Histological analysis on tissues around orthodontically intruded maxillary molars using temporary anchorage devices: A case report
- Affiliations
-
- 1Division of Orthodontics, Department of Dentistry, National Taiwan University Hospital, Taipei, Taiwan
- 2Department of Periodontology, School of Dentistry, College of Medicine, National Taiwan University, Taipei, Taiwan
- 3Private Practice, New Taipei City, Taiwan
- 4Division of Oral Pathology and Diagnosis, Department of Dentistry, National Taiwan University Hospital, Taipei, Taiwan
- 5Department of Oral Pathology and Oral Diagnosis, School of Dentistry, College of Medicine, National Taiwan University, Taipei, Taiwan
- 6Graduate Institute of Clinical Dentistry, School of Dentistry, College of Medicine, National Taiwan University, Taipei, Taiwan
- 7Division of Orthodontics and Dentofacial Orthopedics, Department of Dentistry, National Taiwan University Hospital, Taipei, Taiwan
- KMID: 2540952
- DOI: http://doi.org/10.4041/kjod22.150
Abstract
- Before progress was recently made in the application of temporary anchorage devices (TADs) in bio-mechanical design, orthodontists were rarely able to intrude molars to reduce upper posterior dental height (UPDH). However, TADs are now widely used to intrude molars to flatten the occlusal plane or induce counterclockwise rotation of the mandible. Previous studies involving clinical or animal histological evaluation on changes in periodontal