A case report of successfully treated metachronous gastrointestinal stromal tumor and colon cancer
- Affiliations
-
- 1Department of Radiology, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea
- 2Division of Hematology and Oncology, Department of Internal Medicine, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea
- KMID: 2540764
- DOI: http://doi.org/10.7180/kmj.22.138
Abstract
- The diagnosis of gastrointestinal stromal tumor (GIST) has become relatively common in recent years, but little is known about its association with other malignancies. We present a rare case of successfully treated metachronous GIST and colon cancer with concurrent FOLFOX (5-fluorouracil, leucovorin, and oxaliplatin) chemotherapy and imatinib. A 63-year-old man presented with abdominal pain that had started 2 weeks ago, and endoscopic ultrasonography showed masses that were compatible with GIST on the duodenum. He underwent Whipple surgery. One year after the GIST diagnosis, two liver masses were found on abdominal computed tomography images taken for surveillance. A liver biopsy showed metastatic adenocarcinoma, not GIST. Colonoscopy was then performed to identify the primary site of the metastatic adenocarcinoma in the liver, and sigmoid colon cancer was found. He received 12 cycles of adjuvant FOLFOX concurrently with adjuvant imatinib. There were no serious adverse events of grade 3 or higher from either imatinib or chemotherapy. He has completed adjuvant imatinib and FOLFOX chemotherapy and there is no evidence of disease recurrence. When a synchronous or metachronous tumor is found in a GIST patient, the clinician should keep in mind the possibility of another primary tumor of different histopathology, as well as GIST recurrence.
Figure
-
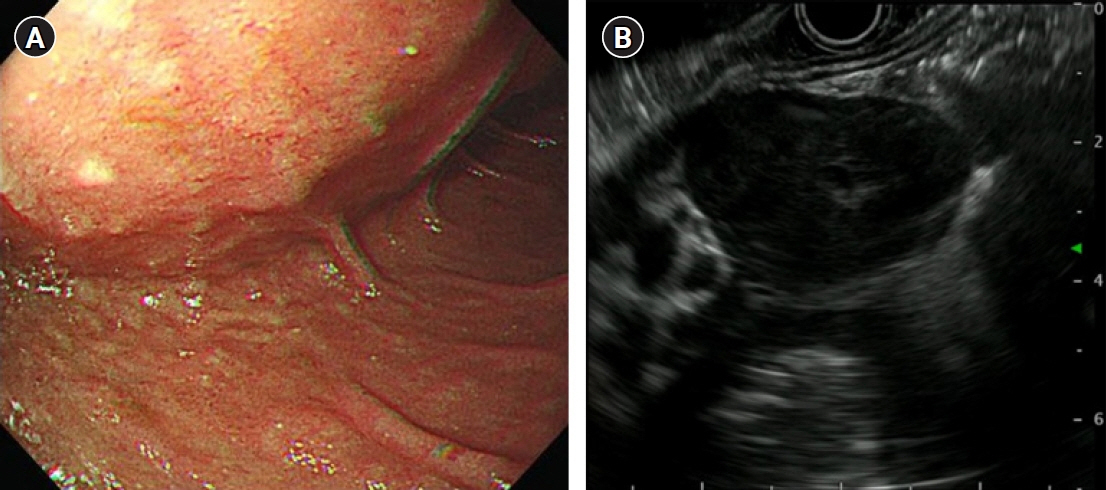
Fig. 1. Endoscopic and endoscopic ultrasonographic findings of gastrointestinal stromal tumor. (A) Bulging at the duodenal second portion and (B) an inhomogeneous hypoechoic oval mass with regular margins and a largest diameter of 42 mm.

Fig. 2. Computed tomographic findings of gastrointestinal stromal tumor. There was circumferential wall thickening with aneurysmal dilatation of the second and third portions of the duodenum (arrow). There was no bowel obstruction or organ invasion by the mass.

Fig. 3. Gross and microscopic findings of the surgically resected gastrointestinal stromal tumor specimen. (A) Three exophytic oval masses (arrows). (B) A well-defined submucosal tumor (hematoxylin and eosin staining, ×40). The immunohistochemical staining results were positive for CD117 (C) and positive for CD34 (D) (×100). CD, cluster of differentiation.

Fig. 4. Computed tomographic findings of two liver metastases (arrow). (A) A 2.4-cm metastatic mass at liver segment 8. (B) An 0.6-cm metastatic nodule at liver segment 5.

