Basics for Pediatric Brain Tumor Imaging: Techniques and Protocol Recommendations
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, Seoul, Korea
- KMID: 2552334
- DOI: http://doi.org/10.14791/btrt.2023.0037
Abstract
- This review provides an overview of the current state of pediatric brain tumor imaging, emphasizing the role of various imaging sequences and highlighting the advantages of standardizing protocols for pediatric brain tumor imaging in diagnosis and treatment response evaluation. Basic anatomical sequences such as pre- and post-contrast 3D T1-weighted, T2-weighted, fluid-attenuated inversion recovery, T2*-weighted, and diffusion-weighted imaging (DWI), are fundamental for assessing tumor location, extent, and characteristics. Advanced techniques like DWI, diffusion tensor imaging, perfusion imaging, magnetic resonance spectroscopy, and functional MRI offer insights into cellularity, vascularity, metabolism, and function. To enhance consistency and quality, standardized protocols for pediatric brain tumor imaging have been recommended by expert groups. Special considerations for pediatric patients, including the minimization of anesthesia exposure and gadolinium contrast agent usage, are essential to ensure patient safety and comfort. Staying up-to-date with diagnostic imaging techniques can contribute to improved communication, outcomes, and patient care in the field of pediatric neurooncology.
Keyword
Figure
-

Fig. 1 Variable T1 hyperintensity in brain tumors. A: A newborn’s cranial ultrasound reveals a hyperechoic lesion in the superior vermis (arrow). B: Sagittal T1-weighted image displays a T1 hyperintense lesion (arrow), corresponding to the ultrasound demonstrated hyperechoic lesion, indicative of a lipoma. C: Axial T1-weighted image of a pineal mixed germ cell tumor shows multifocal T1 hyperintensities attributed to its fat components (arrows).

Fig. 2 Loss of expected T1 bright signal in germinoma. A: Unenhanced sagittal T1-weighted image shows the expected T1 bright signal of the posterior pituitary gland (arrow) due to vasopressin storage. B: Unenhanced sagittal T1-weighted image from a 13-year-old boy with diabetes insipidus shows the absence of the T1 bright signal of the posterior pituitary gland (arrow). C: Post-contrast sagittal T1-weighted image exhibits equivocal thickening of the pituitary stalk (arrow). D: A subsequent image 15 months later after the patient was lost to follow-up displays multifocal masses in the suprasellar and pineal regions with extensive ventricular seeding.
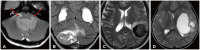
Fig. 3 Variable T2-weighted signal in brain tumors. A: Axial T2-weighted image shows a 4th ventricle mass extending through bilateral foramen Luschka (arrows), confirmed as posterior fossa ependymoma. B: Coronal T2-weighted image shows a heterogeneous, T2 hypointense mass in the right cerebellum causing a mass effect and edema, confirmed as medulloblastoma. C: Axial T2-weighted image depicts a T2 hypointense, hemorrhagic mass in the left parietal lobe accompanied by perilesional edema, confirmed as glioblastoma. D: Axial T2-weighted image reveals a large cystic and solid mass in the left cerebral hemisphere, diagnosed as supratentorial ependymoma.

Fig. 4 T2-fluid-attenuated inversion recovery (FLAIR) mismatch in IDH-mutant, 1p/19q non-codeleted astrocytoma. A: Axial T2-weighted image shows a well-demarcated T2 hyperintense mass in the right frontal lobe. B: Axial FLAIR image shows a FLAIR hypointense mass with a surrounding hyperintense rim, representing the “T2-FLAIR mismatch” sign.

Fig. 5 Variable enhancement patterns of pediatric brain tumors. A: Axial enhanced T1-weighted image shows a right thalamic mass with some enhancement, confirmed as pilocytic astrocytoma. B: Axial enhanced T1-weighted image depicts a well-enhancing heterogeneous mass involving the optic pathway, confirmed as pilocytic astrocytoma. C: Axial enhanced T1-weighted image illustrates a solid mass in the right thalamus causing a mass effect and compression of the 3rd ventricle leading to obstructive hydrocephalus. A small internal enhancing focus is discernible, diagnosed as glioblastoma. D: Axial enhanced T1-weighted image demonstrated expansile mass centered in the pons (arrow) with minimal enhancement, diagnosed as diffuse midline glioma, H3K27M altered.