conditions after molar intrusion have been reported, however, studies involving human histology are scarce. This case was a Class I malocclusion with a high mandibular plane angle. Upper molar intrusion with TADs was performed to reduce UPDH, which led to counterclockwise rotation of the mandible. After 5 months of upper molar intrusion, shortened clinical crowns were noticed, which caused difficulties in oral hygiene and hindered orthodontic tooth movement. The mid-treatment cone-beam computed tomography revealed redundant bone physically interfering with buccal attachment and osseous resective surgeries were followed. During the surgeries, bilateral mini screws were removed and bulging alveolar bone and gingiva were harvested for biopsy. Histological examination revealed bacterial colonies at the bottom of the sulcus. Infiltration of chronic inflammatory cells underneath the non-keratinized sulcular epithelium was noted, with abundant capillaries being filled with red blood cells. Proximal alveolar bone facing the bottom of the gingival sulcus exhibited active bone remodeling and woven bone formation with plump osteocytes in the lacunae. On the other hand, buccal alveolar bone exhibited lamination, indicating slow bone turnover in the lateral region.
Figure
-

Figure 1 Pre-treatment facial and intra-oral photographs. Patient showing lip incompetence, gummy smile and dentoalvolar protrusion.
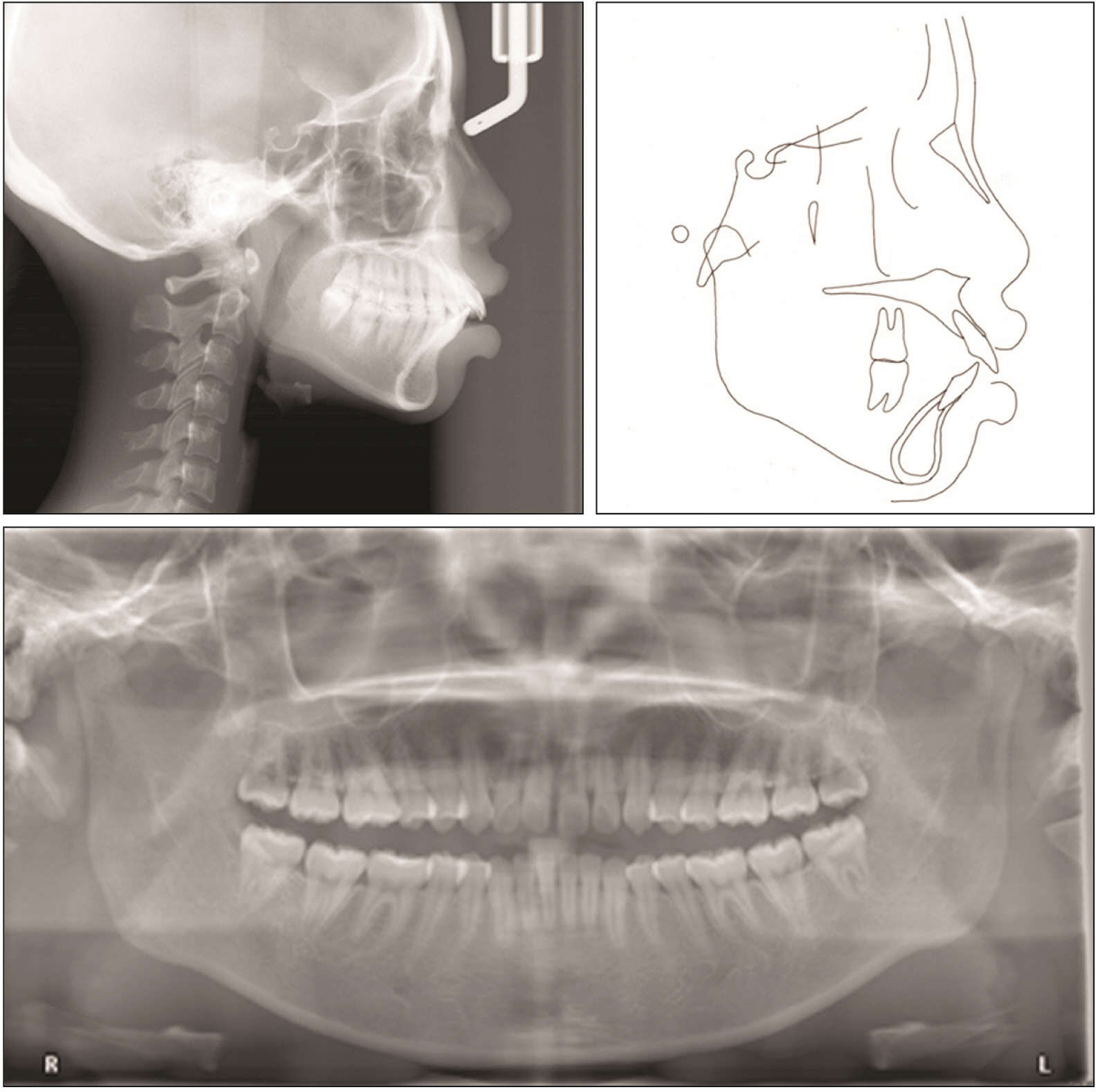
