Open Reduction and Primary Ligament Suture for Irreducible Knee Dislocation: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Daejeon Sun Hospital, Daejeon, Korea
- KMID: 2536678
- DOI: http://doi.org/10.5763/kjsm.2022.40.4.263
Abstract
- Irreducible knee dislocation among acute knee dislocations is very rare. If reduction and treatment are not performed early, serious complications such as skin necrosis, vascular and nerve injury, compartment syndrome, and instability can occur. So far, treatment options, such as two-staged operation with early open reduction and delayed ligaments reconstruction or repair, one-staged arthroscopic reduction without ligaments reconstruction or repair, one-staged operation with open reduction and ligaments reconstruction have been reported for the irreducible knee dislocation. In this case, the authors have found satisfactory results following one-staged operation with open reduction and primary ligament suture after diagnosing the exact injury site using magnetic resonance imaging preoperatively.
Keyword
Figure
-
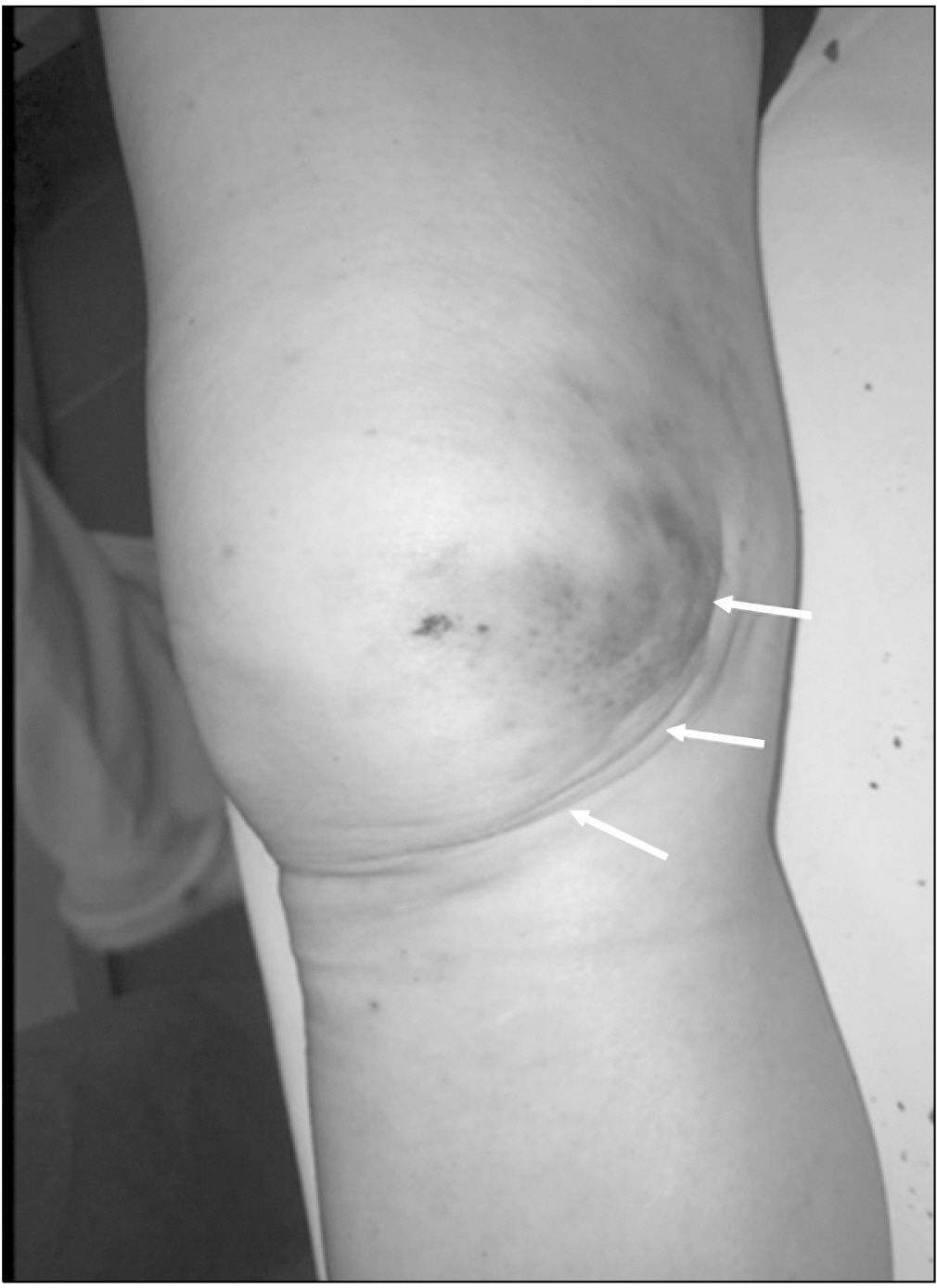
Fig. 1 Preoperative clinical photographs. Ecchymosis and skin dimple sign over the medial joint line (white arrows).
