Circulation remodeling after flow diversion of an anterior communicating artery aneurysm: A case report
- Affiliations
-
- 1University of New England College of Osteopathic Medicine, Biddeford, ME, USA
- 2Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
- 3Department of Radiology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
- 4Northern Light Neurosurgery and Spine, Bangor, ME, USA
- KMID: 2546168
- DOI: http://doi.org/10.7461/jcen.2022.E2022.07.009
Abstract
- Anterior communicating artery aneurysms are the most common intracranial aneurysm and have a high risk of rupture which can lead to morbidity and mortality. Traditionally, intracranial aneurysms were treated by clipping with neurosurgical access. However, certain patients may prefer less invasive approaches or not represent open surgical candidates. Flow diverters, including flow-redirection endoluminal devices (FRED), are new-generation stents that are placed endovascularly by transfemoral or transradial access. Recent studies have demonstrated that FRED is both safe and effective, with complete occlusion of aneurysms in over 90% of patients. This case highlights an interesting phenomenon of post-flow diversion circulatory remodeling, where flow diverter treatment can alter the circle of Willis anatomy and physiology.
Keyword
Figure
-
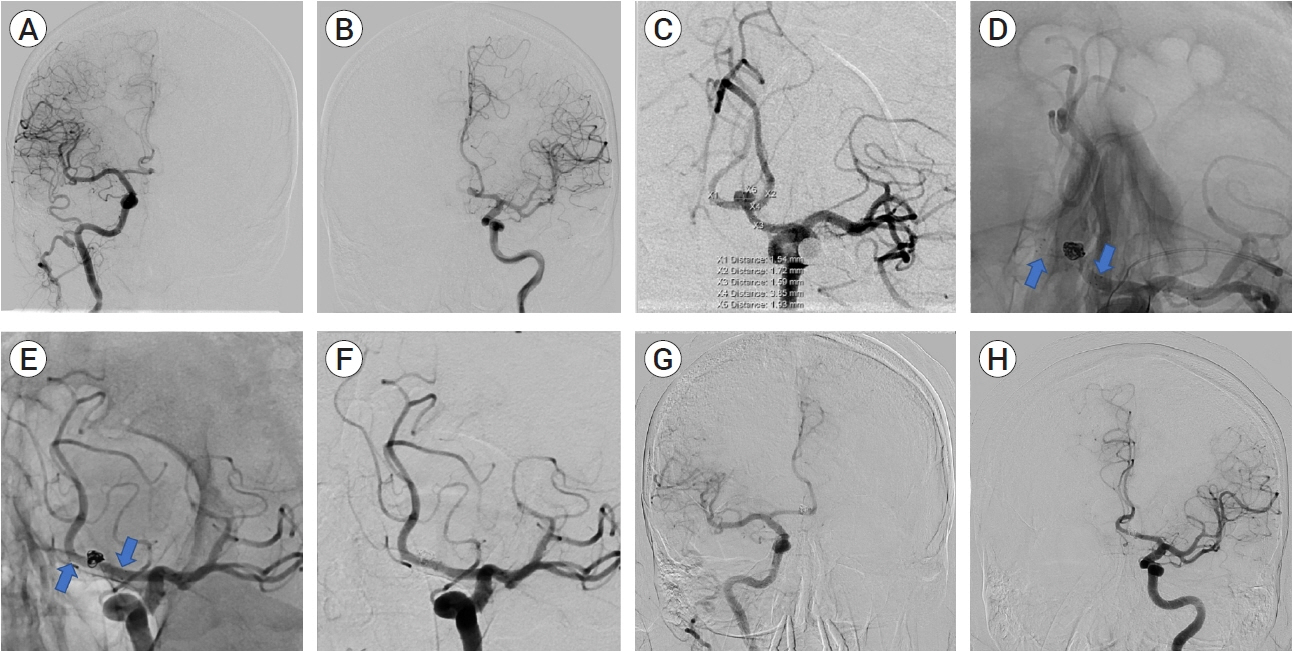
Fig. 1. (A) Anteroposterior projection of right internal cerebral artery (ICA) contrast injection. The right anterior communicating artery (ACOM) fills from the ipsilateral right ICA. (B) Anteroposterior projection of left ICA contrast injection. The left ACOM fills from the ipsilateral left ICA. (C) Oblique working projection of left ICA contrast injection. There is a 3.9×1.9 mm ACOM aneurysm. The ACOM has an “X” configuration. (D) As the arrows indicate, native working projection immediately following treatment. There is a FRED junior stent (arrows) from the left A1 segment, covering the neck of the ACOM aneurysm, and into the right A2 segment. (E) Fifteen-month follow-up native oblique working projection. There is a FRED junior stent from the left A1 segment, covering the neck of the ACOM aneurysm, and into the right A2 segment as indicated by the arrows. (F) Fifteen-month follow-up oblique working projection of left ICA contrast injection. There is no residual aneurysm filling. (G) Fifteen-month follow-up anteroposterior projection of right ICA contrast injection. The contralateral left ACOM fills from the right ICA. (H) Fifteen-month follow-up anteroposterior projection of left ICA contrast injection. The contralateral right ACOM fills from the left ICA. FRED, flow-redirection endoluminal device
Reference
-
