Circulating Tumor DNA–Based Genotyping and Monitoring for Predicting Disease Relapses of Patients with Peripheral T-Cell Lymphomas
- Affiliations
-
- 1Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Department of Health Sciences and Technology, Samsung Advanced Institute for Health Sciences and Technology, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Samsung Genome Institute Samsung Medical Center, Seoul, Korea
- 4GENINUS Inc., Seoul, Korea
- 5Department of Laboratory Medicine and Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 6Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2538012
- DOI: http://doi.org/10.4143/crt.2022.017
Abstract
- Purpose
Plasma circulating tumor DNA (ctDNA) could reflect the genetic alterations present in tumor tissues. However, there is little information about the clinical relevance of cell-free DNA genotyping in peripheral T-cell lymphoma (PTCL).
Materials and Methods
After targeted sequencing plasma cell-free DNA of patients with various subtypes of PTCL (n=94), we analyzed the mutation profiles of plasma ctDNA samples and their predictive value of dynamic ctDNA monitoring for treatment outcomes.
Results
Plasma ctDNA mutations were detected in 53 patients (56%, 53/94), and the detection rate of somatic mutations was highest in angioimmunoblastic T-cell lymphoma (24/31, 77%) and PTCL, not otherwise specified (18/29, 62.1%). Somatic mutations were detected in 51 of 66 genes that were sequenced, including the following top 10 ranked genes: RHOA, CREBBP, KMT2D, TP53, IDH2, ALK, MEF2B, SOCS1, CARD11, and KRAS. In the longitudinal assessment of ctDNA mutation, the difference in ctDNA mutation volume after treatment showed a significant correlation with disease relapse or progression. Thus, a ≥ 1.5-log decrease in genome equivalent (GE) between baseline and the end of treatment showed a significant association with better survival outcomes than a < 1.5-log decrease in GE.