Fig. 6 Optic pathway glioma. A: Axial fluid-attenuated inversion recovery enhanced image displays tortuous thickening of the intraorbital segment of the left optic nerve (arrow) in a neurofibromatosis type 1 patient, suggestive of an optic pathway glioma. B: Enhanced axial T1-weighted image shows diffuse enhancement of the enlarged left optic nerve (arrow). C: Follow-up MRI without treatment shows mildly reduced thickening of the left optic nerve and the disappearance of enhancement (arrow).
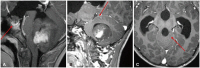
Fig. 7 Enhanced 3D T1-weighted imaging in brain tumors. A: Enhanced 3D sagittal T1-weighted image shows a large posterior fossa mass with some enhancing components. Another enhancing mass in the suprasellar cistern (arrow) is noted due to cerebrospinal fluid dissemination. B: Enhanced 3D sagittal T1-weighted image in a medulloblastoma show a small enhancing nodule (arrow) in superior cerebellum. C: The presence of a small enhancing nodule (arrow) on the enhanced 3D axial T1-weighted image corresponding to the nodule depicted on sagittal image confirms leptomeningeal seeding.

Fig. 8 Utility of post-contrast 3D fluid-attenuated inversion recovery (FLAIR). A: Enhanced axial 3D T1 image displays a posterior fossa mass with central enhancement. B: Enhanced axial 3D FLAIR image offers a better depiction of the large posterior fossa mass with multiple tiny FLAIR-enhancing nodules along the cerebellar folia. C: Enhanced axial T1 image of a patient post-ependymoma resection does not show discrete enhancing lesions in the surgical bed. D: Enhanced axial 3D FLAIR image better demonstrates FLAIR hyperintense nodules (arrows), suggesting tumor recurrence.

Fig. 9 Susceptibility-weighted imaging (SWI) in medulloblastoma. A: Axial T2-weighted image shows a well-defined mass in the 4th ventricle with multiple internal T2 hypointense foci. B: Axial SWI image shows multiple susceptibility foci corresponding to the T2 hypointense foci. C: Axial phase image shows several hyperintense foci, suggesting calcifications rather than hemorrhages. D: Axial non-enhanced CT images display multiple hyperdense foci, indicating calcifications within the 4th ventricle mass.
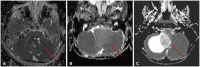
Fig. 10 Diffusion-weighted imaging in brain tumors. A: Axial apparent diffusion coefficient (ADC) image shows a reduced ADC value in medulloblastoma (arrow). B: Axial ADC image presents an intermediate ADC value in the posterior fossa ependymoma (arrow). C: Axial ADC image illustrates a high ADC value within the solid component of a posterior fossa cystic mass (arrow), confirmed as pilocytic astrocytoma.
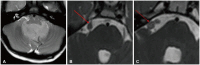
Fig. 11 Utility of 3D heavily T2-weighted sequences. A: Axial T2 preoperative image of posterior fossa ependyma shows a 4th ventricle mass extending to the bilateral foramina of Luschka. B and C: Axial heavily T2-weighted images demonstrate multiple nodular lesions along the right trigeminal nerve (arrow) and right cerebellopontine cistern (dotted arrow) which were less apparent on conventional sequences.
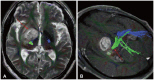
Fig. 12 Diffusion tensor imaging (DTI) in thalamic glioma. A: Axial T2 image depicts a T2 hyperintense mass in the right thalamus (arrow). B: DTI image shows the corticospinal tract (dotted arrow) traversing posteriorly to the right thalamic tumor but within a 2 cm distance.

