Primary adenocarcinoma with yolk sac differentiation in the transplant ureter and salvage of the transplant kidney: a rare case report
- Affiliations
-
- 1Department of Urology, Command Hospital (Southern Command), Pune, India
- 2Department of Pathology, Command Hospital (Southern Command), Pune, India
- 3Department of Nephrology, Command Hospital (Southern Command), Pune, India
- 4Department of General Surgery, Military Hospital, Kargil, India
- KMID: 2544116
- DOI: http://doi.org/10.4285/kjt.22.0055
Abstract
- Renal transplant recipients are prone to a high risk of subsequent upper tract urothelial carcinoma, occurring in both native and transplant ureters. We report a rare case of adenocarcinoma with yolk sac differentiation of the transplant ureter, which was managed successfully with transplant ureterectomy and pyelovesicostomy, thereby salvaging the functioning transplant kidney.
Keyword
Figure
-

Fig. 1 Noncontrast computed tomography of the kidneys, ureters, and bladder scan showing hydronephrosis of the transplant kidney with the intrarenal pelvis and a lesion in the proximal part of the graft ureter, just below the ureteropelvic junction (red arrow).
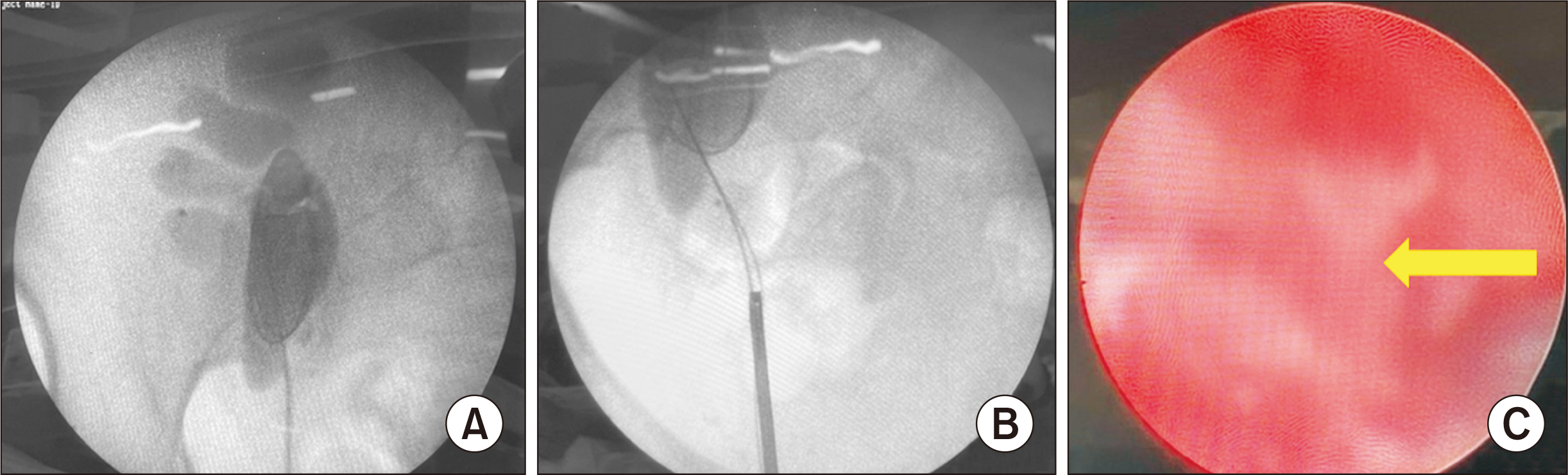
Fig. 2 (A) Retrograde pyelography showing hydronephrosis of the transplant kidney with a cut-off of contrast just below the ureteropelvic junction. (B) The ureteroscope was not able to negotiate beyond the site of obstruction, and (C) ureteroscopy showing unhealthy tissue (yellow arrow).