Conclusion
Our results suggest the clinical relevance of plasma ctDNA analysis in patients with PTCL. However, our findings should be validated by a subsequent study with a larger study population and using a broader gene panel.
Figure
-
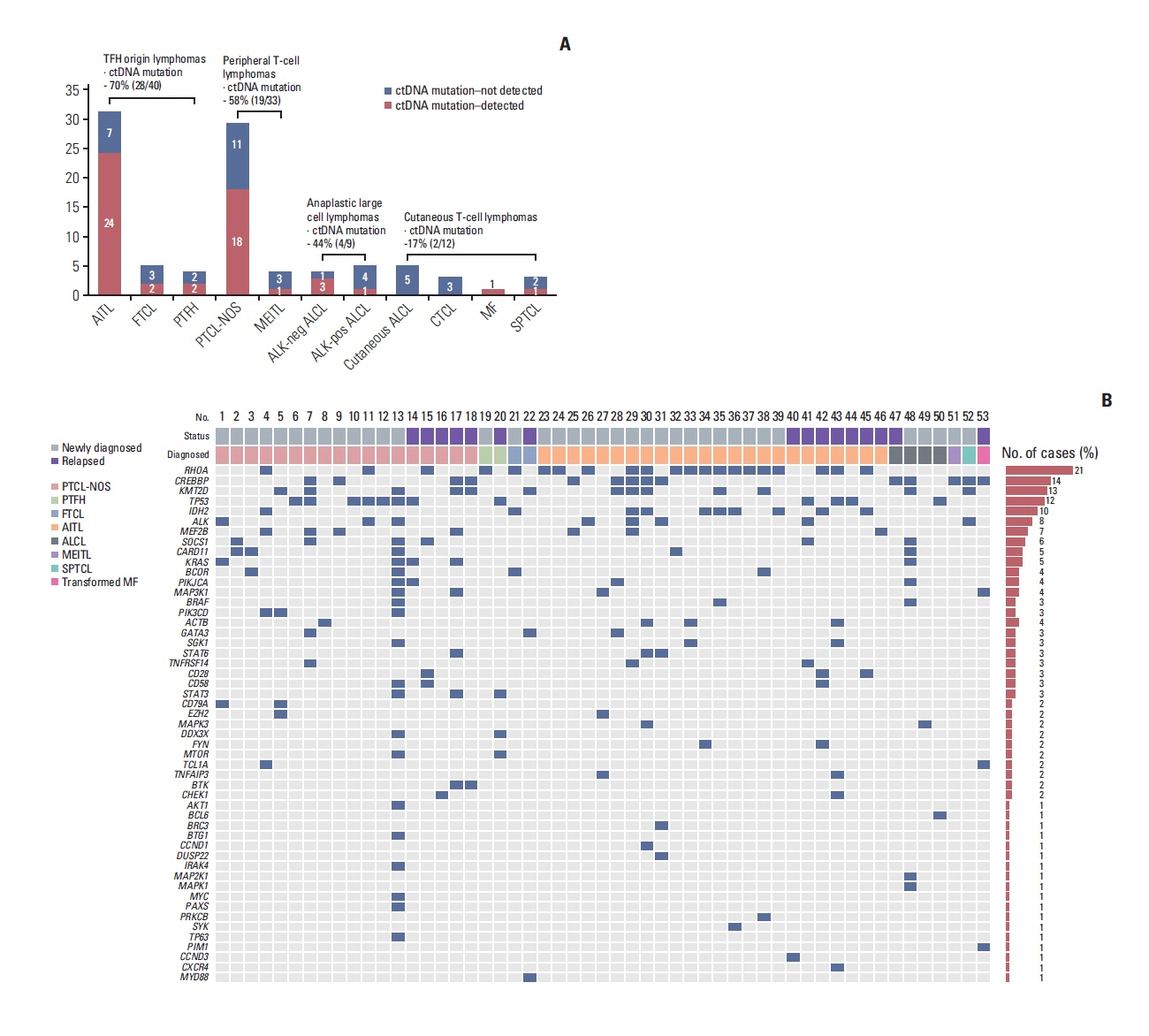
Fig. 1 The detection of plasma ctDNA mutations from 94 baseline samples and mutation profiles of plasma cell-free DNA in 53 patients with peripheral T-cell lymphoma obtained from the baseline samples of our prospective cohort. (A) The detection rate of somatic mutations was highest in two subtypes: AITL (24/31, 77%) and PTCL-NOS (18/29, 62.1%). The ctDNA mutation was detected more frequently in the groups with TFH lymphomas (70%, 28/40) and peripheral T-cell lymphomas (58%, 19/33) than in those with systemic ALCL (44%, 4/9) and cutaneous lymphomas (17%, 2/12). (B) Somatic mutations in RHOA, CREBBP, KMT2D, TP53, and IDH2 were most common across the subtypes. A red box represents the detected mutation of each gene. AITL, angioimmunoblastic T-cell lymphoma; ALCL, anaplastic large cell lymphoma; ALK, anaplastic lymphoma kinase; CTCL, cutaneous T-cell lymphoma; ctDNA, circulating tumor DNA; FTCL, follicular helper T-cell lymphoma; MEITL, monomorphic epitheliotropic intestinal T-cell lymphoma; MF, mycosis fungoides; PTCL-NOS, peripheral T-cell lymphoma, not otherwise specified; PTFH, peripheral T-cell lymphoma with T follicular helper type; SPTCL, subcutaneous panniculitis-like T-cell lymphoma; TFH, T follicular helper cell.