Fig. 13 Perfusion characteristics in brain tumors. A: Enhanced axial T1-weighted image offers a view of a large cystic mass in the posterior fossa with a peripherally strong enhancing nodule (arrow), suggestive of hemangioblastoma. B: Cerebral blood volume (CBV) map from dynamic susceptibility contrast perfusion (DSC) perfusion reveals elevated relative CBV in the solid enhancing nodule (arrow). C: Enhanced axial T1-weighted image illustrates a peripheral rim-enhancing lesion in the left frontal lobe (dotted arrow) with accompanying perilesional edema in a patient who had been resected for a diffuse hemispheric glioma, H3 G34-mutant, WHO grade 4. D: CBV map from DSC perfusion shows elevated relative CBV (dotted arrow), suggesting a tumor. This was surgically confirmed as a recurrence of the diffuse hemispheric glioma, H3 G34-mutant, WHO grade 4.

Fig. 14 Magnetic resonance spectroscopy (MRS) in medulloblastoma. A: Axial T2-weighted image shows a large mass in the 4th ventricle with obstructive hydrocephalus. B: The axial apparent diffusion coefficient (ADC) map displays low ADC values, suggesting a highly cellular tumor. C: MRS reveals elevated choline (arrow), decreased NAA (dotted arrow), an elevated Cho/Cr ratio, and elevated lipid peaks. NAA, N-acetylaspartate; Cho, choline; Cr, creatine.
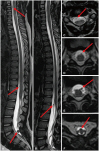
Fig. 15 3D myelographic T2-weighted imaging of the spine in ependymoma. A and B: Sagittal 3D myelographic T2-weighted images show multifocal tiny T2 hypointense seeding nodules (arrows). C-F. Reconstructed axial T2-weighted images show multifocal tiny T2 hypointense seeding nodules (arrows) corresponding to the sagittal images.
Reference
-
1. Warren KE, Vezina G, Poussaint TY, Warmuth-Metz M, Chamberlain MC, Packer RJ, et al. Response assessment in medulloblastoma and leptomeningeal seeding tumors: recommendations from the Response Assessment in Pediatric Neuro-Oncology Committee. Neuro Oncol. 2018; 20:13–23. PMID: 28449033.
Article2. Fangusaro J, Witt O, Hernáiz Driever P, Bag AK, de Blank P, Kadom N, et al. Response assessment in paediatric low-grade glioma: recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) Working Group. Lancet Oncol. 2020; 21:e305–e316. PMID: 32502457.
Article3. Erker C, Tamrazi B, Poussaint TY, Mueller S, Mata-Mbemba D, Franceschi E, et al. Response assessment in paediatric high-grade glioma: recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) Working Group. Lancet Oncol. 2020; 21:e317–e329. PMID: 32502458.
Article4. Cooney TM, Cohen KJ, Guimaraes CV, Dhall G, Leach J, Massimino M, et al. Response assessment in diffuse intrinsic pontine glioma: recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) Working Group. Lancet Oncol. 2020; 21:e330–e336. PMID: 32502459.
Article5. Lindsay HB, Massimino M, Avula S, Stivaros S, Grundy R, Metrock K, et al. Response assessment in paediatric intracranial ependymoma: recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) Working Group. Lancet Oncol. 2022; 23:e393–e401. PMID: 35901835.
Article6. Hoffman LM, Jaimes C, Mankad K, Mirsky DM, Tamrazi B, Tinkle CL, et al. Response assessment in pediatric craniopharyngioma: recommendations from the response Assessment in Pediatric Neuro-Oncology (RAPNO) Working Group. Neuro Oncol. 2023; 25:224–233. PMID: 36124689.
