22-gauge Co-Cr versus stainless-steel Franseen needles for endoscopic ultrasound-guided tissue acquisition in patients with solid pancreatic lesions
- Affiliations
-
- 1Department of Gastroenterology, Saitama Medical University International Medical Center, Saitama, Japan
- KMID: 2553761
- DOI: http://doi.org/10.5946/ce.2023.011
Abstract
- Background/Aims
Endoscopic ultrasound-guided tissue acquisition (EUS-TA) using Franseen needles is reportedly useful for its high diagnostic yield. This study compared the diagnostic yield and puncturing ability of EUS-TA using 22-gauge cobalt-chromium (CO-Cr) needles with those of stainless-steel Franseen needles in patients with solid pancreatic lesions.
Methods
Outcomes were compared between the 22-gauge Co-Cr Franseen needle (December 2019 to November 2020; group C) and stainless-steel needle (November 2020 to May 2022; group S).
Results
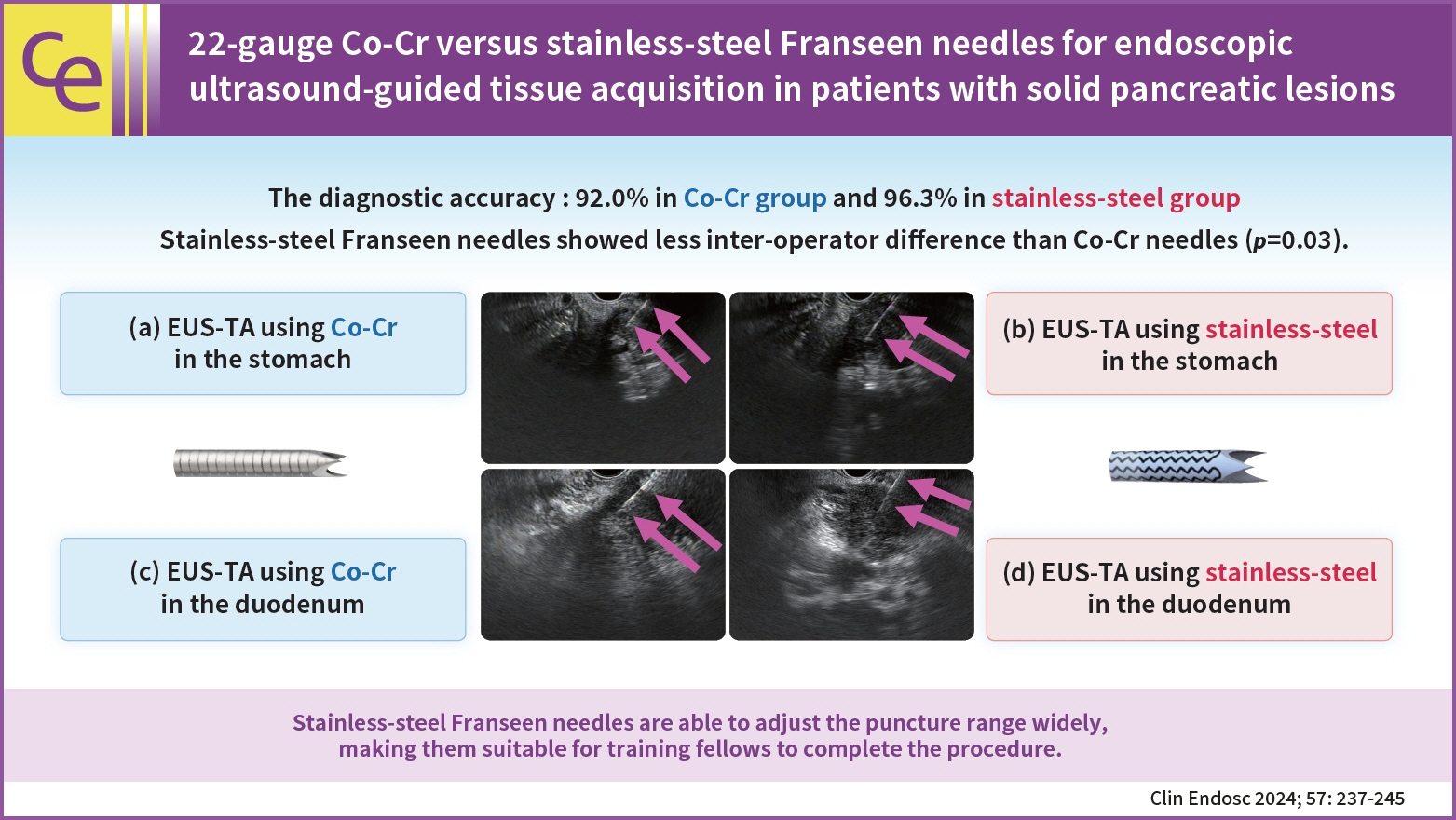
A total of 155 patients (group C, 75; group S, 80) were eligible. The diagnostic accuracy was 92.0% in group C and 96.3% in group S with no significant intergroup differences (p=0.32). The rate of change in the operator (from training fellows to experts) was 20.0% (15/75) in group C and 7.5% (6/80) in group S. Stainless-steel Franseen needles showed less inter-operator difference than Co-Cr needles (p=0.03).