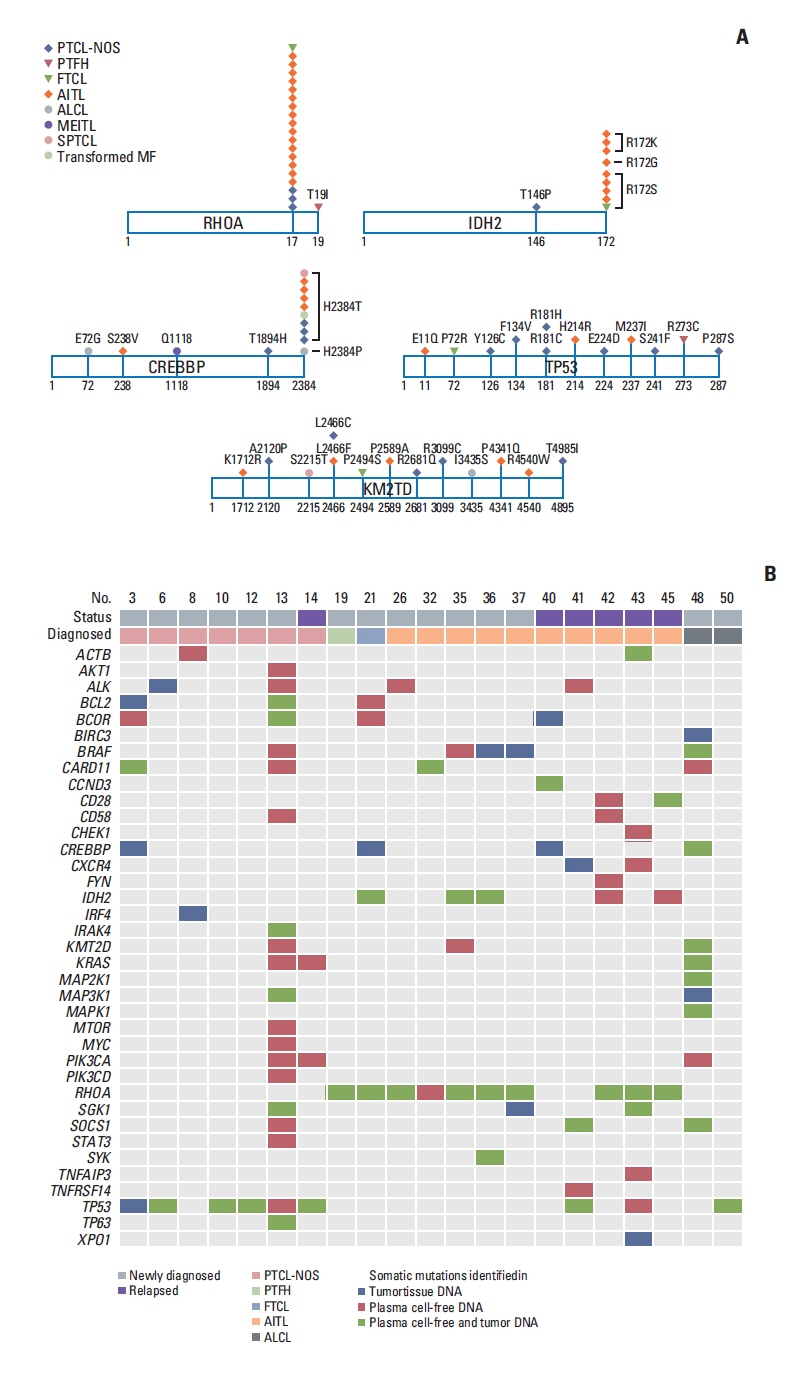
Fig. 2 Mutation sites of most common cell-free DNA mutations and the comparison of plasma ctDNA and tumor tissue DNA mutations. (A) Most cases harbored the RHOA mutation encoding p.Gly17Val, and the IDH2 mutations predominantly affected residue R172. The dominant mutation in CREBBP was at position 2384, including p.His2384Thr, whereas the mutation sites of TP53 and KM2TD did not overlap. (B) A paired analysis using 21 cases shows concordance of the somatic mutations in plasma cell-free DNA and tumor tissue. AITL, angioimmunoblastic T-cell lymphoma; ALCL, anaplastic large cell lymphoma; ctDNA, circulating tumor DNA; FTCL, follicular helper T-cell lymphoma; MEITL, monomorphic epitheliotropic intestinal T-cell lymphoma; MF, mycosis fungoides; PTCL-NOS, peripheral T-cell lymphoma, not otherwise specified; PTFH, peripheral T-cell lymphoma with T follicular helper type; SPTCL, subcutaneous panniculitis-like T-cell lymphoma.