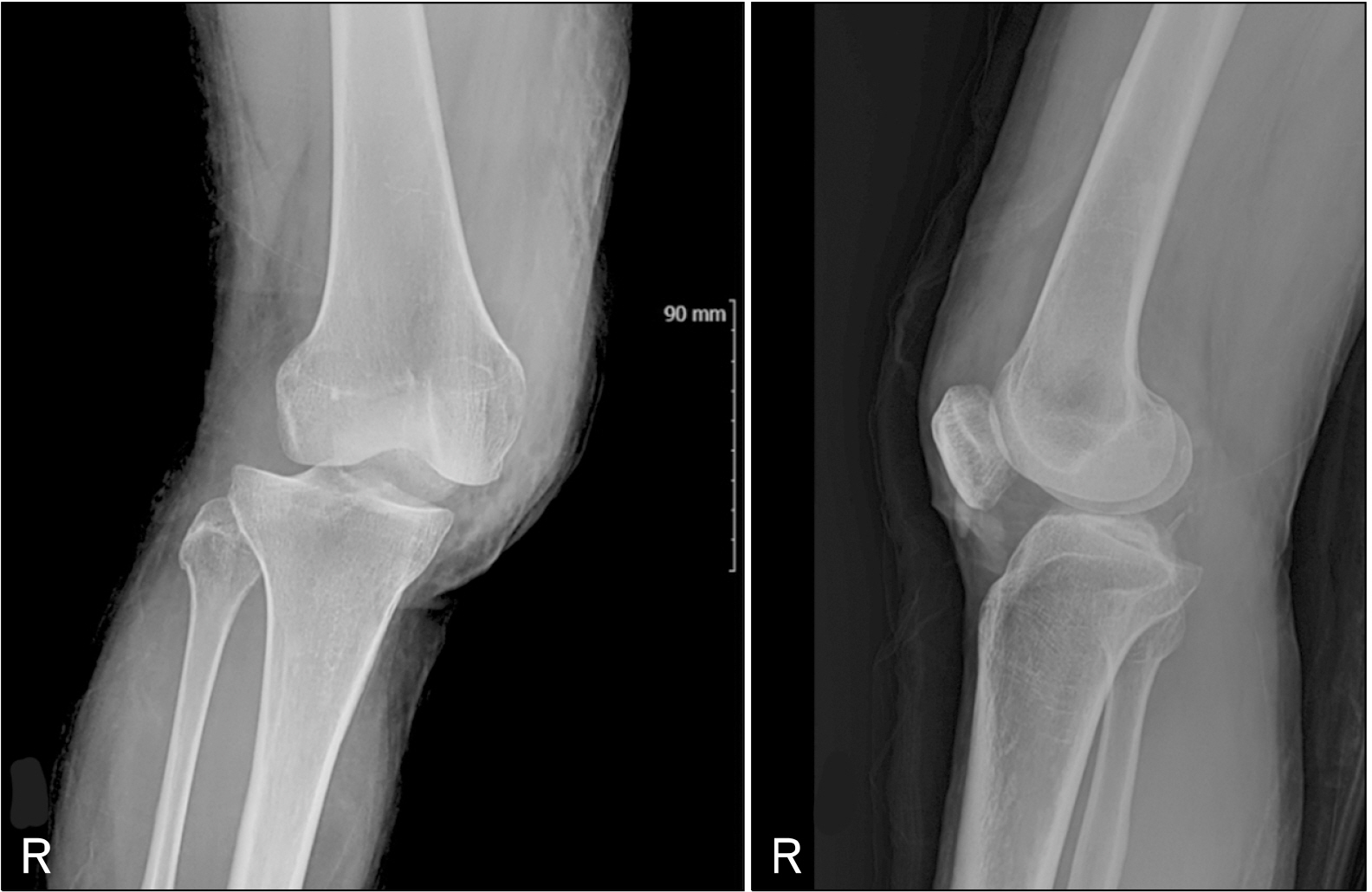
Fig. 2 The radiographs show posterolateral dislocation of the right knee joint.
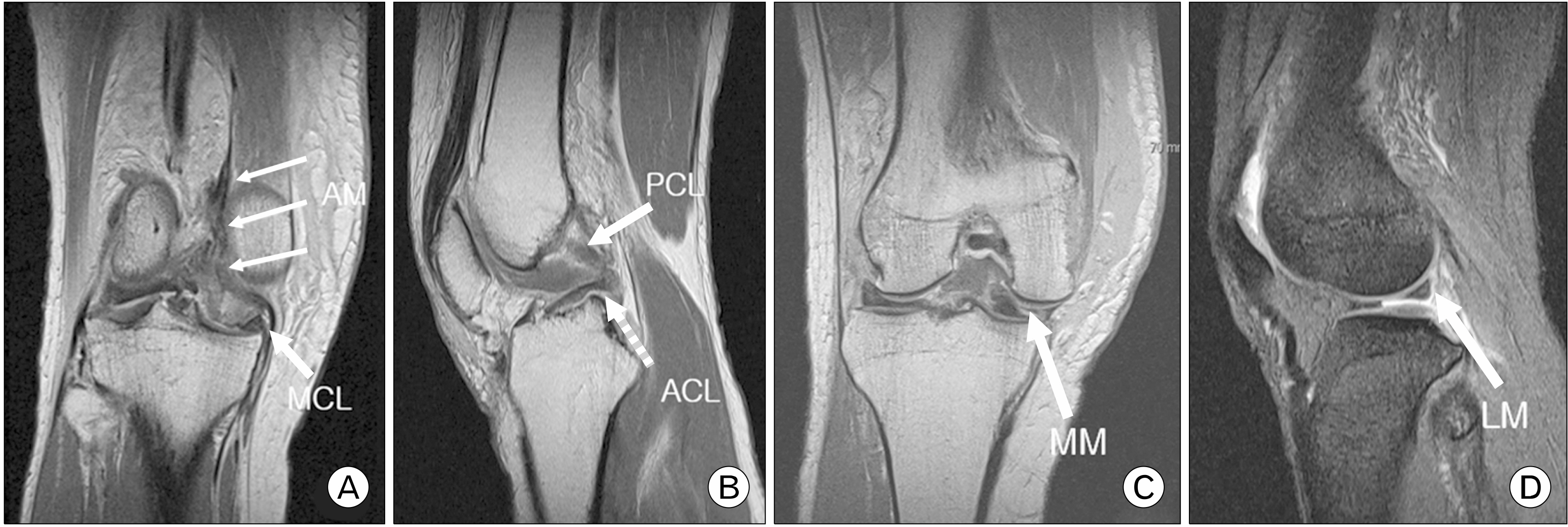
Fig. 3 Coronal T2-weighted magnetic resonance image (MRI) scan taken before reduction, showing adductor magnus (AM) tendon, medial collateral ligament (MCL), and medial retinaculum interpositioned into the intercondyle notch (thin arrows) (A) and coronal T2-weighted MRI of a peripheral tear of the medial meniscus (MM, arrow) anterior horn (C). Sagittal T2-weighted MRI scan taken before reduction, showing ruptured tibial attachment site of posterior cruciate ligament (PCL, arrow) and femoral attachment site of the anterior cruciate ligament (ACL, dotted arrow) (B) and sagittal T1-weighted MRI showing a longitudinal tear of the lateral meniscus (LM, arrow) posterior horn (D).
