital, Harvard Medical School, Boston, USA
- 2Neurovascular Centre, Departments of Medical Imaging & Neurosurgery, St. Michael’s Hospital, University of Toronto, Toronto, Canada
- 3Department of Neurosurgery and Laboratory of Neurosurgery, Lanzhou University Second Hospital, Lanzhou, People’s Republic of China
- 4Institute of Neurology, Lanzhou University, Lanzhou, People’s Republic of China
- KMID: 2554048
- DOI: http://doi.org/10.7461/jcen.2023.E2023.04.009
Abstract
- We present a case of intracranial aneurysm located in the P1 segment of left posterior cerebral artery in the context of tetralogy of Fallot. Complex variations included right aortic arch with abnormal branching. Also, the bilateral vertebral arteries were absent, with a type I persistent proatlantal intersegmental artery of the left side. The aneurysm was treated with endovascular intervention with a Tubridge flow diverter and was noted to be completely cured on 6-month follow-up. We discuss the many considerations in this patient including developmental and modern-era treatment.
Keyword
Figure
-

Fig. 1. (A, B) Echocardiography illustrating TOF with pulmonic stenosis. (C, D) MRI T2 weighted imaging depicting left PCA aneurysm (arrow) and remote infarctions in the right frontal and parietal lobes (arrows). TOF, tetralogy of Fallot; MRI, magnetic resonance imaging; PCA, posterior cerebral artery
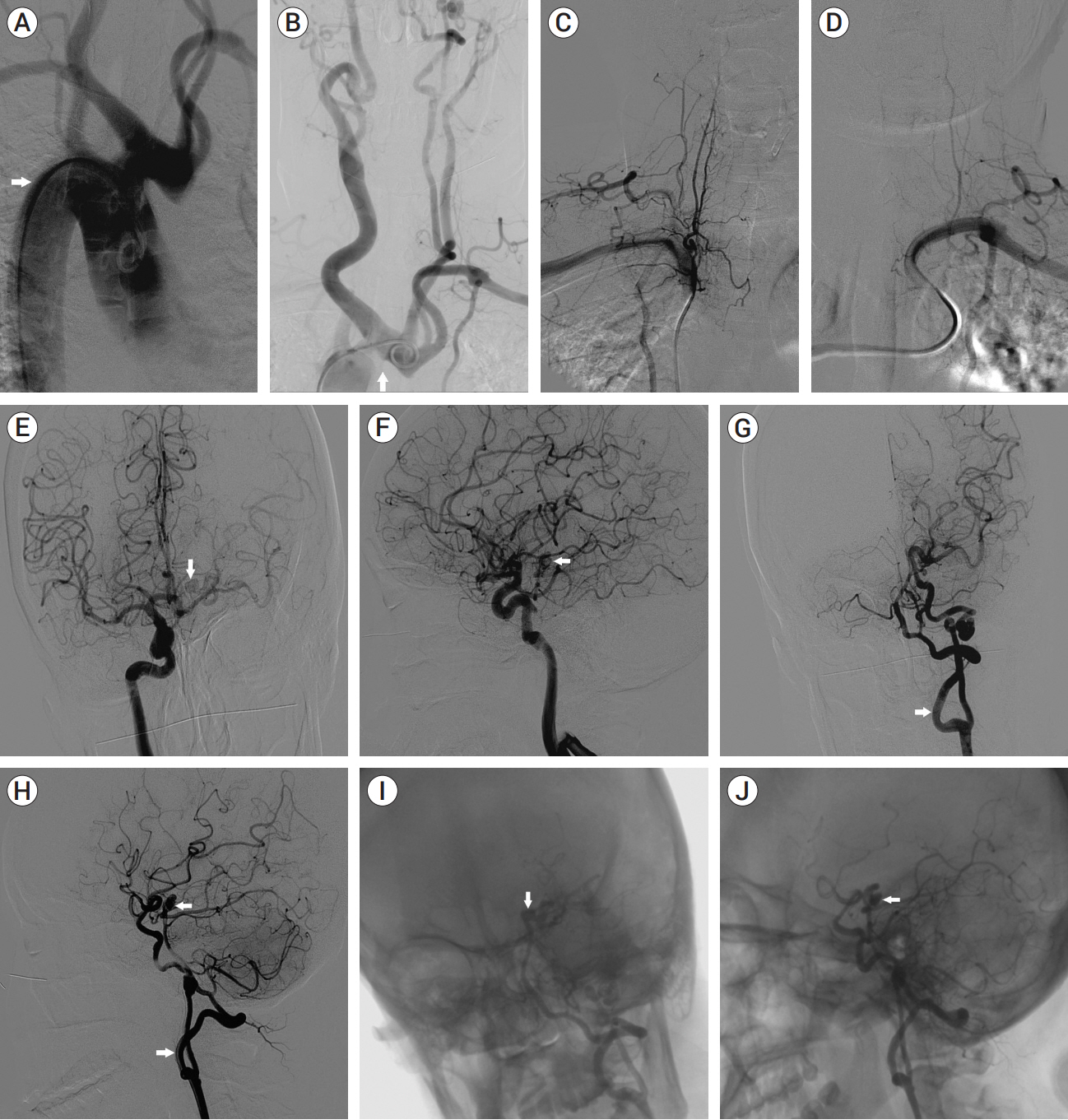
Fig. 2. (A, B) Aortic arch angiography (arrow): RAA; the right CCA, left ICA, left ECA and left SA all branched from a common main trunk from the aortic arch. (C, D) SA angiography: bilateral VAs absent. (E, F) Right ICA angiography: patent anterior communicating