1. Chen J, Li M, Zhu X, Chen Y, Zhang C, Shi W, et al. Anterior communicating artery aneurysms: anatomical considerations and microsurgical strategies. Front Neurol. 2020; Sep. 11:1020.2. Chua MMJ, Silveira L, Moore J, Pereira VM, Thomas AJ, Dmytriw AA. Flow diversion for treatment of intracranial aneurysms: mechanism and implications. Ann Neurol. 2019; Jun. 85(6):793–800.3. Dmytriw AA, Phan K, Moore JM, Pereira VM, Krings T, Thomas AJ. On flow diversion: the changing landscape of intracerebral aneurysm management. AJNR Am J Neuroradiol. 2019; Apr. 40(4):591–600.4. Griessenauer CJ, Enriquez-Marulanda A, Xiang S, Hong T, Zhang H, Taussky P, et al. Comparison of PED and FRED flow diverters for posterior circulation aneurysms: a propensity score matched cohort study. J Neurointerv Surg. 2021; Feb. 13(2):153–8.5. Hernesniemi J, Dashti R, Lehecka M, Niemelä M, Rinne J, Lehto H, et al. Microneurosurgical management of anterior communicating artery aneurysms. Surg Neurol. 2008; Jul. 70(1):8–28. discussion 29.6. Liu P, Lv X, Li Y, Lv M. High resolution MRI in treatment decision of anterior communicating artery aneurysm accompanied by visual symptoms: endovascular treatment or surgical clipping? A report of two cases and literature review. Interv Neuroradiol. 2016; Jun. 22(3):270–7.7. Luecking H, Doerfler A, Goelitz P, Hoelter P, Engelhorn T, Lang S. Two- to five-year follow-up of 78 patients after treatment with the Flow Redirection Endoluminal Device. Interv Neuroradiol. 2020; Feb. 26(1):38–44.8. Maragkos GA, Dmytriw AA, Salem MM, Tutino VM, Meng H, Cognard C, et al. Overview of different flow diverters and flow dynamics. Neurosurgery. 2020; Jan. 86(Suppl 1):S21–34.9. Nariai Y, Takigawa T, Hyodo A, Suzuki K. Distal migration of the flow-redirection endoluminal device immediately after treatment: a case report and literature review. Surg Neurol Int. 2022; Mar. 13:81.10. Xie Y, Tian H, Xiang B, Li D, Liu YZ, Xiang H. Risk factors for anterior communicating artery aneurysm rupture: a protocol for systematic review and meta-analysis. Medicine (Baltimore). 2021; Dec. 100(48):e28088.11. Xu N, Meng H, Liu T, Feng Y, Qi Y, Zhang D, et al. Stent-jailing technique reduces aneurysm recurrence more than stent-jack technique by causing less mechanical forces and angiogenesis and inhibiting TGF-β/Smad2,3,4 signaling pathway in intracranial aneurysm patients. Front Physiol. 2019; Jan. 9:1862.12. Zhang J, Can A, Lai PMR, Mukundan S Jr, Castro VM, Dligach D, et al. Vascular geometry associated with anterior communicating artery aneurysm formation. World Neurosurg. 2021; Feb. 146:e1318–25.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Analysis of the Pattern of Anterior-Posterior Circulation in Patients with Posterior Communicating Artery Aneurysm
- Intracranial Aneurysm Associated with Aplasia of the Internal Cartoid Artery
- Microsurgical anatomy of the Anterior Cerebral-anterior Communicating Artery
- Transposition of Anterior Choroidal Artery and Posterior Communicating Artery Origin
- Anterior Communicating Artery Aneurysms Associated with Multiplication of Anterior Communicating Artery