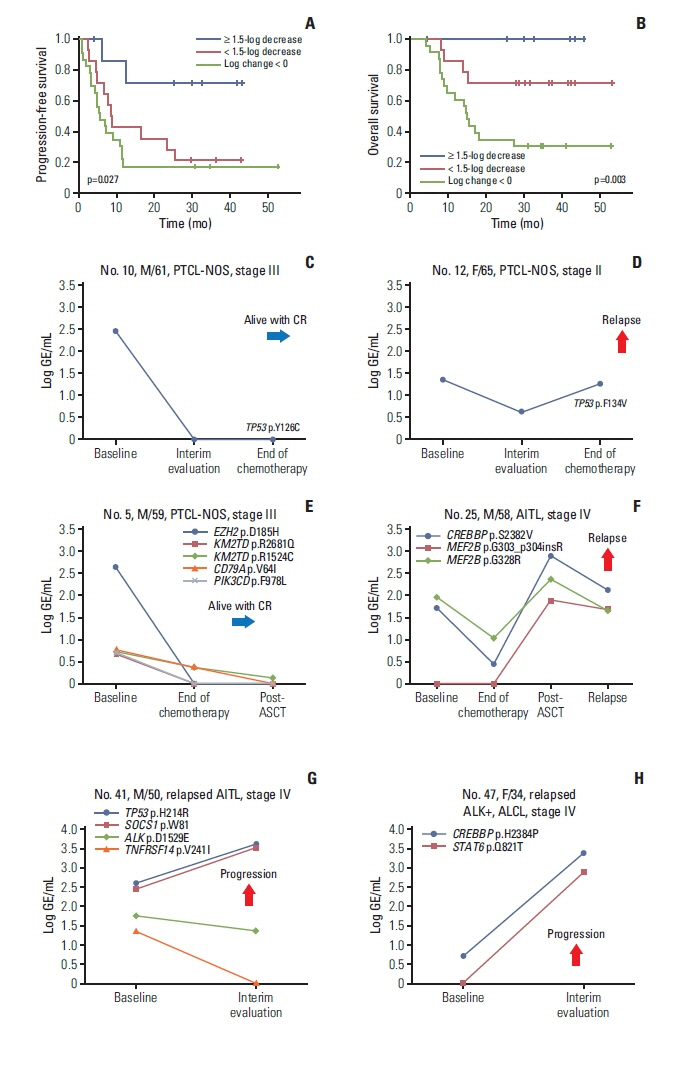
Fig. 3 Longitudinal analysis of plasma cell-free DNA mutations shows the correlation with treatment outcomes. (A, B) Patients with a decrease in mutation volume at the end of treatment (log change in genome equivalents ≥ 1.5) showed better progression-free and overall survival than patients showing increased mutation volume (log change in genome equivalents < 0) or a small decrease in mutation volume (log change in genome equivalents < 1.5). (C) A 61-year-old male with PTCL-NOS maintained a CR with loss of a TP53 mutation. (D) A 65-year-old female with PTCL-NOS showing an increase in a TP53 mutation at the end of treatment finally relapsed. (E) A 59-year-old male with PTCL-NOS maintained a complete response with a decrease in initially detected mutations including EZH2. (F) A 58-year-old male with AITL showed increases in CREBBP and MEF2B mutations after autologous stem cell transplantation and relapsed during follow-up. (G) A 50-year-old male with relapsed AITL showed increases in TP53 and SOCS1 mutations after salvage treatment during disease progression. (H) A 34-year-old female with ALK-positive ALCL showed increases in CREBBP and STAT6 mutation volumes after salvage therapy. AITL, angioimmunoblastic T-cell lymphoma; ALCL, anaplastic large cell lymphoma; ALK, anaplastic lymphoma kinase; ASCT, autologous stem cell transplantation; CR, complete response; GE, genome equivalent; PTCL-NOS, peripheral T-cell lymphoma, not otherwise specified.