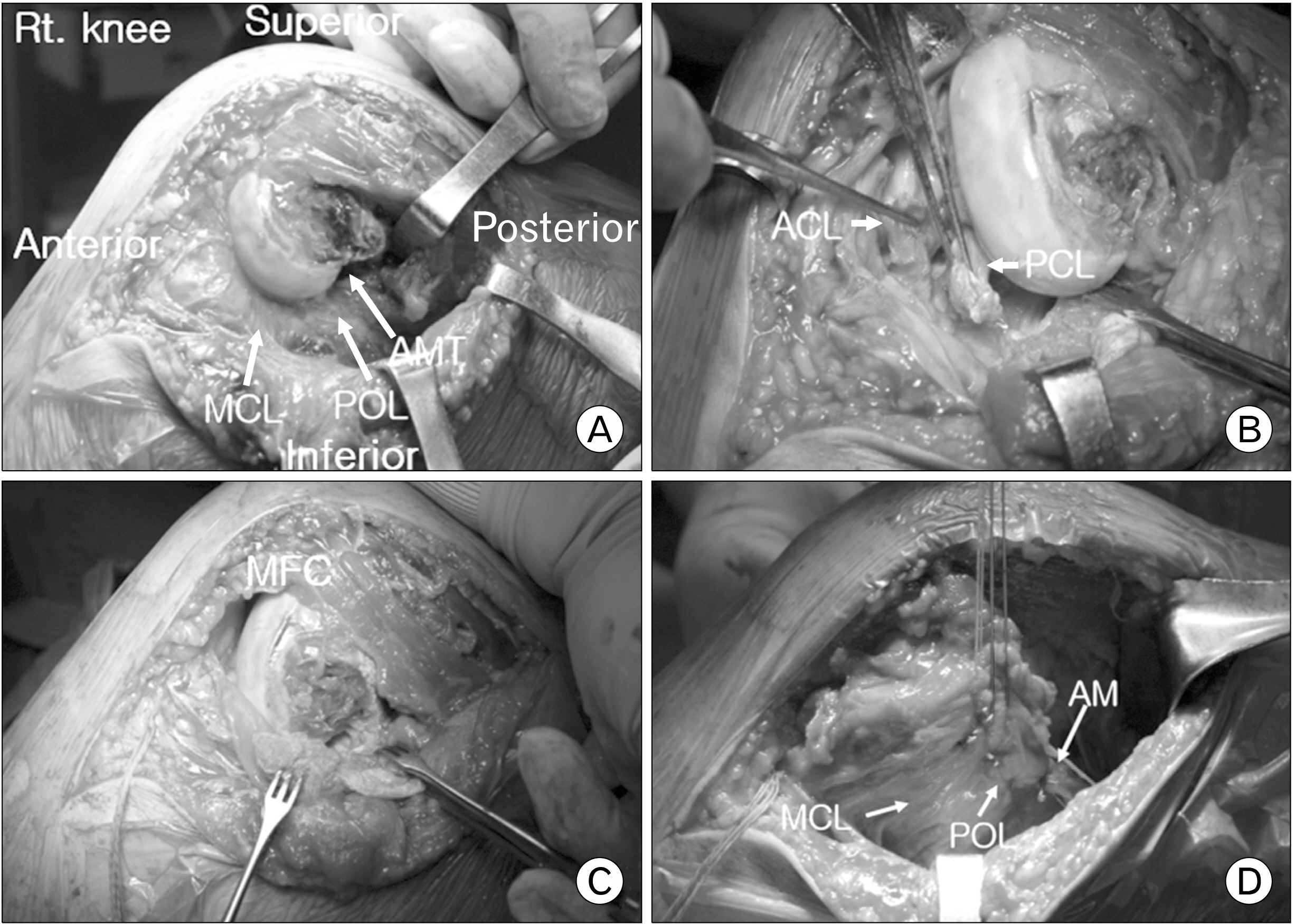
Fig. 4 Intraoperative gross images. There was no reduction achieved because of the tight medial patella retinaculum and adductor magnus tendon (AMT) interpositioned into the intercondyle notch (A). The anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) were ruptured (B). Meniscus, ACL, PCL were repaired and successful reduction was achieved (C). The medial collateral ligament (MCL), posterior oblique ligament (POL), and adductor magnus (AM) were repaired (D). MFC: medial femur condyle.

