Case Report of Erdheim-Chester Disease Successfully Treated with Pegylated Interferon: A Single-Center Experience
- Affiliations
-
- 1Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 4Division of Cardiology, Department of Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2544185
- DOI: http://doi.org/10.4143/crt.2022.1535
Abstract
- Erdheim-Chester disease (ECD), also known as non-Langerhans cell histiocytosis, is a multi-systemic disease with unclear pathogenesis. Based on a small number of case studies, pegylated interferon-α (PEG-IFN-α) has been used as the front-line treatment option. However, there are limited data regarding administration of ropegylated-interferon α-2b (ROPEG-IFN-α 2b) for ECD patients. Herein, we report two cases of severe ECD treated with two types of PEG-IFN-α. One patient with heart and skeleton involvement and BRAF V600E mutation was treated with weekly PEG-IFN-α 2a. Another patient with bone involvement and no BRAF V600E mutation was administered monthly ROPEG-IFN-α 2b. The two types of PEG-IFN-α showed excellent disease control, excellent survival outcomes, and manageable toxicities in ECD patients. These results suggest that ROPEG-IFN-α 2b could be used equivalently to PEG-IFN-α 2a for management of advanced ECD.
Keyword
Figure
-
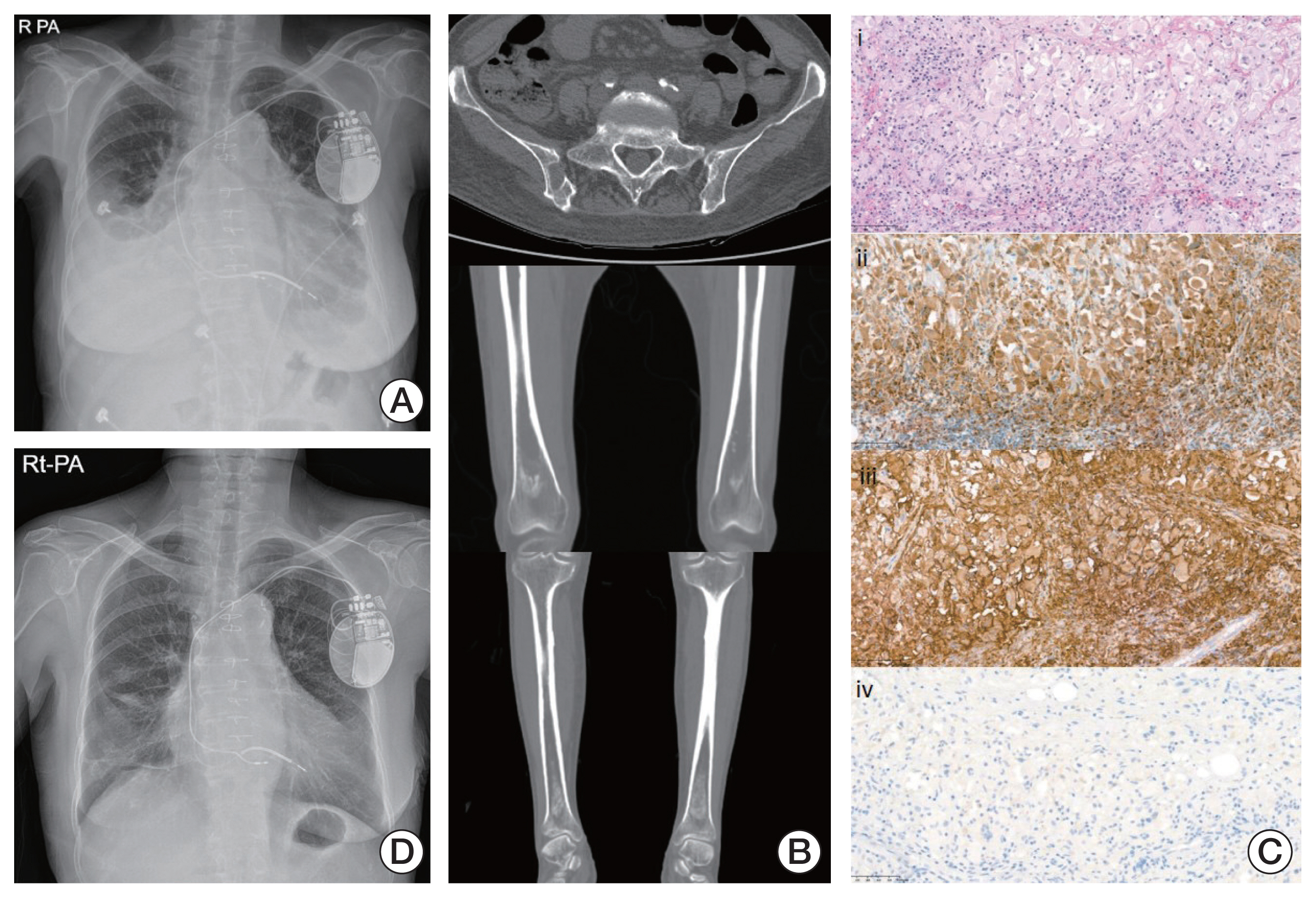
Fig. 1 (A) Chest X-ray at diagnosis shows bilateral pleural effusion and pulmonary edema. (B) Skeletal computed tomography shows osteolytic lesion at right ilium and bilateral symmetric osteosclerosis of both distal femurs and proximal and distal tibia. (C) Heart biopsy presented proliferation of foamy histiocytes (H&E stain, ×100) (i), positive immunostaining of CD68 (x100) (ii) and CD163 (x100) (iii), but negative immunostaining of CD1a (x100) (iv). (D) The pleural effusion had resolved in the chest X-ray after 3 months of pegylated interferon-α 2a injections.