Conclusions
Both Co-Cr and stainless-steel Franseen needles showed high diagnostic ability. Stainless-steel Franseen needles are soft and flexible; therefore, the range of puncture angles can be widely adjusted, making them suitable for training fellows to complete the procedure.
Keyword
Figure
-
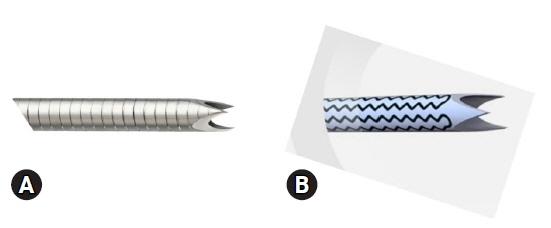
Fig. 1. Franseen needles for endoscopic ultrasound-guided tissue acquisition. (A) Cobalt-chromium Franseen needle. (B) Stainless-steel Franseen needle.
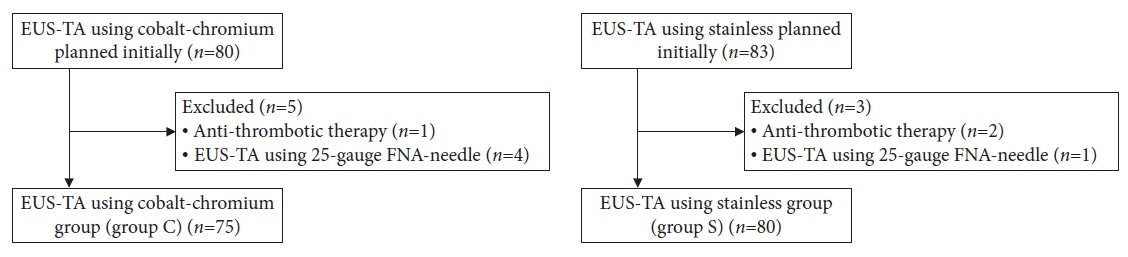
Fig. 2. Patient eligibility flowchart. EUS-TA, endoscopic ultrasound-guided tissue acquisition; FNA, fine-needle aspiration.
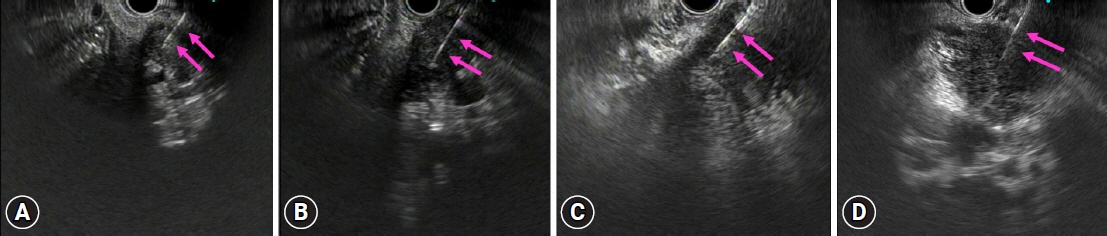
Fig. 3. Endoscopic ultrasound findings. Endoscopic ultrasound-guided tissue acquisition (EUS-TA) using cobalt-chromium (CO-Cr) (A) and stainless-steel Franseen needle (B) from the stomach when the elevator of the linear echoendoscope was fully used. Both needles are visible (pink arrows). No significant difference intergroup difference in puncture angles was noted. EUS-TA using Co-Cr (C) and stainless-steel Franseen needles (D) from the second portion of the duodenum when the elevator of the linear echoendoscope was fully used. Both needles are visible (pink arrows). The stainless-steel needles had a greater puncture angle than the Co-Cr needles.