Fig. 5 At the 13-month follow-up, the patient regained the same range of motion as the opposite side.
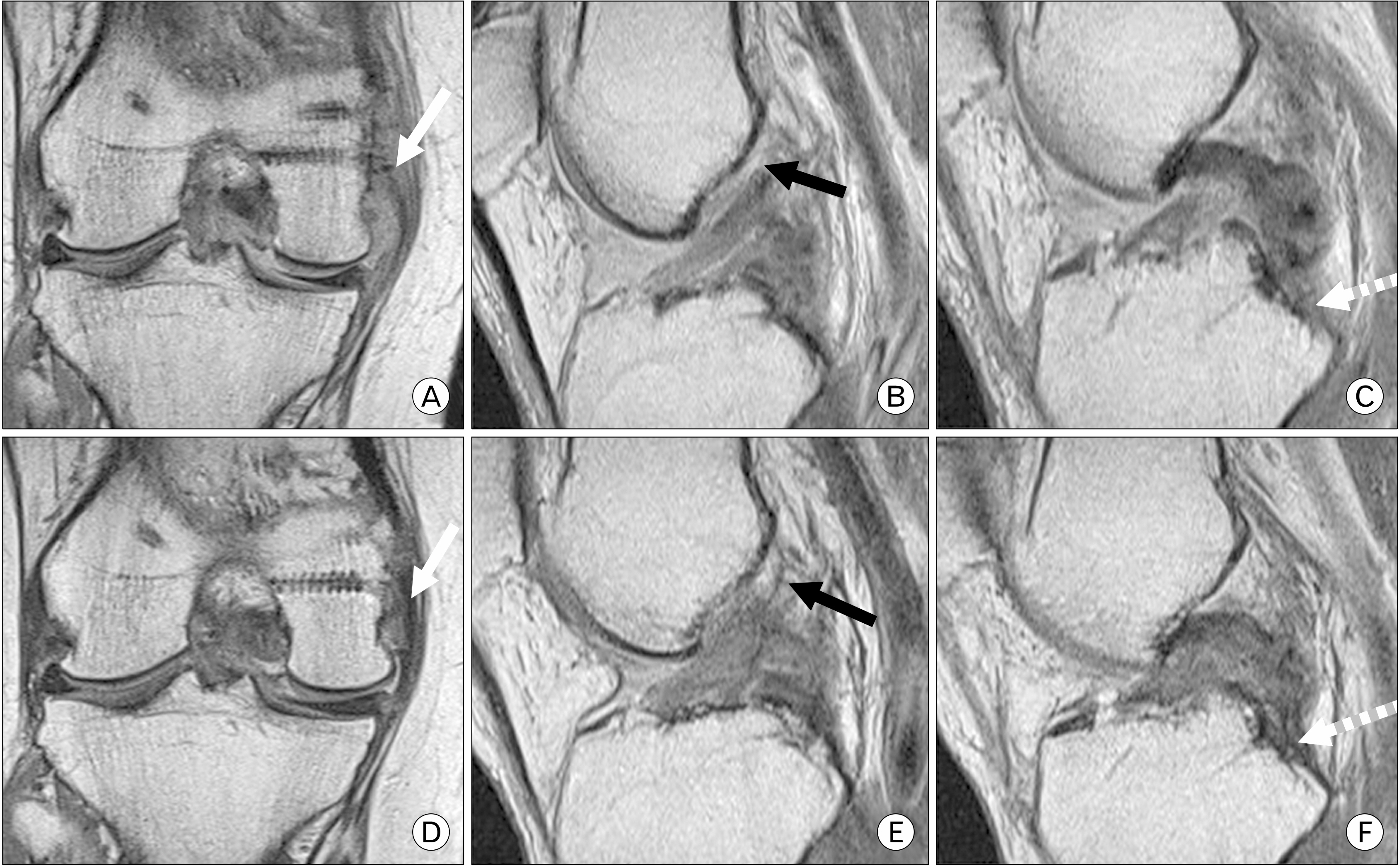
Fig. 6 After 10 weeks (A–C) and 13 months (D–F) postoperatively, coronal T2-weighted magnetic resonance image (MRI) showed that the medial collateral ligament was completely healed (white arrows) (A, D), and sagittal T2-weighted MRI showed that the anterior (black arrows) and posterior cruciate ligaments (white dotted arrows) were incompletely healed (B, C, E, F).