Figure 2 Pre-treatment lateral cephalogram, cephalogram tracing, and panoramic radiograph. Proclination of upper and lower anterior teeth was prominent.

Figure 3 Intra-oral photographs at 1 year and 5 months of treatment, before the periodontal surgeries. A, Occlual view of upper arch. Trans-palatal arch was inserted for control of the molar width. B, Frontal view. Intrusion arch was used to intrude anterior teeth. C, Occlual view of lower arch. Extraction space was almost closed. D, Right buccal view. Retraction with temporary anchorage devices was ongoing with the redundant tissues present at the upper buccal side. E, Lateral view of anterior teeth. Large overjet was present due to difficulty of retraction of upper teeth. F, Left buccal view. Redundant tissue was also present around premolar and molar region. Despite of absolute anchorage provided for retraction, upper anterior teeth remained at this position. Lower anterior teeth were successfully being retracted with powerchains from miniscrews to long hooks on arch wire.
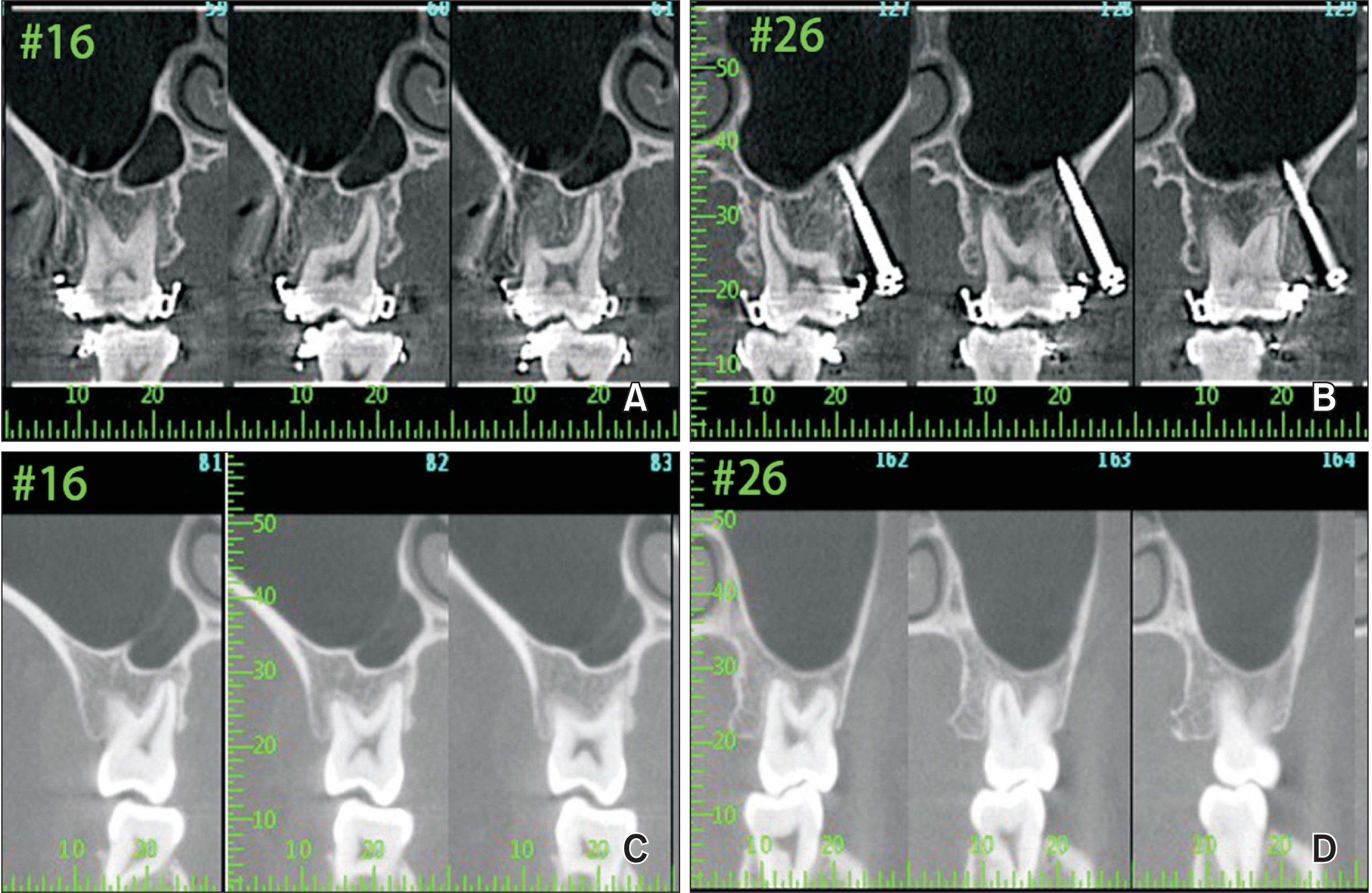
Figure 4 Cone-beam computed tomography images before and after the osseous resective surgeries of the maxillary first molars. A, B, Before the periodontal surgeries, please note that the bracket hooks of the upper right and left first molars were impinging on the alveolar bone. The enamel-cementum junction of upper right and left first molars were below the buccal