Reference
-
1. Iglesias-Garcia J, Dominguez-Munoz JE, Abdulkader I, et al. Influence of on-site cytopathology evaluation on the diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) of solid pancreatic masses. Am J Gastroenterol. 2011; 106:1705–1710.2. Vilmann P, Săftoiu A, Hollerbach S, et al. Multicenter randomized controlled trial comparing the performance of 22 gauge versus 25 gauge EUS-FNA needles in solid masses. Scand J Gastroenterol. 2013; 48:877–883.3. Puli SR, Bechtold ML, Buxbaum JL, et al. How good is endoscopic ultrasound-guided fine-needle aspiration in diagnosing the correct etiology for a solid pancreatic mass?: a meta-analysis and systematic review. Pancreas. 2013; 42:20–26.4. Iwashita T, Yasuda I, Doi S, et al. Use of samples from endoscopic ultrasound-guided 19-gauge fine-needle aspiration in diagnosis of autoimmune pancreatitis. Clin Gastroenterol Hepatol. 2012; 10:316–322.5. Bang JY, Hebert-Magee S, Trevino J, et al. Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions. Gastrointest Endosc. 2012; 76:321–327.6. Iwashita T, Nakai Y, Samarasena JB, et al. High single-pass diagnostic yield of a new 25-gauge core biopsy needle for EUS-guided FNA biopsy in solid pancreatic lesions. Gastrointest Endosc. 2013; 77:909–915.7. Fujita A, Ryozawa S, Tanisaka Y, et al. Evaluation of endoscopic ultrasound-guided fine-needle biopsy for preoperative pancreatic solid lesions. Scand J Gastroenterol. 2021; 56:188–192.8. Tanisaka Y, Mizuide M, Fujita A, et al. Comparison of endoscopic ultrasound-guided fine-needle aspiration and biopsy device for lymphadenopathy. Gastroenterol Res Pract. 2021; 2021:6640862.9. Itonaga M, Yasukawa S, Fukutake N, et al. Comparison of 22-gauge standard and Franseen needles in EUS-guided tissue acquisition for diagnosing solid pancreatic lesions: a multicenter randomized controlled trial. Gastrointest Endosc. 2022; 96:57–66.10. Kandel P, Nassar A, Gomez V, et al. Comparison of endoscopic ultrasound-guided fine-needle biopsy versus fine-needle aspiration for genomic profiling and DNA yield in pancreatic cancer: a randomized crossover trial. Endoscopy. 2021; 53:376–382.11. Ikeda G, Hijioka S, Nagashio Y, et al. Fine-needle biopsy with 19G needle is effective in combination with endoscopic ultrasound-guided tissue acquisition for genomic profiling of unresectable pancreatic cancer. Dig Endosc. 2023; 35:124–133.12. Bang JY, Hebert-Magee S, Hasan MK, et al. Endoscopic ultrasonography-guided biopsy using a Franseen needle design: initial assessment. Dig Endosc. 2017; 29:338–346.13. Mukai S, Itoi T, Yamaguchi H, et al. A retrospective histological comparison of EUS-guided fine-needle biopsy using a novel franseen needle and a conventional end-cut type needle. Endosc Ultrasound. 2019; 8:50–57.14. Kurita A, Yasukawa S, Zen Y, et al. Comparison of a 22-gauge Franseen-tip needle with a 20-gauge forward-bevel needle for the diagnosis of type 1 autoimmune pancreatitis: a prospective, randomized, controlled, multicenter study (COMPAS study). Gastrointest Endosc. 2020; 91:373–381.15. Ishigaki K, Nakai Y, Sasahira N, et al. A prospective multicenter study of endoscopic ultrasound-guided fine needle biopsy using a 22-gauge Franseen needle for pancreatic solid lesions. J Gastroenterol Hepatol. 2021; 36:2754–2761.16. Nakai Y, Isayama H, Chang KJ, et al. Slow pull versus suction in endoscopic ultrasound-guided fine-needle aspiration of pancreatic solid masses. Dig Dis Sci. 2014; 59:1578–1585.17. Saxena P, El Zein M, Stevens T, et al. Stylet slow-pull versus standard suction for endoscopic ultrasound-guided fine-needle aspiration of solid pancreatic lesions: a multicenter randomized trial. Endoscopy. 2018; 50:497–504.18. Bor R, Vasas B, Fábián A, et al. Slow-pull technique yields better quality smears: prospective comparison of slow-pull and standard suction techniques of endoscopic ultrasound-guided fine-needle aspiration. Scand J Gastroenterol. 2020; 55:1369–1376.19. Matynia AP, Schmidt RL, Barraza G, et al. Impact of rapid on-site evaluation on the adequacy of endoscopic-ultrasound guided fine-needle aspiration of solid pancreatic lesions: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2014; 29:697–705.20. Kouanda A, Mclean R, Faggen A, et al. Telecytology versus in-room cytopathologist for EUS-guided FNA or fine-needle biopsy sampling of solid pancreatic lesions. Gastrointest Endosc. 2023; 97:466–471.21. Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010; 71:446–454.22. Bang JY, Hebert-Magee S, Navaneethan U, et al. Randomized trial comparing the Franseen and Fork-tip needles for EUS-guided fine-needle biopsy sampling of solid pancreatic mass lesions. Gastrointest Endosc. 2018; 87:1432–1438.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Ultrasound-Guided Tissue Acquisition by 22-Gauge Franseen and Standard Needles for Solid Pancreatic Lesions
- Comparison of Endoscopic Ultrasound-Guided Tissue Acquisition Using a 20-Gauge Menghini Needle with a Lateral Forward Bevel and a 22-Gauge Franseen Needle: A Single-Center Large Cohort Study
- Endoscopic ultrasound-guided tissue acquisition: Needle types, technical issues, and sample handling
- Comparison of the Diagnostic Yield of the Standard 22-Gauge Needle and the New 20-Gauge Forward-Bevel Core Biopsy Needle for Endoscopic Ultrasound-Guided Tissue Acquisition from Pancreatic Lesions
- Comparison of 19-gauge conventional and Franseen needles for the diagnosis of lymphadenopathy and classification of malignant lymphoma using endoscopic ultrasound fine-needle aspiration
