Inspiratory Muscle Training in Patients in the Postoperative Phase of Cardiac Surgery: A Systematic Review and Meta-Analysis
- Affiliations
-
- 1Department of Medicine and Human Health, Bahiana School of Medicine and Public Health, Salvador, Brazil
- 2Department of Physical Therapy, Centro Universitário Nobre, Feira de Santana, Brazil
- 3Physiotherapy Department, Hospital Geral Clériston Andrade, Feira de Santana, Brazil
- 4Department of Physical Therapy, Universidade Federal da Bahia, Salvador, Brazil
- KMID: 2543413
- DOI: http://doi.org/10.5535/arm.23022
Abstract
- To review the evidence about inspiratory muscle training (IMT) in patients in postoperative of cardiac surgery. We conducted this systematic review used the databases Ovid, LILACS, CINAHL, PubMed, PEDro, and CENTRAL. Randomized clinical trials that addressed IMT after cardiac surgery were selected. The outcomes assessed were maximum inspiratory pressure (MIP), maximum expiratory pressure (MEP), tidal volume (TV), peak expiratory flow (PEF), functional capacity (6-minute walk test) and length of hospital stay. The mean difference between groups and the respective 95% confidence interval (CI) were calculated and used to quantify the effect of continuous outcomes. Seven studies were selected. The IMT was superior to the control over MIP 15.77 cmH2O (95% CI, 5.95–25.49), MEP 15.87 cmH2O (95% CI, 1.16–30.58), PEF 40.98 L/min (95% CI, 4.64–77.32), TV 184.75 mL (95% CI, 19.72–349.77), hospital stay -1.25 days (95% CI, -1.77 to -0.72), but without impact on functional capacity 29.93 m (95% CI, -27.59 to 87.45). Based on the results presented, IMT was beneficial as a form of treatment for patients after cardiac surgery.
Figure
-

Fig. 1. Selection process for studies included in the analysis.
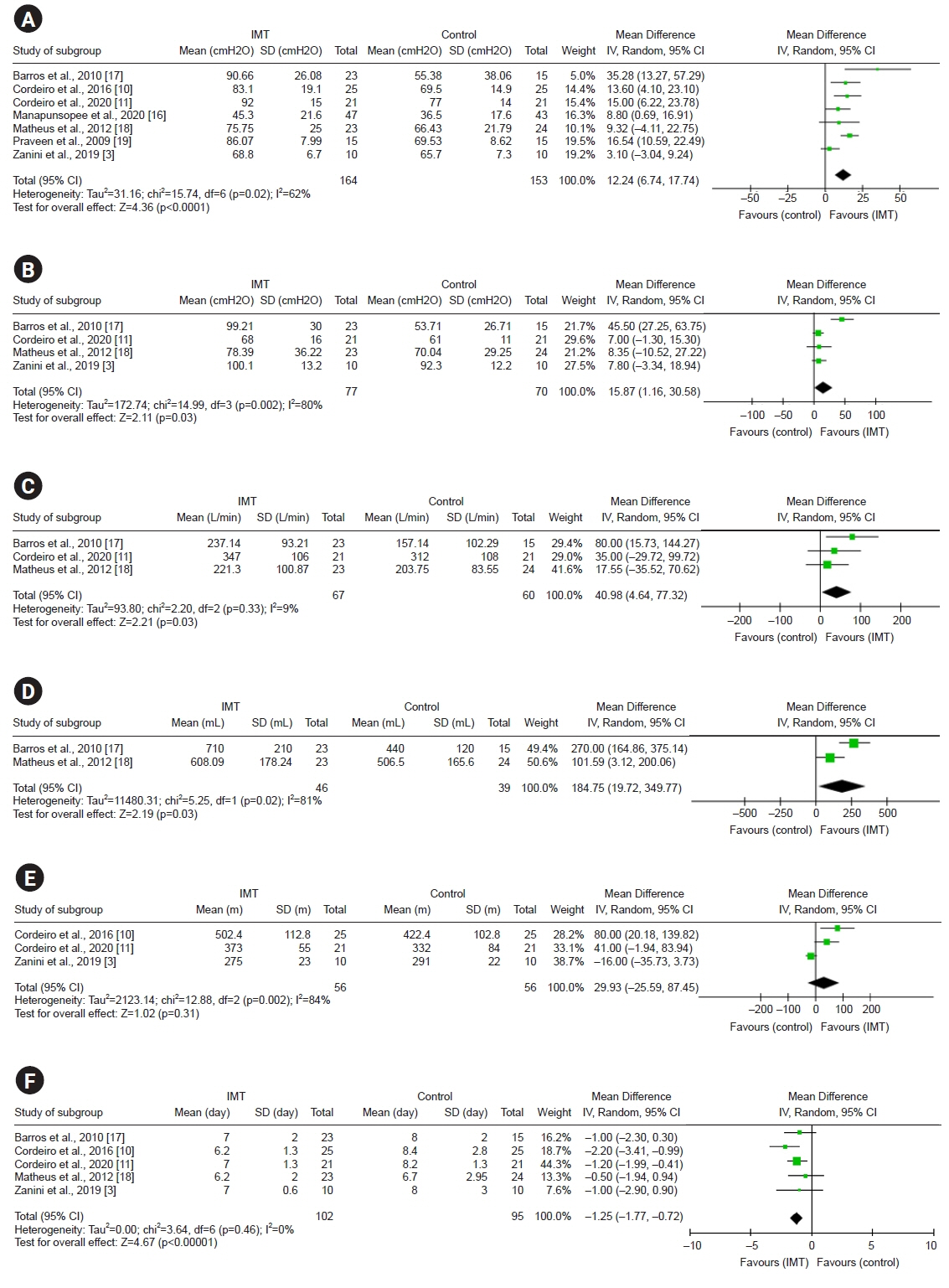
Fig. 2. Forest plot of the results of the meta-analysis. (A) Comparison of the inspiratory muscle training (IMT) with the control over the maximum inspiratory pressure outcome. The values presented are the average effects (difference between the means) and a 95% confidence interval (CI). The average effect was calculated using a random-effect model. (B) Comparison of the IMT with the control over the maximum expiratory pressure outcome. The values presented are the average effects (difference between the means) and a 95% CI. The average effect was calculated using a random-effect model. (C) Comparison of IMT with control over peak expiratory flow outcome. The values presented are the average effects (difference between the means) and a 95% CI. The average effect was calculated using a random-effect model. (D) Comparison of the IMT with the control over the tidal volume outcome. The values presented are the average effects (difference between the means) and a 95% CI. The average effect was calculated using a random-effect model. (E) Comparison of the IMT with the control over the functional capacity outcome. The values presented are the average effects (difference between the means) and a 95% CI. The average effect was calculated using a random-effect model. (F) Comparison of the IMT with the control over the outcome length of hospital stay. The values presented are the average effects (difference between the means) and a 95% CI. The average effect was calculated using a random-effect model. SD, standard deviation.
Reference
-
1. Gjeilo KH, Stenseth R, Wahba A, Lydersen S, Klepstad P. Long-term health-related quality of life and survival after cardiac surgery: a prospective study. J Thorac Cardiovasc Surg. 2018; 156:2183–90.e2.
Article2. Johnson D, Hurst T, Thomson D, Mycyk T, Burbridge B, To T, et al. Respiratory function after cardiac surgery. J Cardiothorac Vasc Anesth. 1996; 10:571–7.
Article3. Zanini M, Nery RM, de Lima JB, Buhler RP, da Silveira AD, Stein R. Effects of different rehabilitation protocols in inpatient cardiac rehabilitation after coronary artery bypass graft surgery: a randomized clinical trial. J Cardiopulm Rehabil Prev. 2019; 39:E19–25.4. Gomes Neto M, Martinez BP, Reis HF, Carvalho VO. Pre- and postoperative inspiratory muscle training in patients undergoing cardiac surgery: systematic review and meta-analysis. Clin Rehabil. 2017; 31:454–64.
Article5. Welsby IJ, Bennett-Guerrero E, Atwell D, White WD, Newman MF, Smith PK, et al. The association of complication type with mortality and prolonged stay after cardiac surgery with cardiopulmonary bypass. Anesth Analg. 2002; 94:1072–8.
Article6. Katsura M, Kuriyama A, Takeshima T, Fukuhara S, Furukawa TA. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. 2015; 2015:CD010356.