Article7. Jaju A, Li Y, Dahmoush H, Gottardo NG, Laughlin S, Mirsky D, et al. Imaging of pediatric brain tumors: a COG diagnostic imaging committee/SPR oncology committee/ASPNR white paper. Pediatr Blood Cancer. 2023; 70(Suppl 4):e30147. PMID: 36519599.8. Kim DY, Kim PH, Jung AY, Choi JH, Cho YA, Yoon HM, et al. Neoplastic etiology and natural course of pituitary stalk thickening. J Clin Endocrinol Metab. 2022; 107:563–574. PMID: 34614160.
Article9. Do YA, Cho SJ, Choi BS, Baik SH, Bae YJ, Sunwoo L, et al. Predictive accuracy of T2-FLAIR mismatch sign for the IDH-mutant, 1p/19q noncodeleted low-grade glioma: an updated systematic review and meta-analysis. Neurooncol Adv. 2022; 4:vdac010. PMID: 35198981.
Article10. Wagner MW, Nobre L, Namdar K, Khalvati F, Tabori U, Hawkins C, et al. T2-FLAIR mismatch sign in pediatric low-grade glioma. AJNR Am J Neuroradiol. 2023; 44:841–845. PMID: 37348970.
Article11. Farnsworth RH, Lackmann M, Achen MG, Stacker SA. Vascular remodeling in cancer. Oncogene. 2014; 33:3496–3505. PMID: 23912450.
Article12. D’Arco F, Culleton S, De Cocker LJL, Mankad K, Davila J, Tamrazi B. Current concepts in radiologic assessment of pediatric brain tumors during treatment, part 1. Pediatr Radiol. 2018; 48:1833–1843. PMID: 29980859.
Article13. Villanueva-Meyer JE, Mabray MC, Cha S. Current clinical brain tumor imaging. Neurosurgery. 2017; 81:397–415. PMID: 28486641.
Article14. Cavallaro M, Coglitore A, Tessitore A, Galletta K, Frosina L, Cuffari A, et al. Three-dimensional constructive interference in steady state (3D CISS) imaging and clinical applications in brain pathology. Biomedicines. 2022; 10:2997. PMID: 36428564.
Article15. Pollice S, Capuano M, Scarabino T. Magnetic resonance technique. Scarabino T, Pollice S, editors. Imaging gliomas after treatment: a case-based atlas. Cham: Springer;2020. p. 41–45.16. Tamrazi B, Mankad K, Nelson M, D’Arco F. Current concepts and challenges in the radiologic assessment of brain tumors in children: part 2. Pediatr Radiol. 2018; 48:1844–1860. PMID: 30215111.
Article17. Chuang MT, Liu YS, Tsai YS, Chen YC, Wang CK. Differentiating radiation-induced necrosis from recurrent brain tumor using MR perfusion and spectroscopy: a meta-analysis. PLoS One. 2016; 11:e0141438. PMID: 26741961.
Article18. Nael K, Bauer AH, Hormigo A, Lemole M, Germano IM, Puig J, et al. Multiparametric MRI for differentiation of radiation necrosis from recurrent tumor in patients with treated glioblastoma. AJR Am J Roentgenol. 2018; 210:18–23. PMID: 28952810.
Article19. Artunduaga M, Liu CA, Morin CE, Serai SD, Udayasankar U, Greer MC, et al. Safety challenges related to the use of sedation and general anesthesia in pediatric patients undergoing magnetic resonance imaging examinations. Pediatr Radiol. 2021; 51:724–735. PMID: 33860861.
Article20. Tsai JW, Choi JJ, Ouaalam H, Murillo EA, Yeo KK, Vogelzang J, et al. Integrated response analysis of pediatric low-grade gliomas during and after targeted therapy treatment. Neurooncol Adv. 2023; 5:vdac182. PMID: 36926246.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Advanced Magnetic Resonance Imaging for Pediatric Brain Tumors: Current Imaging Techniques and Interpretation Algorithms
- Current Applications and Future Perspectives of Brain Tumor Imaging
- Emerging Techniques in Brain Tumor Imaging: What Radiologists Need to Know
- Advanced MRI for Pediatric Brain Tumors with Emphasis on Clinical Benefits
- Modern Brain Tumor Imaging