Fig. 5. Colonoscopic findings of colon cancer. (A) A large fungating mass at the sigmoid colon. (B) Microscopic findings of moderately differentiated colon adenocarcinoma (hematoxylin and eosin staining, ×40).
Reference
-
References
1. Soreide K, Sandvik OM, Soreide JA, Giljaca V, Jureckova A, Bulusu VR. Global epidemiology of gastrointestinal stromal tumours (GIST): a systematic review of population-based cohort studies. Cancer Epidemiol. 2016; 40:39–46.2. Patel N, Benipal B. Incidence of gastrointestinal stromal tumors in the United States from 2001-2015: a United States cancer statistics analysis of 50 states. Cureus. 2019; 11:e4120.3. Miettinen M, Sobin LH, Lasota J. Gastrointestinal stromal tumors of the stomach: a clinicopathologic, immunohistochemical, and molecular genetic study of 1765 cases with long-term follow-up. Am J Surg Pathol. 2005; 29:52–68.4. Urbanczyk K, Limon J, Korobowicz E, Chosia M, Sygut J, Karcz D, et al. Gastrointestinal stromal tumors: a multicenter experience. Pol J Pathol. 2005; 56:51–61.5. Stratakis CA, Carney JA. The triad of paragangliomas, gastric stromal tumours and pulmonary chondromas (Carney triad), and the dyad of paragangliomas and gastric stromal sarcomas (Carney-Stratakis syndrome): molecular genetics and clinical implications. J Intern Med. 2009; 266:43–52.6. Au WY, Ho KM, Shek TW. Papillary renal cell carcinoma and gastrointestinal stromal tumor: a unique association. Ann Oncol. 2004; 15:843–4.7. Agaimy A, Wunsch PH, Sobin LH, Lasota J, Miettinen M. Occurrence of other malignancies in patients with gastrointestinal stromal tumors. Semin Diagn Pathol. 2006; 23:120–9.8. Wronski M, Ziarkiewicz-Wroblewska B, Gornicka B, Cebulski W, Slodkowski M, Wasiutynski A, et al. Synchronous occurrence of gastrointestinal stromal tumors and other primary gastrointestinal neoplasms. World J Gastroenterol. 2006; 12:5360–2.9. Liu YJ, Yang Z, Hao LS, Xia L, Jia QB, Wu XT. Synchronous incidental gastrointestinal stromal and epithelial malignant tumors. World J Gastroenterol. 2009; 15:2027–31.10. Arnogiannaki N, Martzoukou I, Kountourakis P, Dimitriadis E, Papathanasaki A, Nastoulis E, et al. Synchronous presentation of GISTs and other primary neoplasms: a single center experience. In Vivo. 2010; 24:109–15.11. Ruka W, Rutkowski P, Nowecki Z, Nasierowska-Guttmejer A, Debiec-Rychter M. Other malignant neoplasms in patients with gastrointestinal stromal tumors (GIST). Med Sci Monit. 2004; 10:LE13–4.12. Casali PG, Blay JY, Abecassis N, Bajpai J, Bauer S, Biagini R, et al. Gastrointestinal stromal tumours: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2022; 33:20–33.13. Corless CL, Fletcher JA, Heinrich MC. Biology of gastrointestinal stromal tumors. J Clin Oncol. 2004; 22:3813–25.14. Joensuu H, Eriksson M, Sundby Hall K, Hartmann JT, Pink D, Schutte J, et al. One vs three years of adjuvant imatinib for operable gastrointestinal stromal tumor: a randomized trial. JAMA. 2012; 307:1265–72.15. Raut CP, Espat NJ, Maki RG, Araujo DM, Trent J, Williams TF, et al. Efficacy and tolerability of 5-year adjuvant imatinib treatment for patients with resected intermediate- or high-risk primary gastrointestinal stromal tumor: the PERSIST-5 clinical trial. JAMA Oncol. 2018; 4:e184060.16. Kumar K, Rowsell C, Law C, Ko YJ. Coexistence of gastrointestinal stromal tumour and colorectal adenocarcinoma: two case reports. J Gastrointest Oncol. 2011; 2:50–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Exophytic Colon Cancer: Resemblance to a Gastrointestinal Stromal Tumor of the Stomach: A Case Report
- Treatment of Multiple Colorectal Cancers
- Unusual Metachronous Renal Pelvis and Colon Metastases in a Patient with Endometrial Cancer: A Case Report
- Totally Laparoscopic Resection for a Large Gastrointestinal Stromal Tumor of Stomach
- Synchronous Incidental Occurrence of Gastric Gastrointestinal Stromal Tumor and Colon Adenocarcinoma