bone crest. C, D, One year and 6 months after the osseous resective surgeries. No angular bony defects were noticed of upper right and left first molars and the tooth-bone relationships were stable after the surgeries.
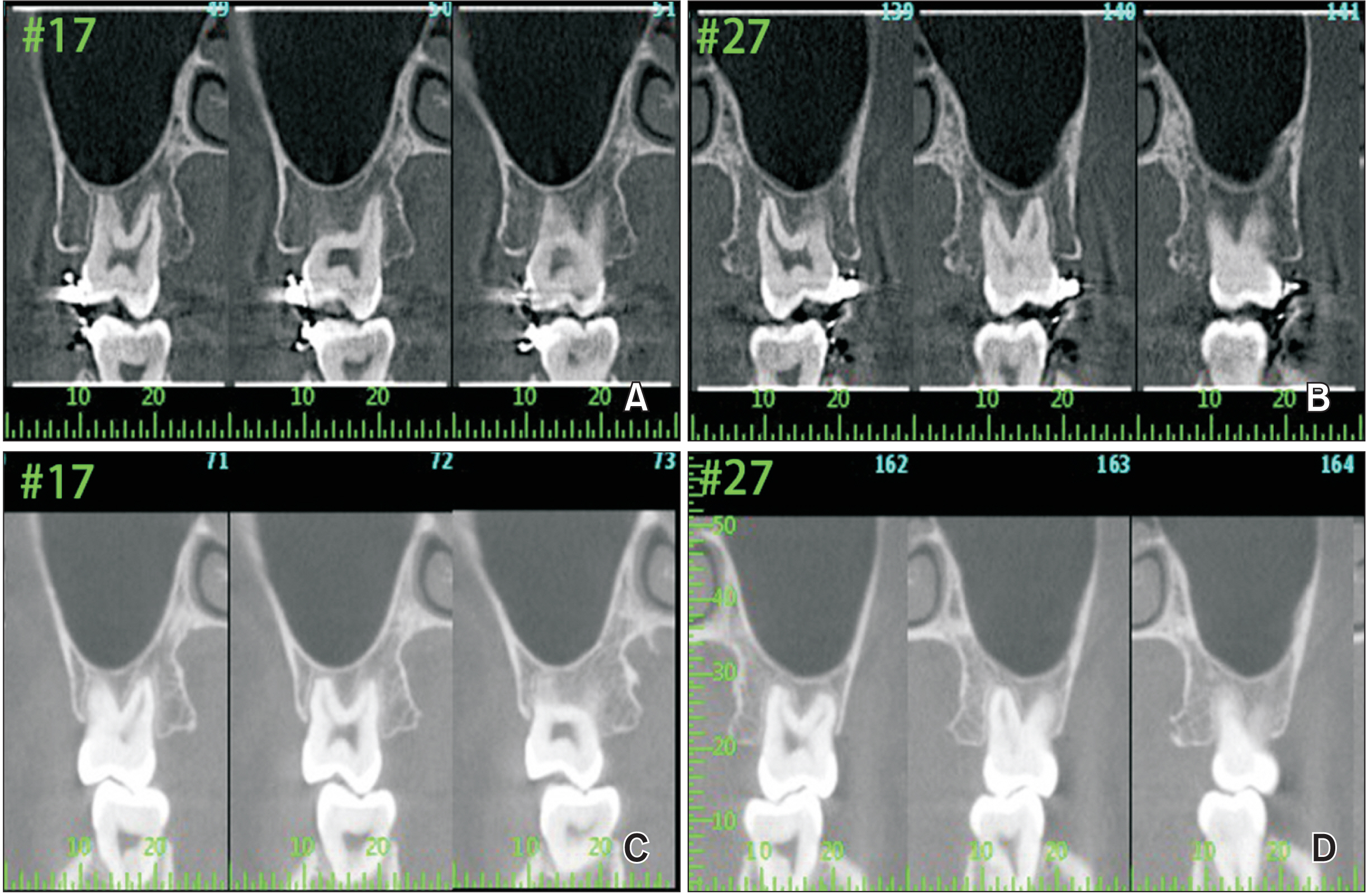
Figure 5 Cone-beam computed tomography images before and after the osseous resective surgeries of the maxillary second molars. A, B, The bulging alveolar bone and the angular bony defects at the buccal side of the upper right and left second molars were noticed before the osseous resective surgeries. C, D, One year and 6 months after the osseous resective surgeries. No angular bony defects were noticed of upper right and left second molars and the tooth-bone relationships were stable after the surgeries.

Figure 6 Intra-oral photographs of surgery at upper left posterior region. A, Pre-operative occlusal view at the upper left arch. Short clinical crowns were noticed from the upper left second premolar to second molar. A soft tissue indentation at the buccal side of upper left first molar was conspicuous after bracket debonding. B, Unfavorable bony architectures were noticed after the full thickness flap was reflected. C, D, Osteoplasty was performed with a high-speed carbide bur for grooving and the back action chisel to separate the redundant bone. E, Natural bony architecture was restored following the osteoplasty. F, The wound was primarily closed by a 5-0 Nylon suture.