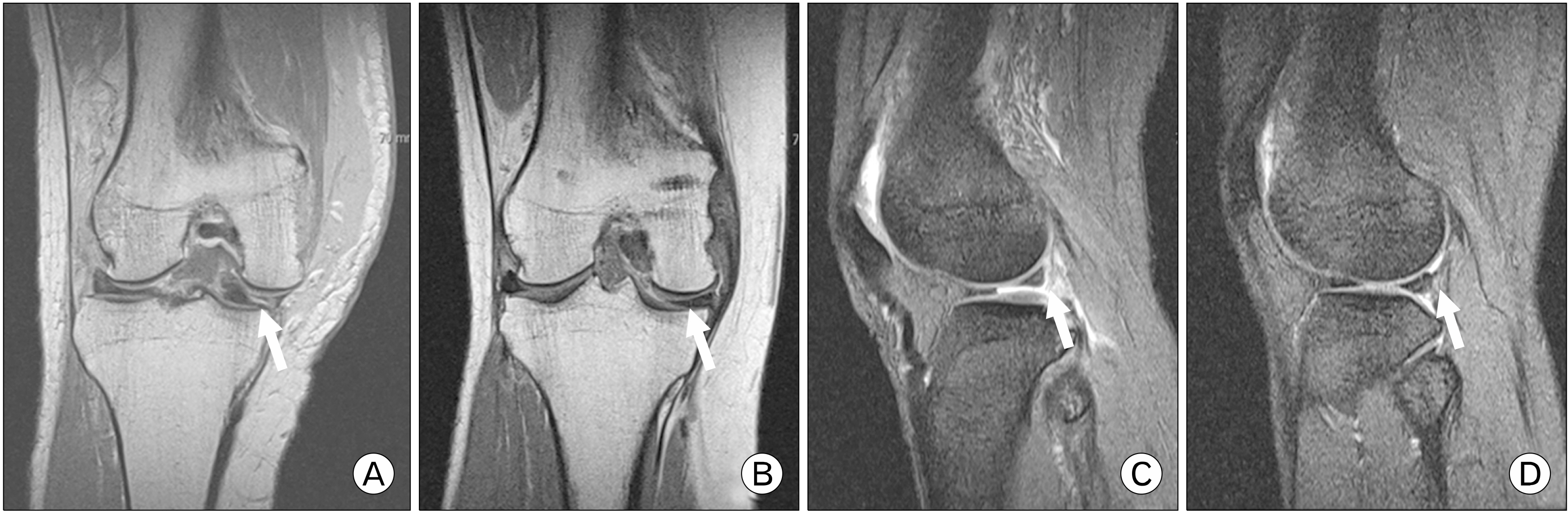
Fig. 7 (A) Preoperative coronal magnetic resonance imaging (MRI). The white arrow shows a medial meniscus anterior horn peripheral tear. (C) Preoperative sagittal MRI. The white arrow shows a lateral meniscus posterior horn longitudinal tear. (B, D) After 13 months postoperatively, complete healing was noted at the previous tear of medial meniscus and lateral meniscus (arrows).