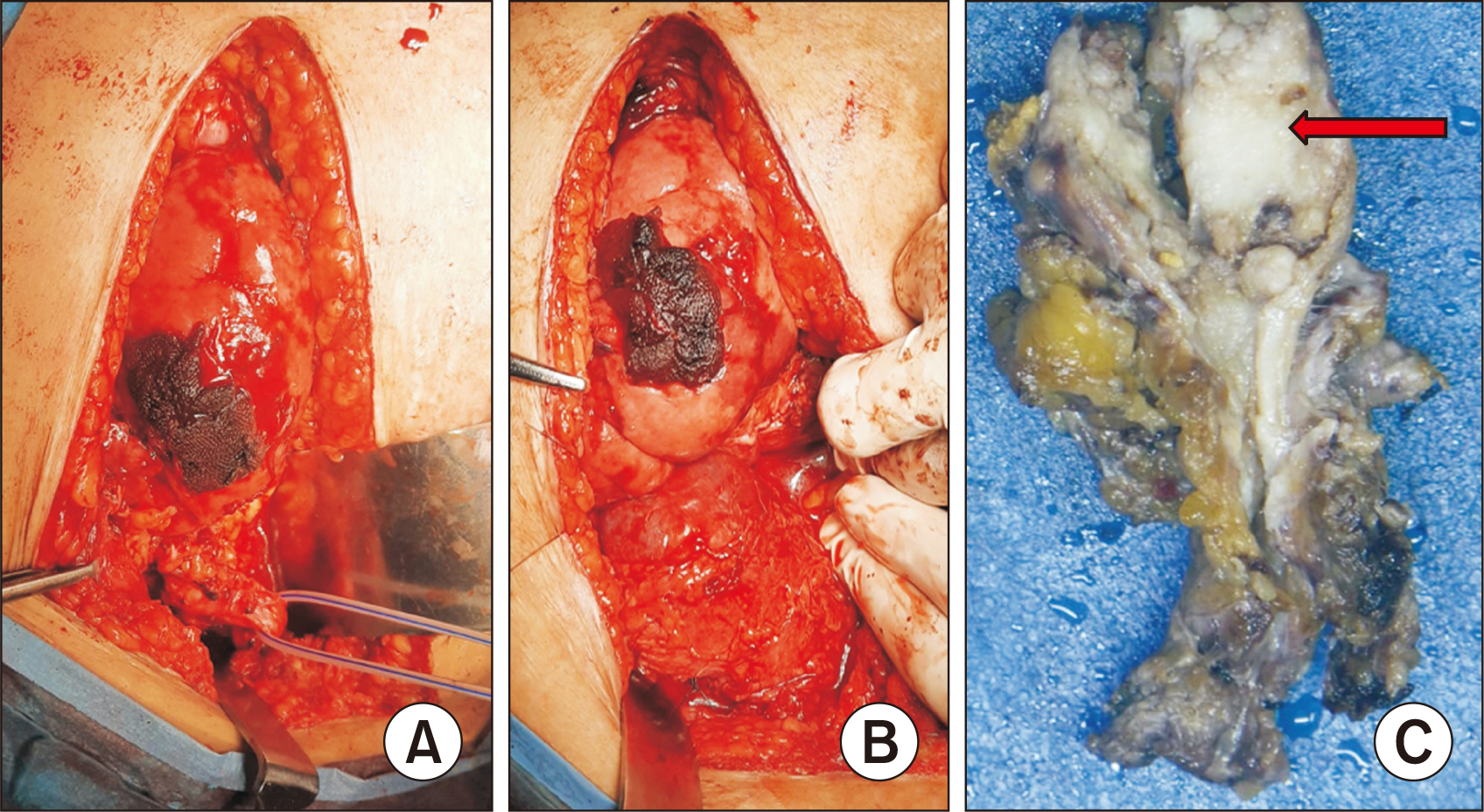
Fig. 3 Intraoperative images showing (A) dissection of the transplant ureter, (B) completed pyelovesicostomy with the bladder distended with saline to check for urine leak at the anastomosis, and (C) gross photograph of the cut-open resected specimen of ureterectomy with a whitish, firm infiltrative tumor present at the proximal end (red arrow).

Fig. 4 H&E stained histopathological images of the tumor: (A) tumor composed of areas of villoglandular morphology infiltrating the underlying stroma along with areas of necrosis (black arrow; H&E, ×40), (B) another area of the ureteric tumor with the lining showing a well-defined villoglandular architecture (H&E, ×40), (C) tumor with areas showing a reticulocystic pattern, some of the cystic areas containing secretions within (H&E, ×40), and (D) higher-power view of another area with glandular differentiation, showing distorted glands lined by highly pleomorphic cells (H&E, ×100).

Fig. 5 Immunohistochemistry characterizing the lesion as a ureteric adenocarcinoma with a villoglandular pattern and areas of yolk sac differentiation: (A) tumor cells are diffusely positive for CK7 (×100), (B) GATA 3 (×100), and (C) CA 19.9 (×100). (D) The reticulocystic areas were positive for alpha-fetoprotein (×200) and (E) glypican 3 (×200). (F) The tumor had a mutated phenotype for p53 (×100).

Fig. 6 Postoperative magnetic resonance imaging of the abdomen, 12 months after total transplant ureterectomy and pyelovesicostomy, showing a patent anastomosis between the transplanted renal pelvis and the superolateral wall of the bladder, with no lesion in the renal pelvis or bladder and significant improvement of hydronephrosis.
Reference
-
1. Yu J, Lee CU, Kang M, Jeon HG, Jeong BC, Seo SI, et al. 2018; Incidences and oncological outcomes of urothelial carcinoma in kidney transplant recipients. Cancer Manag Res. 11:157–66. DOI: 10.2147/CMAR.S185796. PMID: 30636892. PMCID: PMC6307682.
