Treatment for subarachnoid hemorrhage due to ruptured posterior cerebral arterial dolichoectasia with aortic arch anomaly
- Affiliations
-
- 1Department of Neurosurgery, Yeungnam University Medical Center, Deagu, Korea
- KMID: 2540809
- DOI: http://doi.org/10.7461/jcen.2022.E2022.03.002
Abstract
- Subarachnoid hemorrhage (SAH) due to ruptured posterior cerebral artery (PCA) intracranial arterial dolichoectasia (IADE) is very rare. As these lesions are difficult to treat microsurgically, neurointervention is preferred because the dolichoectatic artery does not have a clear neck, and the surgical field of view was deep seated with the SAH. However, in some cases, neurointervention is difficult due to anatomical variation of the blood vessel to access the lesion. In this case, a 30-year-old male patient presented with a ruptured PCA IADE and an aortic arch anomaly. Aortic arch anomalies render it difficult to reach the ruptured PCA IADE via endovascular treatment. The orifice of the vertebral artery (VA) was different from the usual cases, so it was difficult to find the entrance. After only finding the VA and arriving at the lesion along the VA, trapping was performed. Herein, we report the PCA IADE with aortic arch anomaly endovascular treatment methods and results.
Keyword
Figure
-
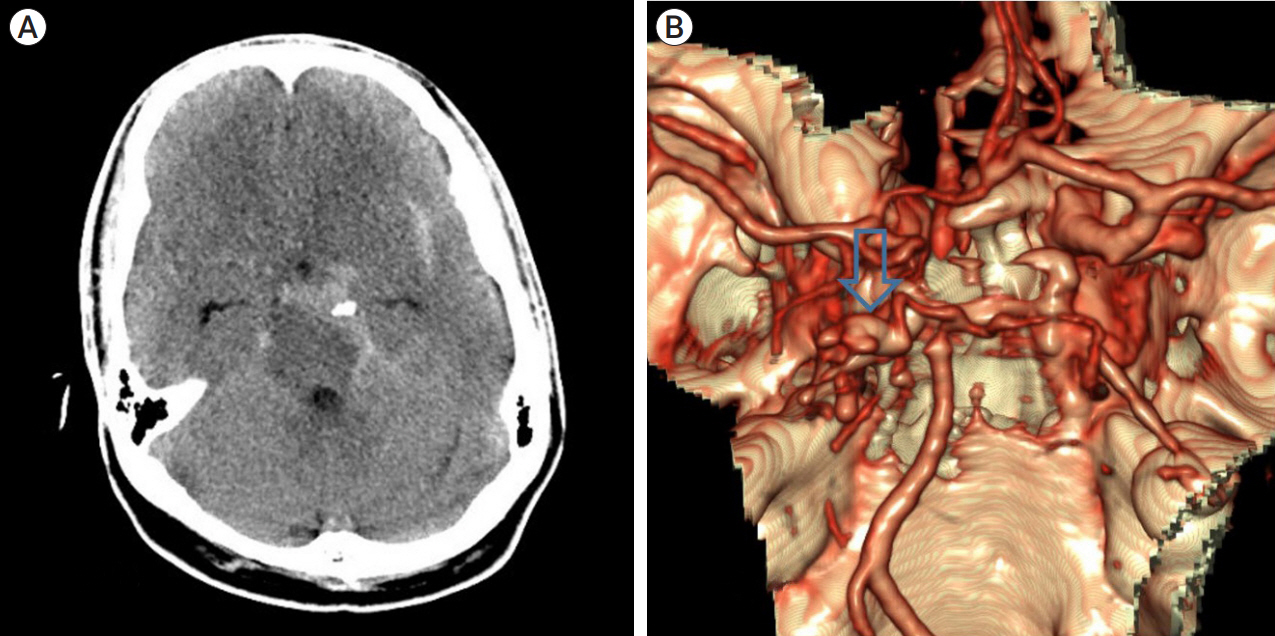
Fig. 1. Brain multi-phased computed tomography angiography is showing subarachnoid hemorrhage in basal on left crural cistern and left ambient cistern (A). Three-dimensional reconstructed angiography showed left P2 segment were elongated and enlarged (arrow) (B).