Article7. Kendall F, Oliveira J, Peleteiro B, Pinho P, Bastos PT. Inspiratory muscle training is effective to reduce postoperative pulmonary complications and length of hospital stay: a systematic review and meta-analysis. Disabil Rehabil. 2018; 40:864–82.
Article8. Thybo Karanfil EO, Møller AM. Preoperative inspiratory muscle training prevents pulmonary complications after cardiac surgery - a systematic review. Dan Med J. 2018; 65:A5450.9. Chen X, Hou L, Zhang Y, Liu X, Shao B, Yuan B, et al. The effects of five days of intensive preoperative inspiratory muscle training on postoperative complications and outcome in patients having cardiac surgery: a randomized controlled trial. Clin Rehabil. 2019; 33:913–22.
Article10. Cordeiro AL, de Melo TA, Neves D, Luna J, Esquivel MS, Guimarães AR, et al. Inspiratory muscle training and functional capacity in patients undergoing cardiac surgery. Braz J Cardiovasc Surg. 2016; 31:140–4.11. Cordeiro ALL, Mascarenhas HC, Landerson L, Araújo JDS, Borges DL, Melo TA, et al. Inspiratory muscle training based on anaerobic threshold on the functional capacity of patients after coronary artery bypass grafting: clinical trial. Braz J Cardiovasc Surg. 2020; 35:942–9.
Article12. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 6:e1000097.
Article13. da Costa Santos CM, de Mattos Pimenta CA, Nobre MR. The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem. 2007; 15:508–11.
Article14. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003; 83:713–21.
Article15. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 5.1 (updated March 2011) [Internet]. London: Cochrane, 2011. [cited 2020 Dec 5]. Available from: www.training.cochrane.org/handbook.16. Manapunsopee S, Thanakiatpinyo T, Wongkornrat W, Chuaychoo B, Thirapatarapong W. Effectiveness of incentive spirometry on inspiratory muscle strength after coronary artery bypass graft surgery. Heart Lung Circ. 2020; 29:1180–6.
Article17. Barros GF, Santos Cda S, Granado FB, Costa PT, Límaco RP, Gardenghi G. Respiratory muscle training in patients submitted to coronary arterial bypass graft. Rev Bras Cir Cardiovasc. 2010; 25:483–90.18. Matheus GB, Dragosavac D, Trevisan P, Costa CE, Lopes MM, Ribeiro GC. Inspiratory muscle training improves tidal volume and vital capacity after CABG surgery. Rev Bras Cir Cardiovasc. 2012; 27:362–9.19. Praveen R, Swaminathan N, Praveen JS. Inspiratory muscle training is effective in improving respiratory muscle functions in patients who have undergone coronary artery bypass graft. Fizjoterapia Polska. 2009; 4:285–92.20. Kodric M, Trevisan R, Torregiani C, Cifaldi R, Longo C, Cantarutti F, et al. Inspiratory muscle training for diaphragm dysfunction after cardiac surgery. J Thorac Cardiovasc Surg. 2013; 145:819–23.
Article21. Brocki BC, Andreasen JJ, Langer D, Souza DS, Westerdahl E. Postoperative inspiratory muscle training in addition to breathing exercises and early mobilization improves oxygenation in high-risk patients after lung cancer surgery: a randomized controlled trial. Eur J Cardiothorac Surg. 2016; 49:1483–91.
Article22. Ge X, Wang W, Hou L, Yang K, Fa X. Inspiratory muscle training is associated with decreased postoperative pulmonary complications: evidence from randomized trials. J Thorac Cardiovasc Surg. 2018; 156:1290–300.e5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effectiveness of Inspiratory Muscle Training on Respiratory Muscle Strength in Patients Undergoing Cardiac Surgeries: A Systematic Review With Meta-Analysis
- Factors Related to Persistent Postoperative Pain after Cardiac Surgery: A Systematic Review and Meta-Analysis
- An Introduction of the Systematic Review and Meta-Analysis
- Effect of Autogenic Training for Stress Response: A Systematic Review and Meta-Analysis
- Clinical Implications of Inspiratory Muscle Training in Patients with Duchenne Muscular Dystrophy