Article2. Olsburgh J, Zakri RH, Horsfield C, Collins R, Fairweather J, O'Donnell P, et al. 2016; TCC in transplant ureter: when and when not to preserve the transplant kidney. Am J Transplant. 16:704–11. DOI: 10.1111/ajt.13533. PMID: 26731492.3. Sagnotta A, Dente M, Socciarelli F, Cacchi C, Stoppacciaro A, Balducci G. 2014; Primary adenocarcinoma of the renal pelvis: histologic features of a stepwise process from intestinal hyperplasia to dysplasia in a patient with chronic renal abscess. Int J Surg Pathol. 22:182–5. DOI: 10.1177/1066896913502225. PMID: 24008439.4. Hudson J, Arnason T, Merrimen JL, Lawen J. 2013; Intestinal type villous adenoma of the renal pelvis. Can Urol Assoc J. 7:E138–42. DOI: 10.5489/cuaj.257. PMID: 23671505. PMCID: PMC3650791.
Article5. Gullo CE, Fantin JP, Spessoto LC, Gatti M, Arruda JG, Antoniassi TD, et al. 2017; Renal cell carcinoma and mucinous adenocarcinoma of ureter after renal transplantation with neoplasm of urethra in follow up. Int J Sci. 6:77–80. DOI: 10.18483/ijSci.1202.6. Healy KA, Carney KJ, Osunkoya AO. 2010; Endometrioid adenocarcinoma in the native ureter of a renal transplant patient: case report and review of the literature. ScientificWorldJournal. 10:1714–22. DOI: 10.1100/tsw.2010.166. PMID: 20842317. PMCID: PMC5763830.
Article7. Chaudhary P, Agarwal R, Srinivasan S, Singh D. 2016; Primary adenocarcinoma of ureter: a rare histopathological variant. Urol Ann. 8:357–9. DOI: 10.4103/0974-7796.184885. PMID: 27453661. PMCID: PMC4944632.
Article8. Espejo-Herrera N, Condom-Mundó E. 2020; Yolk sac tumor differentiation in urothelial carcinoma of the urinary bladder: a case report and differential diagnosis. Diagn Pathol. 15:68. DOI: 10.1186/s13000-020-00983-3. PMID: 32493368. PMCID: PMC7271425.
Article9. Collins K, Alkashash AM, Hwang M, Kaimakliotis HZ, Cheng L, Idrees MT. 2022; Somatic-type yolk sac tumor arising as a predominant component of bladder urothelial carcinoma. Int J Surg Pathol. 30:207–13. DOI: 10.1177/10668969211030688. PMID: 34255554.
Article10. Bihari C, Rastogi A, Chandan KN, Yadav V, Panda D. 2013; Gastric adenocarcinoma with yolk sac tumor differentiation and liver metastasis of yolk sac tumor component. Case Rep Oncol Med. 2013:923596. DOI: 10.1155/2013/923596. PMID: 24294529. PMCID: PMC3835910.
Article11. Umeda H, Kikuchi S, Kuroda S, Yano S, Tanaka T, Noma K, et al. 2021; Long-term survival without recurrence after surgery for gastric yolk sac tumor-like carcinoma: a case report. Surg Case Rep. 7:111. DOI: 10.1186/s40792-021-01199-3. PMID: 33956241. PMCID: PMC8102656.
Article12. Ji M, Lu Y, Guo L, Feng F, Wan X, Xiang Y. 2013; Endometrial carcinoma with yolk sac tumor-like differentiation and elevated serum β-hCG: a case report and literature review. Onco Targets Ther. 6:1515–22. DOI: 10.2147/OTT.S51983. PMID: 24187502. PMCID: PMC3810345.13. Sookram J, Levin B, Barroeta J, Kenley K, Mehta P, Krill LS. 2019; A case of ovarian endometrioid adenocarcinoma with yolk sac differentiation and Lynch syndrome. Gynecol Oncol Rep. 27:60–4. DOI: 10.1016/j.gore.2019.01.001. PMID: 30723761. PMCID: PMC6348978.
Article14. Gutierrez-Dalmau A, Campistol JM. 2007; Immunosuppressive therapy and malignancy in organ transplant recipients: a systematic review. Drugs. 67:1167–98. DOI: 10.2165/00003495-200767080-00006. PMID: 17521218.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Yolk Sac Tumor of the Cerebellar Hemisphere: Case Report
- A case of Primary Mediastinal Yolk Sac Tumor
- Yolk-sac Tumor of Testis in Male Infant with Pulmonary Metastasis: A Case Report
- Adenocarcinoma with Yolk Sac Tumor of the Stomach: Case Report with Review of the Literature and an Immunohistochemical Study
- A Case of Systemic Chemotherapy in Advanced Yolk Sac Carcinoma