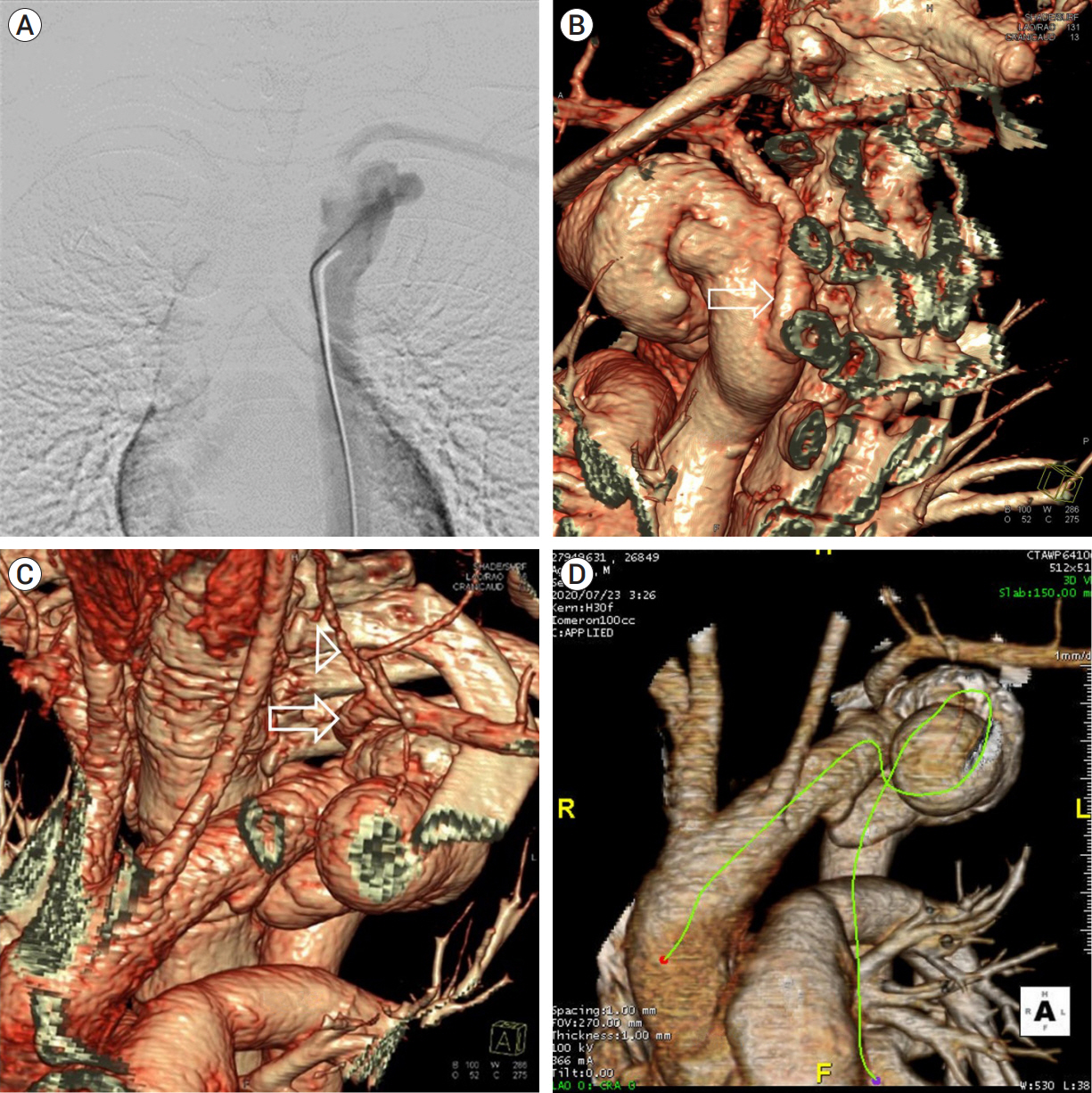
Fig. 2. In anteroposterior view of aortogram, the left subclavian artery was identified, but the left vertebral artery (VA) was not seen and the shape of the aortic arch was unusual (A). Aortic arch three-dimensional image, left subclavian artery comes off posteriorly from the descending aorta at the level of T4. Arrow: left subclavian artery (B). From the left subclavian artery orifice to the left subclavian artery at the level of T1, it is pointing to the right. After passing the left first rib, it turns to the left. Left VA comes off superiorly from the left subclavian artery at the level of T2. Arrow: left subclavian artery, Arrowhead: left VA (C). From the aortic arch to the ascending aorta, it is clockwise. Two aortic arch aneurysm is found (D).

Fig. 3. Left vertebral artery angiogram, working view showing a tortuous and elongated Lt. P2 (A, B). After first, second coil was inserted (C). Followed angiogram, there were no distal flow left posterior cerebral artery after the coil embolization (D). Followed stroke magnetic resonance imaging (MRI), there were focal acute infarction on left lateral thalamus (E).