artery (arrow), right embryonic posterior cerebral artery, and left PCA aneurysm (arrow). (G, H) Left ICA angiography: PIA (arrow). (I, J) left ICA angiography: P1 segment aneurysm (arrow). RAA, right aortic arch; CCA, common carotid artery; ICA, internal carotid artery; ECA, external carotid artery; SA, subclavian artery; VA, vertebral artery; PCA, posterior cerebral artery; PIA, proatlantal intersegmental artery
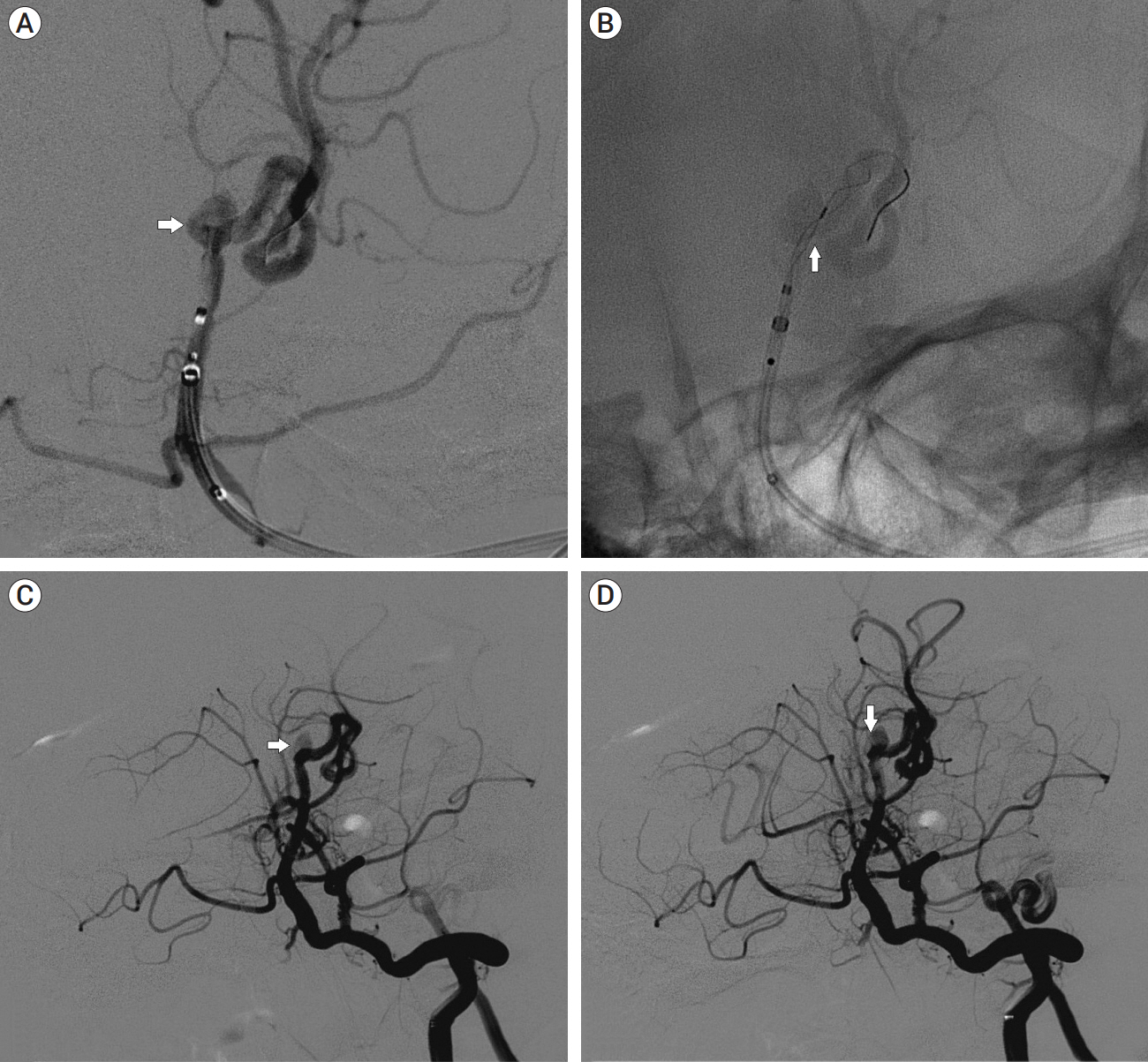
Fig. 3. (A, B) Intraoperative angiography: a saccular wide-necked aneurysm (arrow) in the P1 segment of the left PCA (diameter: body 5.2×3.7 mm, neck 3.1 mm, parent artery 2.3 mm); Tubridge (arrow) FD (2.5/20 mm) semi-release and covering the neck of the aneurysm. (C, D) Immediate angiography after Tubridge FD implantation: decreased contrast filling into the aneurysm sac (arrow). PCA, posterior cerebral artery; FD, flow diverter
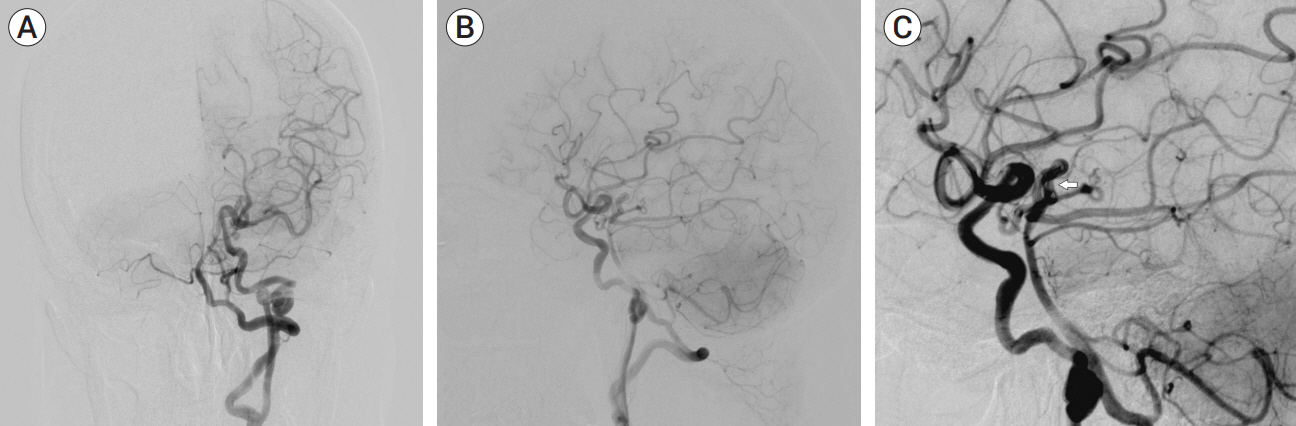
Fig. 4. (A-C) Left ICA angiography at 6-month follow-up: left P1 aneurysm not visible (arrow) and cured clinically. ICA, internal carotid artery
Reference
-
1. Ammash N, Warnes CA. Cerebrovascular events in adult patients with cyanotic congenital heart disease. J Am Coll Cardiol. 1996; Sep. 28(3):768–72.
Article2. Fiorda-Diaz J, Shabsigh M, Dimitrova G, Soghomonyan S, Sandhu G. Perioperative management of subarachnoid hemorrhage in a patient with alagille syndrome and unrepaired tetralogy of Fallot: Case report. Front Surg. 2017; Dec. 4:72.
Article3. Iida Y, Nagamine H, Nomura M. Right aortic arch associated with left internal carotid artery agenesis. NMC Case Rep J. 2017; Jun. 4(3):79–82.