Fig. 4 Monitoring of plasma cell-free DNA harboring somatic mutations revealed the emergence of new somatic mutations during disease relapse or progression. (A) A 56-year-old male with ALK-negative ALCL showed increases in CREBBP, SOCS1, MAPK1, and MAP2K1 mutations at the time of disease progression even after salvage therapy with brentuximab vedotin, whereas the mutations of KMT2D and BRAF showed different patterns according to the sites of mutations (top and middle). The mutations of PIM1, MTOR, and CARD11 increased as disease progressed, reflecting the emergence of new mutations (bottom). (B) A 57-year-old male with PTCL-NOS showed elevation of mutation volume in multiple genes such as CREBBP, KMT2D, GATA3, and MEF2B at the time of complete response and finally showed disease relapse together with further increases in those mutations after autologous stem cell transplantation (top and middle). As the patient exhibited relapse, new mutations such as BRAF and IRK1 appeared (bottom). (C) The mutation profiles of longitudinally assessed serial samples from 45 patients showed the increases in mutation volumes during disease progression or relapse predominantly in KMT2D, CREBBP, and MEF2B. ALCL, anaplastic large cell lymphoma; ALK, anaplastic lymphoma kinase; ASCT, autologous stem cell transplantation; GE, genome equivalent; PTCL-NOS, peripheral T-cell lymphoma, not otherwise specified.
Cited by 1 articles
-
Feasibility of Circulating Tumor DNA Analysis in Patients with Follicular Lymphoma
Sang Eun Yoon, Seung-Ho Shin, Dae Keun Nam, Junhun Cho, Won Seog Kim, Seok Jin Kim
Cancer Res Treat. 2024;56(3):920-935. doi: 10.4143/crt.2023.869.
Reference
-
References
1. Vose J, Armitage J, Weisenburger D. International T-Cell Lymphoma Project. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008; 26:4124–30.2. Briski R, Feldman AL, Bailey NG, Lim MS, Ristow K, Habermann TM, et al. The role of front-line anthracycline-containing chemotherapy regimens in peripheral T-cell lymphomas. Blood Cancer J. 2014; 4:e214.3. Ellin F, Landstrom J, Jerkeman M, Relander T. Real-world data on prognostic factors and treatment in peripheral T-cell lymphomas: a study from the Swedish Lymphoma Registry. Blood. 2014; 124:1570–7.4. Phan A, Veldman R, Lechowicz MJ. T-cell lymphoma epidemiology: the known and unknown. Curr Hematol Malig Rep. 2016; 11:492–503.5. Ma H, Marchi E, O’Connor OA. The peripheral T-cell lymphomas: an unusual path to cure. Lancet Haematol. 2020; 7:e765–71.
Article6. Cirillo M, Craig AFM, Borchmann S, Kurtz DM. Liquid biopsy in lymphoma: molecular methods and clinical applications. Cancer Treat Rev. 2020; 91:102106.7. Dogliotti I, Drandi D, Genuardi E, Ferrero S. New molecular technologies for minimal residual disease evaluation in B-cell lymphoid malignancies. J Clin Med. 2018; 7:288.8. Camus V, Jardin F. Cell-free DNA and the monitoring of lymphoma treatment. Pharmacogenomics. 2019; 20:1271–82.
Article9. Kurtz DM, Scherer F, Jin MC, Soo J, Craig AF, Esfahani MS, et al. Circulating tumor DNA measurements as early outcome predictors in diffuse large B-cell lymphoma. J Clin Oncol. 2018; 36:2845–53.10. Qi F, Cao Z, Chen B, Chai Y, Lin J, Ye J, et al. Liquid biopsy in extranodal NK/T-cell lymphoma: a prospective analysis of cell-free DNA genotyping and monitoring. Blood Adv. 2021; 5:2505–14.
Article11. Miljkovic MD, Melani C, Pittaluga S, Lakhotia R, Lucas N, Jacob A, et al. Next-generation sequencing-based monitoring of circulating tumor DNA reveals clonotypic heterogeneity in untreated PTCL. Blood Adv. 2021; 5:4198–210.12. Zhang W, Wang W, Han X, Gan Y, Qian L, Zhang Y, et al. Circulating tumor DNA by high-throughput sequencing of T cell receptor monitored treatment response and predicted treatment failure in T cell lymphomas. Int J Lab Hematol. 2021; 43:1041–9.