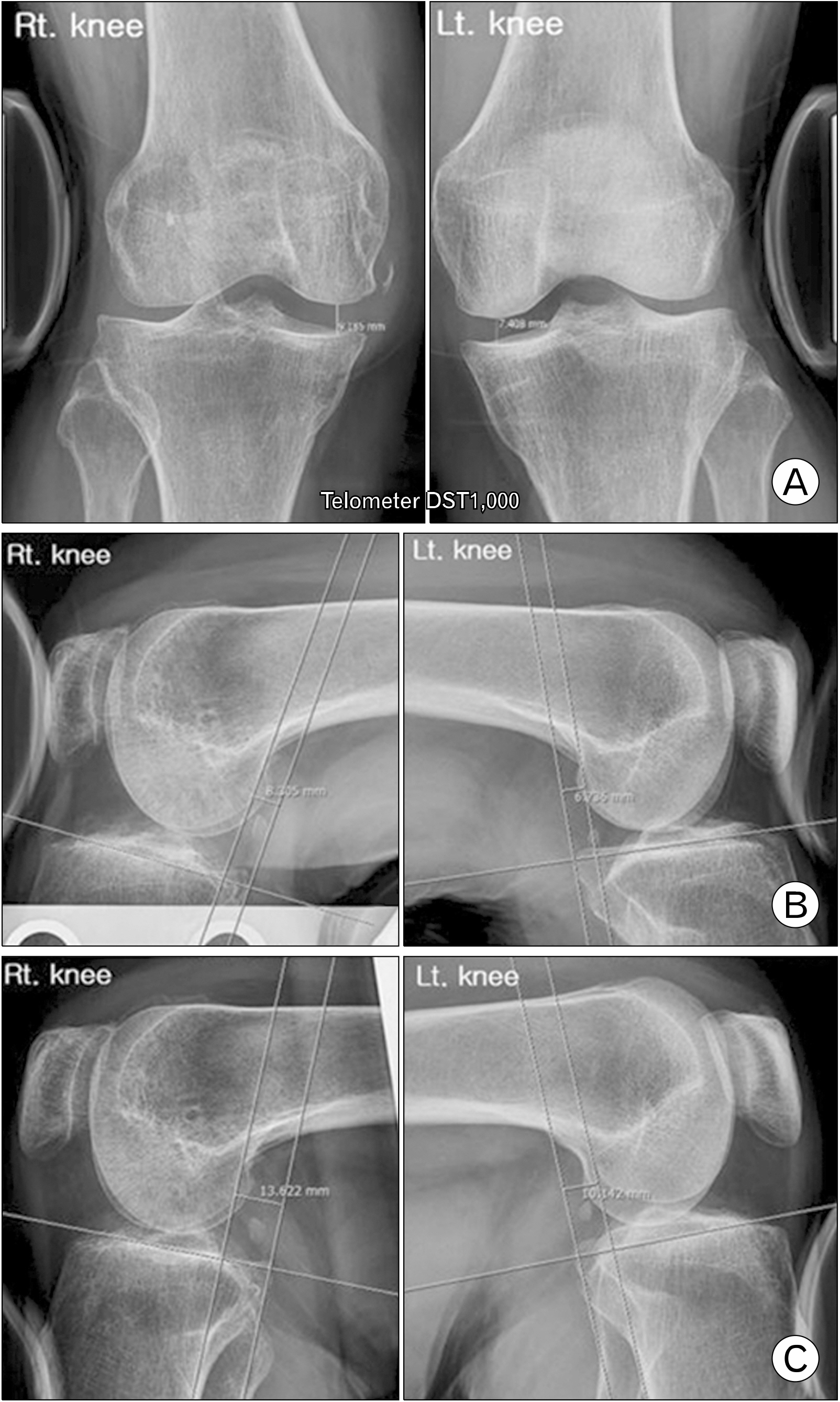
Fig. 8 Using Telometer DST1000 (Daiseung Medics Corp., Seoul, Korea) in the valgus stress test, medial side of the injured right knee was 1.8 mm (right, 9.2 mm; left, 7.4 mm) wider than the left knee (A), in the anterior drawer test, the injured right knee has 1.6 mm (right, 8.3 mm; left, 6.7 mm) more anterior displacement than the left knee (B), and in the posterior drawer test, the injured right knee has 3.5 mm (right, 13.6 mm; left, 10.1 mm) more posterior displacement than the left knee (C).
Reference
-
1. Capito N, Gregory MH, Volgas D, Sherman SL. 2013; Evaluation and management of an irreducible posterolateral knee dislocation. J Knee Surg. 26 Suppl 1:S136–41. DOI: 10.1055/s-0033-1341577. PMID: 23512541.
Article2. Lee HS, Lee SH, Lee SW. 2020; Closed reduction of irreducible posterolateral rotatory knee dislocation. J Korean Orthop Assoc. 55:95–100. DOI: 10.4055/jkoa.2020.55.1.95.
Article3. Koh HS, Kim HS, Lee HS. 2009; Irreducible Posterolateral Dislocation of the Knee Joint with Lateral Dislocation of the Patella: a report of two cases. Knee Surg Relat Res. 21:51–6.4. Kim HS, Park SR, Kang JS, Lee WH, Kim KW. 2001; A rare case of irreducible knee dislocation: vastus medialis obliqus-buttonholing of medial femoral condyle: a case report. J Korean Arthrosc Soc. 5:41–4.5. Malik SS, MacDonald PB. 2020; The irreducible knee dislocation. J Knee Surg. 33:328–34. DOI: 10.1055/s-0039-1698749. PMID: 31756734.