Fig. 2 (A) Baseline positron emission tomography shows multiple hypermetabolic bone lesions and lymphadenopathy. (B) Bone marrow biopsy reveals numerous histiocytic infiltration (H&E stain, ×200) (i), CD68-positive staining (×200) (ii), CD163-positive staining (×200) (iii) and CD1a-negative staining (×200) (iv). (C) After ropegylated-interferon α-2b, the disease nearly resolved in follow-up positron emission tomography.
Reference
-
References
1. Arnaud L, Hervier B, Neel A, Hamidou MA, Kahn JE, Wechsler B, et al. CNS involvement and treatment with interferon-alpha are independent prognostic factors in Erdheim-Chester disease: a multicenter survival analysis of 53 patients. Blood. 2011; 117:2778–82.2. Munoz J, Janku F, Cohen PR, Kurzrock R. Erdheim-Chester disease: characteristics and management. Mayo Clin Proc. 2014; 89:985–96.
Article3. Vassallo R, Ryu JH, Schroeder DR, Decker PA, Limper AH. Clinical outcomes of pulmonary Langerhans’-cell histiocytosis in adults. N Engl J Med. 2002; 346:484–90.
Article4. Haroche J, Charlotte F, Arnaud L, von Deimling A, Helias-Rodzewicz Z, Hervier B, et al. High prevalence of BRAF V600E mutations in Erdheim-Chester disease but not in other non-Langerhans cell histiocytoses. Blood. 2012; 120:2700–3.
Article5. Diamond EL, Dagna L, Hyman DM, Cavalli G, Janku F, Estrada-Veras J, et al. Consensus guidelines for the diagnosis and clinical management of Erdheim-Chester disease. Blood. 2014; 124:483–92.
Article6. Arnaud L, Gorochov G, Charlotte F, Lvovschi V, Parizot C, Larsen M, et al. Systemic perturbation of cytokine and chemokine networks in Erdheim-Chester disease: a single-center series of 37 patients. Blood. 2011; 117:2783–90.
Article7. Dagna L, Corti A, Langheim S, Guglielmi B, De Cobelli F, Doglioni C, et al. Tumor necrosis factor alpha as a master regulator of inflammation in Erdheim-Chester disease: rationale for the treatment of patients with infliximab. J Clin Oncol. 2012; 30:e286–90.8. Stoppacciaro A, Ferrarini M, Salmaggi C, Colarossi C, Praderio L, Tresoldi M, et al. Immunohistochemical evidence of a cytokine and chemokine network in three patients with Erdheim-Chester disease: implications for pathogenesis. Arthritis Rheum. 2006; 54:4018–22.
Article9. Mossetti G, Rendina D, Numis FG, Somma P, Postiglione L, Nunziata V. Biochemical markers of bone turnover, serum levels of interleukin-6/interleukin-6 soluble receptor and bisphosphonate treatment in Erdheim-Chester disease. Clin Exp Rheumatol. 2003; 21:232–6.10. Braiteh F, Boxrud C, Esmaeli B, Kurzrock R. Successful treatment of Erdheim-Chester disease, a non-Langerhans-cell histiocytosis, with interferon-alpha. Blood. 2005; 106:2992–4.11. Gisslinger H, Klade C, Georgiev P, Krochmalczyk D, Gercheva-Kyuchukova L, Egyed M, et al. Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study. Lancet Haematol. 2020; 7:e196–208.12. Haroche J, Amoura Z, Trad SG, Wechsler B, Cluzel P, Grenier PA, et al. Variability in the efficacy of interferon-alpha in Erdheim-Chester disease by patient and site of involvement: results in eight patients. Arthritis Rheum. 2006; 54:3330–6.
Article13. Hervier B, Arnaud L, Charlotte F, Wechsler B, Piette JC, Amoura Z, et al. Treatment of Erdheim-Chester disease with long-term high-dose interferon-alpha. Semin Arthritis Rheum. 2012; 41:907–13.14. Goyal G, Shah MV, Call TG, Litzow MR, Hogan WJ, Go RS. Clinical and radiologic responses to cladribine for the treatment of Erdheim-Chester disease. JAMA Oncol. 2017; 3:1253–6.
Article15. Mazor RD, Manevich-Mazor M, Shoenfeld Y. Erdheim-Chester Disease: a comprehensive review of the literature. Orphanet J Rare Dis. 2013; 8:137.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erdheim-Chester Disease with Perirenal Masses Containing Macroscopic Fat Tissue
- Improvement of Erdheim-Chester disease-related renal failure after treatment with anakinra
- Successful Treatment of Erdheim-Chester Disease with Multisystemic Involvement in a 4-year-old Child by Interferon-α and Corticosteroid
- Commentary on "A Case of Erdheim-Chester Disease with Asymptomatic Renal Involvement"
- A Case of Erdheim-Chester Disease with Bilateral Hydronephrosis