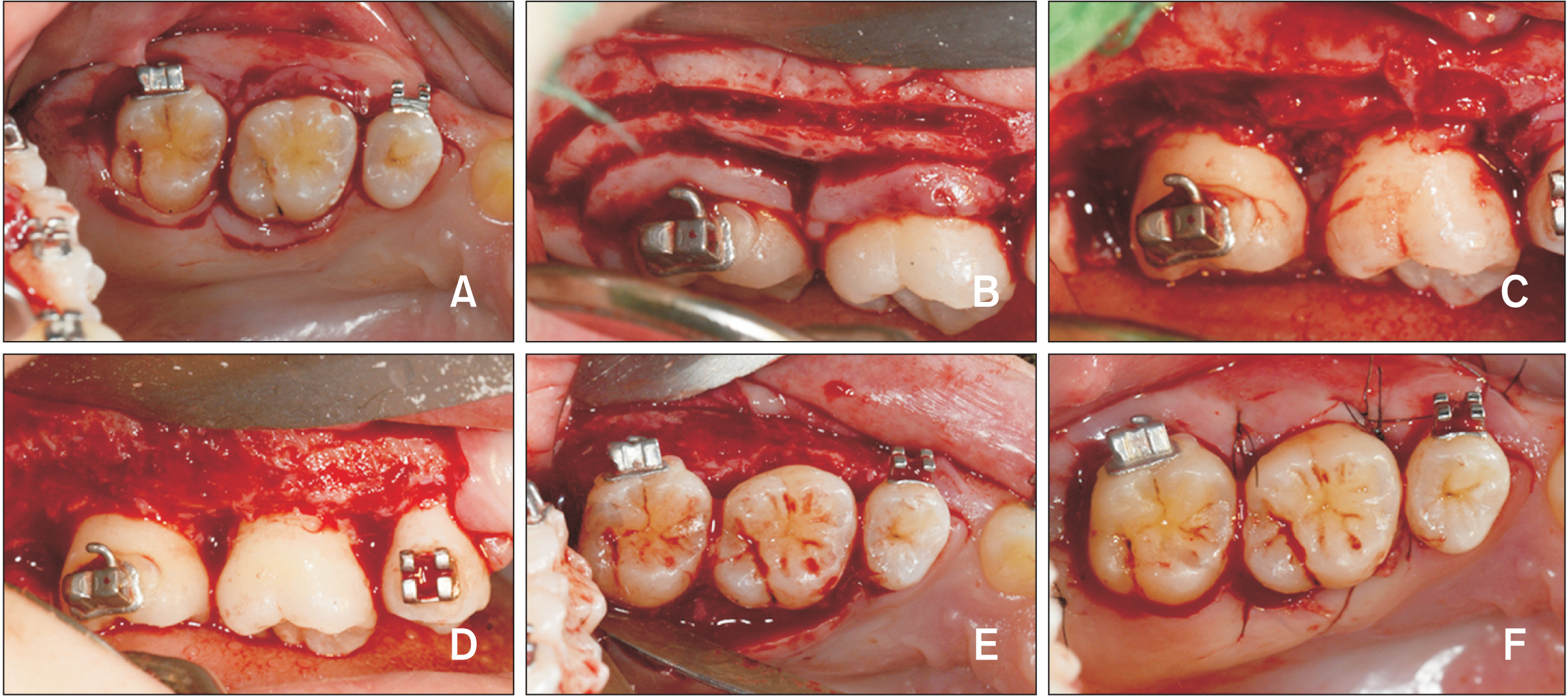
Figure 7 Post-treatment facial and intra-oral photographs. Pleasant profile was achieved after full retraction of anterior teeth with maximum anchorage.

Figure 8 Intra-oral photographs of surgery at upper right posterior region. A, Sub-marginal incisions were made at the upper right arch by No. 12 & 15C blades. B, Horizontal bony cut 2 mm below the soft tissue incision was made by a high-speed carbide bur after the full thickness flap being reflected. C, The hard and soft tissues were removed carefully as a whole for biopsy. D, E, Natural bony architecture was restored following alveoloplasty. F, The wound was primarily closed by a 5-0 Nylon suture.
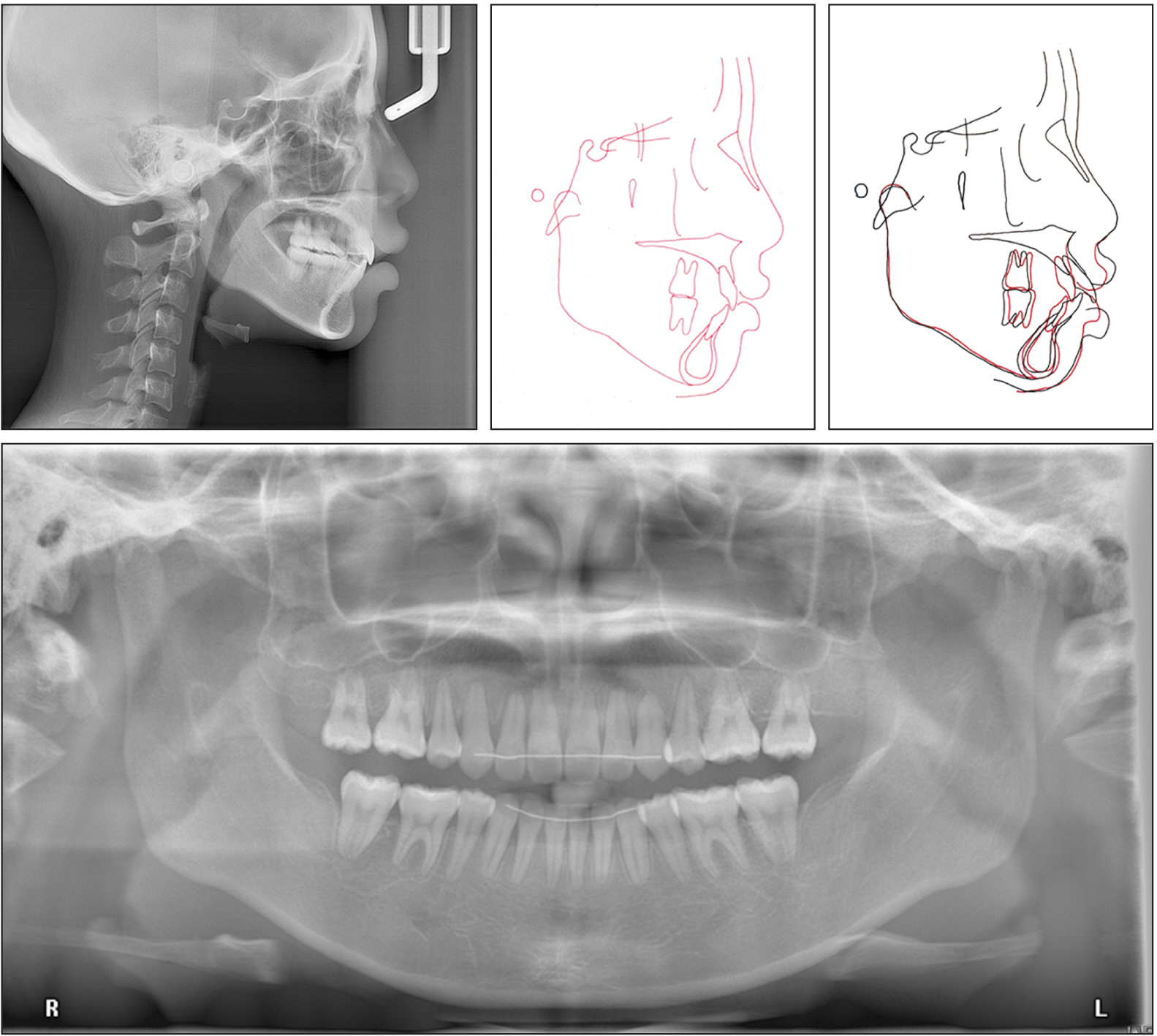
Figure 9 Post-treatment lateral cephalogram, cephalogram tracing and superimposition, and panoramic radiograph.

Figure 10 Tissue biopsy and histological analysis. A, The surgical photograph before the specimen was harvested. B, Specimen freshly harvested, before histological processing. C, Hematoxylin and eosin (H&E) staining of the histological section of the representative area 1–6 along the tooth axis shows buccal gingiva (G, green color) and underlying alveolar bone (B, green color) under tooth intrusion. Inserted boxes (1–6) are the low power views of Figure 11A–F. Dotted line indicates where the dental crown is (H&E, 20×). Higher magnification pictures from inserted boxes in low power view pictures (Figure 11).

Figure 11 Higher magnification pictures from the inserted boxes in Figure 10. A, Buccal gingiva: the gingiva is covered by parakeratinized squamous epithelium and supported by dense fibrous lamina propria. No obvious inflammatory cells infiltrate underneath the epithelium. B, C, Along the surface facing the crown, a few sulcular epithelium and bacterial colonies most likely dental plaque or calculus, are present. This presents an interface between teeth and the redundant tissue. Some chronic inflammatory cells that infiltrate underneath the non-keratinized sulcular epithelium are noted with abundant capillaries filled with red blood cells. D, Bacterial colonies are observed at the bottom of this triangle area between bone and intruded tooth. E, The bone close to the sulcular region at the bottom shows bone remodeling and woven bone formation with plump osteocytes in the lacunae. F, The bone facing buccal side without covering soft tissue, which has been preserved for clinical suturing, is composed of dense and mature laminated bone with small osteocytes in the lacunae and fibrovascular tissue in the Haversian canals, indicating a relatively slow turnover of bone here (H&E, A, E: 100×; B, C, F: 200×; D: 400×).