Reference
-
1. Al-Atassi T, Khoynezhad A. Indications for aortic arch intervention. Semin Cardiothorac Vasc Anesth. 2016; Dec. 20(4):259–64.2. Baccin CE, Krings T, Alvarez H, Ozanne A, Lasjaunias PL. A report of two cases with dolichosegmental intracranial arteries as a new feature of PHACES syndrome. Child Nerv Syst. 2007; May. 23(5):559–67.3. Chao KH, Riina HA, Heier L, Steig PE, Gobin YP. Endovascular management of dolichoectasia of the posterior cerebral artery report. AJNR Am J Neuroradiol. 2004; Nov-Dec. 25(10):1790–1.4. Coert BA, Chang SD, Do HM, Marks MP, Steinberg GK. Surgical and endovascular management of symptomatic posterior circulation fusiform aneurysms. J Neurosurg. 2007; May. 106(5):855–65.5. Dziewasa R, Freund M, Ludemann P, Muller M, Ritter M, Droste DW, et al. Treatment options in vertebrobasilar dolichoectasia–case report and review of the literature. Eur Neurol. 2003; 49(4):245–7.6. Gutierrez J, Sacco RL, Wright CB. Dolichoectasia-an evolving arterial disease. Nat Rev Neurol. 2011; Jan. 7(1):41–50.7. Hanneman K, Newman B, Chan F. Congenital variants and anomalies of the aortic arch. Radiographics. 2017; Jan-Feb. 37(1):32–51.8. Mantri SS, Raju B, Jumah F, Rallo MS, Nagaraj A, Khandelwal P, et al. Aortic arch anomalies, embryology and their relevance in neuro-interventional surgery and stroke: a review. Interv Neuroradiol. 2022; Aug. 28(4):489–98.9. Menshawi K, Mohr JP, Gutierrez J. A functional perspective on the embryology and anatomy of the cerebral blood supply. J Stroke. 2015; May. 17(2):144–58.10. O’Shaughnessy BA, Getch CC, Bendok BR, Parkinson RJ, Batjer HH. Progressive growth of a giant dolichoectatic vertebrobasilar artery aneurysm after complete Hunterian occlusion of the posterior circulation: case report. Neurosurgery. 2004; Nov. 55(5):1223.11. Passero SG, Calchetti B, Bartalini S. Intracranial bleeding in patients with vertebrobasilar dolichoectasia. Stroke. 2005; Jul. 36(7):1421–5.12. Pereira-Filho A, Faria M, Bleil C, Kraemer JL. Brainstem compression syndrome caused by vertebrobasilar dolichoectasia: microvascular repositioning technique. Arq Neuropsiquiatr. 2008; Jun. 66(2B):408–11.13. Ubogu EE, Zaidat OO. Intracranial arterial dolichoectasia is associated with enlarged descending thoracic aorta. Neurology. 2005; Nov. 65(10):1681–2.14. Pico F, Labreuche J, Amarenco P. Pathophysiology, presentation, prognosis, and management of intracranial arterial dolichoectasia. Lancet Neurol. 2015; Aug. 14(8):833–45.15. Pico F, Labreuche J, Hauw JJ, Seilhean D, Duyckaerts C, Amarenco P. Coronary and basilar artery ectasia are associated: results from an autopsy case-control study. Stroke. 2016; Jan. 47(1):224–7.16. Rabb CH, Barnwell SL. Catastrophic subarachnoid hemorrhage resulting from ruptured vertebrobasilar dolichoectasia: case report. Neurosurgery. 1998; Feb. 42(2):379–82.17. Rathore L, Yamada Y, Kawase T, Kato Y, Senapati SB. A 5-year follow-up of intracranial arterial dolichoectasia: a case report and review of literature. Asian J Neurosurg. 2019; Nov. 14(4):1302–7.18. Siddiqui A, Chew NS, Miszkiel K. Vertebrobasilar dolichoectasia: a rare cause of obstructive hydrocephalus: case report. Br J Radiol. 2008; Apr. 81(964):e123–6.19. Sokolov AA, Husain S, Sztajzel R, Croquelois A, Lobrinus JA, Thaler D, et al. Fatal subarachnoid hemorrhage following ischemia in vertebrobasilar dolichoectasia. Medicine (Baltimore). 2016; Jul. 95(27):e4020.20. Yamaguchi S, Ito O, Maeda Y, Murata H, Imamoto N, Yuhi F, et al. Coil embolization for a ruptured posterior cerebral artery aneurysm with vertebrobasilar dolichoectasia. Neurol Med Chir (Tokyo). 2011; 51(9):657–60.21. Yuan YJ, Xu K, Luo Q, Yu JL. Research progress on vertebrobasilar dolichoectasia. Int J Med Sci. 2014; Aug. 11(10):1039–48.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Large Dolichoectasia Concurrently Involving Both Anterior and Posterior Cerebral Circulation: A Case Report
- Subarachnoid Hemorrhage Due to a Ruptured Middle Cerebral Artery Bifurcation Aneurysm Superimposed by an Idiopathic Intracerebral Hematoma
- Spontaneous Anterior Cerebral Artery Dissection Presenting with Simultaneous Subarachnoid Hemorrhage and Cerebral Infarction in a Patient with Multiple Extracranial Arterial Dissections
- CT findings of subarachnoid hemorrhage due to ruptured cerebral aneurysm
- The Short Term Results of the Total Aortic Arch Replacement with Arch First Technique