Article4. Ojha V, Vadher A, Chandrashekhara SH, Malhi AS, Nayak SK, Kumar S. A unique case of separate origins of left internal and external carotid arteries from high aortic arch with aberrant right subclavian artery - An unreported association in tetralogy of Fallot. J Cardiovasc Comput Tomogr. 2020; Sep-Oct. 14(5):e71–2.
Article5. Sato H, Fujiwara S, Otabe K, Sato S. A case of persistent primitive proatlantal intersegmental artery (proatlantal artery I) with aneurysm--A case report. No Shinkei Geka. 1985; Jan. 13(1):117–21.6. Uchino A, Saito N, Kozawa E, Masutani S. Multiple variations of the cerebral arteries associated with tetralogy of Fallot: A case report. Surg Radiol Anat. 2017; Oct. 39(10):1161–4.
Article7. Van Praagh R. What determines whether the great arteries are normally or abnormally related? Am J Cardiol. 2016; Nov. 118(9):1390–8.
Article8. Yilmaz E, Ilgit E, Taner D. Primitive persistent carotid-basilar and carotid-vertebral anastomoses: A report of seven gases and a review of the literature. Clin Anat. 1995; 8(1):36–43.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clipping of a persistent middle cerebral artery aneurysm after previous flow diverter placement: An illustrative case and review of the literature
- Kinking of Flow Diverter in a Giant Wide-Necked Supraclinoid Internal Carotid Artery Aneurysm
- A Novel Flow Diverter (Tubridge) for the Treatment of Recurrent Aneurysms: A Single-Center Experience
- Salvage flow diverter stent across the posterior communicating artery for persistent retrograde filling of a giant internal carotid artery aneurysm after parent vessel occlusion
- Flow Diverter Device for Treatment of Cerebral Aneurysm with Short-Term Follow Up: Two Case Reports