Article6. Jeong JY. 2009; Arthroscopic reduction of irreducible knee dislocation: a case report. J Korean Arthrosc Soc. 13:161–4.7. Lim JC, Kim SH, Seo SH, Kim YM. 2019; A Study of applied pressure according to knee variable during Lachman test for anterior cruciate ligament using Telos device. J Korean Radiology Soc. 13:391–8.8. Huang FS, Simonian PT, Chansky HA. 2000; Irreducible posterolateral dislocation of the knee. Arthroscopy. 16:323–7. DOI: 10.1016/S0749-8063(00)90057-4. PMID: 10750013.
Article9. Solarino G, Notarnicola A, Maccagnano G, Piazzolla A, Moretti B. 2015; Irreducible posterolateral dislocation of the knee: a case report. Joints. 3:91–6. DOI: 10.11138/jts/2015.3.2.091. PMID: 26605258. PMCID: PMC4634811.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Reduction of Irreducible Posterolateral Knee Dislocation with Interposition of the Vastus Medialis: A Case Report
- Closed Reduction of Irreducible Posterolateral Rotatory Knee Dislocation
- Irreducible Posterolateral Dislocation of the Knee Joint with Lateral Dislocation of the Patella: A Report of Two Cases
- Irreducible Dislocation of the Interphalangeal Joint of the Thumb: A Case Report
- Irreducible Knee Dislocation with Vastus Medialis Muscle Interposition