Article13. Sakata-Yanagimoto M, Nakamoto-Matsubara R, Komori D, Nguyen TB, Hattori K, Nanmoku T, et al. Detection of the circulating tumor DNAs in angioimmunoblastic T-cell lymphoma. Ann Hematol. 2017; 96:1471–5.14. Shin SH, Kim YJ, Lee D, Cho D, Ko YH, Cho J, et al. Analysis of circulating tumor DNA by targeted ultra-deep sequencing across various non-Hodgkin lymphoma subtypes. Leuk Lymphoma. 2019; 60:2237–46.15. Hur JY, Kim YJ, Yoon SE, Son DS, Park WY, Kim SJ, et al. Plasma cell-free DNA is a prognostic biomarker for survival in patients with aggressive non-Hodgkin lymphomas. Ann Hematol. 2020; 99:1293–302.16. Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014; 32:3059–68.17. Newman AM, Lovejoy AF, Klass DM, Kurtz DM, Chabon JJ, Scherer F, et al. Integrated digital error suppression for improved detection of circulating tumor DNA. Nat Biotechnol. 2016; 34:547–55.18. McKenna A, Hanna M, Banks E, Sivachenko A, Cibulskis K, Kernytsky A, et al. The Genome Analysis Toolkit: a MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010; 20:1297–303.19. Li H. A statistical framework for SNP calling, mutation discovery, association mapping and population genetical parameter estimation from sequencing data. Bioinformatics. 2011; 27:2987–93.20. Avanzini S, Kurtz DM, Chabon JJ, Moding EJ, Hori SS, Gambhir SS, et al. A mathematical model of ctDNA shedding predicts tumor detection size. Sci Adv. 2020; 6:eabc4308.21. Sakata-Yanagimoto M, Enami T, Yoshida K, Shiraishi Y, Ishii R, Miyake Y, et al. Somatic RHOA mutation in angioimmunoblastic T cell lymphoma. Nat Genet. 2014; 46:171–5.22. Yoo HY, Sung MK, Lee SH, Kim S, Lee H, Park S, et al. A recurrent inactivating mutation in RHOA GTPase in angioimmunoblastic T cell lymphoma. Nat Genet. 2014; 46:371–5.23. Palomero T, Couronne L, Khiabanian H, Kim MY, Ambesi-Impiombato A, Perez-Garcia A, et al. Recurrent mutations in epigenetic regulators, RHOA and FYN kinase in peripheral T cell lymphomas. Nat Genet. 2014; 46:166–70.24. Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016; 127:2375–90.25. Lemonnier F, Safar V, Beldi-Ferchiou A, Cottereau AS, Bachy E, Cartron G, et al. Integrative analysis of a phase 2 trial combining lenalidomide with CHOP in angioimmunoblastic T-cell lymphoma. Blood Adv. 2021; 5:539–48.26. Heavican TB, Bouska A, Yu J, Lone W, Amador C, Gong Q, et al. Genetic drivers of oncogenic pathways in molecular subgroups of peripheral T-cell lymphoma. Blood. 2019; 133:1664–76.27. Ji MM, Huang YH, Huang JY, Wang ZF, Fu D, Liu H, et al. Histone modifier gene mutations in peripheral T-cell lymphoma not otherwise specified. Haematologica. 2018; 103:679–87.28. Xie C, Li X, Zeng H, Qian W. Molecular insights into pathogenesis and targeted therapy of peripheral T cell lymphoma. Exp Hematol Oncol. 2020; 9:30.29. Melchardt T, Hufnagl C, Weinstock DM, Kopp N, Neureiter D, Trankenschuh W, et al. Clonal evolution in relapsed and refractory diffuse large B-cell lymphoma is characterized by high dynamics of subclones. Oncotarget. 2016; 7:51494–502.
Article30. Pon JR, Wong J, Saberi S, Alder O, Moksa M, Grace Cheng SW, et al. MEF2B mutations in non-Hodgkin lymphoma dysregulate cell migration by decreasing MEF2B target gene activation. Nat Commun. 2015; 6:7953.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Application of Circulating Tumor DNA Analysis
- Current Methods of Circulating Tumor Cell Detection
- Circulating Tumor Cells and Extracellular Nucleic Acids in Breast Cancer
- Circulating Cell-free Tumor Nucleic Acids in Gastric Cancer
- Circulating Lymphoma Cells in the Peripheral Blood from 4 Cases of Mantle and T Cell Types of Non-Hodgkin's Lymphoma: Light and Electron Microscopic Morphology