Reference
-
1. Gainsforth BL, Higley L. 1945; A study of orthodontic anchorage possibilities in basal bone. Am J Orthod Oral Surg. 31:406–17. DOI: 10.1016/0096-6347(45)90025-1.2. Brånemark PI, Hansson BO, Adell R, Breine U, Lindström J, Hallén O, et al. 1977; Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 16:1–132. PMID: 356184.3. Creekmore TD, Eklund MK. 1983; The possibility of skeletal anchorage. J Clin Orthod. 17:266–9. PMID: 6574142.4. Yao CC, Wu CB, Wu HY, Kok SH, Chang HF, Chen YJ. 2004; Intrusion of the overerupted upper left first and second molars by mini-implants with partial-fixed orthodontic appliances: a case report. Angle Orthod. 74:550–7. DOI: 10.1043/0003-3219(2004)074<0550:IOTOUL>2.0.CO;2. PMID: 15387035.5. Kravitz ND, Kusnoto B, Tsay PT, Hohlt WF. 2007; Intrusion of overerupted upper first molar using two orthodontic miniscrews. A case report. Angle Orthod. 77:915–22. DOI: 10.2319/050106-187.1. PMID: 17902236.6. Sherwood KH, Burch JG, Thompson WJ. 2002; Closing anterior open bites by intruding molars with titanium miniplate anchorage. Am J Orthod Dentofacial Orthop. 122:593–600. DOI: 10.1067/mod.2002.128641. PMID: 12490869.7. Erverdi N, Keles A, Nanda R. 2004; The use of skeletal anchorage in open bite treatment: a cephalometric evaluation. Angle Orthod. 74:381–90. DOI: 10.1043/0003-3219(2004)074<0381:TUOSAI>2.0.CO;2. PMID: 15264651.8. Park YC, Lee HA, Choi NC, Kim DH. 2008; Open bite correction by intrusion of posterior teeth with miniscrews. Angle Orthod. 78:699–710. DOI: 10.2319/0003-3219(2008)078[0699:OBCBIO]2.0.CO;2. PMID: 18302471.9. Togawa R, Iino S, Miyawaki S. 2010; Skeletal Class III and open bite treated with bilateral sagittal split osteotomy and molar intrusion using titanium screws. Angle Orthod. 80:1176–84. DOI: 10.2319/021910-102.1. PMID: 20677972. PMCID: PMC8929500.10. Marzouk ES, Abdallah EM, El-Kenany WA. 2015; Molar intrusion in open-bite adults using zygomatic miniplates. Int J Orthod Milwaukee. 26:47–54. PMID: 26349291.11. Alsafadi AS, Alabdullah MM, Saltaji H, Abdo A, Youssef M. 2016; Effect of molar intrusion with temporary anchorage devices in patients with anterior open bite: a systematic review. Prog Orthod. 17:9. DOI: 10.1186/s40510-016-0122-4. PMID: 26980200. PMCID: PMC4803715. PMID: 2bfea0e6693d479088c4e96e5a695b05.12. Bayani S, Heravi F, Radvar M, Anbiaee N, Madani AS. 2015; Periodontal changes following molar intrusion with miniscrews. Dent Res J (Isfahan). 12:379–85. DOI: 10.4103/1735-3327.161462. PMID: 26288629. PMCID: PMC4533198. PMID: 0a618b5a98de4bf39ffe06a5fcb897fd.13. Marzouk ES, Kassem HE. 2016; Evaluation of long-term stability of skeletal anterior open bite correction in adults treated with maxillary posterior segment intrusion using zygomatic miniplates. Am J Orthod Dentofacial Orthop. 150:78–88. DOI: 10.1016/j.ajodo.2015.12.014. PMID: 27364209.14. Yao CC, Lee JJ, Chen HY, Chang ZC, Chang HF, Chen YJ. 2005; Maxillary molar intrusion with fixed appliances and mini-implant anchorage studied in three dimensions. Angle Orthod. 75:754–60. DOI: 10.1043/0003-3219(2005)75[754:MMIWFA]2.0.CO;2. PMID: 16279822.15. Daimaruya T, Takahashi I, Nagasaka H, Umemori M, Sugawara J, Mitani H. 2003; Effects of maxillary molar intrusion on the nasal floor and tooth root using the skeletal anchorage system in dogs. Angle Orthod. 73:158–66. DOI: 10.1043/0003-3219(2003)73<158:EOMMIO>2.0.CO;2. PMID: 12725372.16. Kanzaki R, Daimaruya T, Takahashi I, Mitani H, Sugawara J. 2007; Remodeling of alveolar bone crest after molar intrusion with skeletal anchorage system in dogs. Am J Orthod Dentofacial Orthop. 131:343–51. DOI: 10.1016/j.ajodo.2006.04.025. PMID: 17346589.17. Graber LW, Vanarsdall RL Jr., Vig KWL. 2011. Orthodontics: current principles and techniques. 5th ed. Mosby;Louis: DOI: 10.1016/0002-9416(85)90010-7.18. Sugawara J, Baik UB, Umemori M, Takahashi I, Nagasaka H, Kawamura H, et al. 2002; Treatment and posttreatment dentoalveolar changes following intrusion of mandibular molars with application of a skeletal anchorage system (SAS) for open bite correction. Int J Adult Orthodon Orthognath Surg. 17:243–53. PMID: 12592995.19. Murakami T, Yokota S, Takahama Y. 1989; Periodontal changes after experimentally induced intrusion of the upper incisors in Macaca fuscata monkeys. Am J Orthod Dentofacial Orthop. 95:115–26. DOI: 10.1016/0889-5406(89)90390-9. PMID: 2916468.20. Hong SY, Shin JW, Hong C, Chan V, Baik UB, Kim YH, et al. 2019; Alveolar bone remodeling during maxillary incisor intrusion and retraction. Prog Orthod. 20:47. DOI: 10.1186/s40510-019-0300-2. PMID: 31867679. PMCID: PMC6926139. PMID: e0480c60d993430db766b7c0b195b316.21. Newman MG, Takei H, Klokkevold PR, Carranza FA. 2015. Carranza's clinical periodontology. 12th ed. Elsevier Science;St. Louis:22. da Silva VC, Cirelli CC, Ribeiro FS, Leite FR, Benatti Neto C, Marcantonio RA, et al. 2008; Intrusion of teeth with class III furcation: a clinical, histologic and histometric study in dogs. J Clin Periodontol. 35:807–16. DOI: 10.1111/j.1600-051X.2008.01293.x. PMID: 18662302.23. Chung CJ, Jang W, Piers C, Lee DW, Hwang S, Kim KH, et al. 2019; Differential alveolar bone modeling after orthodontic retraction. J Am Dent Assoc. 150:313–20. DOI: 10.1016/j.adaj.2018.12.029. PMID: 30922461.24. Weltman B, Vig KW, Fields HW, Shanker S, Kaizar EE. 2010; Root resorption associated with orthodontic tooth movement: a systematic review. Am J Orthod Dentofacial Orthop. 137:462–76. discussion 12ADOI: 10.1016/j.ajodo.2009.06.021. PMID: 20362905.25. Moon CH, Wee JU, Lee HS. 2007; Intrusion of overerupted molars by corticotomy and orthodontic skeletal anchorage. Angle Orthod. 77:1119–25. DOI: 10.2319/092705-334.1. PMID: 18004918.26. Bellini-Pereira SA, Almeida J, Aliaga-Del Castillo A, Dos Santos CCO, Henriques JFC, Janson G. 2021; Evaluation of root resorption following orthodontic intrusion: a systematic review and meta-analysis. Eur J Orthod. 43:432–41. DOI: 10.1093/ejo/cjaa054. PMID: 32968763.27. Kuroda S, Katayama A, Takano-Yamamoto T. 2004; Severe anterior open-bite case treated using titanium screw anchorage. Angle Orthod. 74:558–67. DOI: 10.1043/0003-3219(2004)074<0558:SAOCTU>2.0.CO;2. PMID: 15387036.28. Lee HA, Park YC. 2008; Treatment and posttreatment changes following intrusion of maxillary posterior teeth with miniscrew implants for open bite correction. Korean J Orthod. 38:31–40. DOI: 10.4041/kjod.2008.38.1.31.29. Baek MS, Choi YJ, Yu HS, Lee KJ, Kwak J, Park YC. 2010; Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth. Am J Orthod Dentofacial Orthop. 138:396.e1–e9. DOI: 10.1016/j.ajodo.2010.04.023. PMID: 20889043.30. González Espinosa D, de Oliveira Moreira PE, da Sousa AS, Flores-Mir C, Normando D. 2020; Stability of anterior open bite treatment with molar intrusion using skeletal anchorage: a systematic review and meta-analysis. Prog Orthod. 21:35. DOI: 10.1186/s40510-020-00328-2. PMID: 32888097. PMCID: PMC7474024. PMID: a91612bfb3a442b38c7e6d75ab4cdad8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nonextraction treatment of Class II division 2 in an adult patient using microimplant anchorage (MIA)
- Effectiveness of anchorage with temporary anchorage devices during anterior maxillary tooth retraction: A randomized clinical trial
- Orthodontic Traction of the Permanent Molar Using Skeletal Anchorage: A Case Report
- Three-dimensional analysis of the distal movement of maxillary 1st molars in patients fitted with mini-implant-aided trans-palatal arches
- Maxillary protraction treatment of skeletal Class III children using miniplate anchorage
