Endoscopic Debridement of Post-Radiation Nasopharyngeal Necrosis: The Effects of Resurfacing With a Vascularized Flap
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2536534
- DOI: http://doi.org/10.21053/ceo.2022.00465
Abstract
Objectives
. Post-radiation nasopharyngeal necrosis (PRNN) is a serious complication that severely impacts the quality of life and survival of nasopharyngeal carcinoma patients. Endoscopic debridement is considered the first-line treatment for PRNN. This study aimed to analyze clinical outcomes, focusing on the mucosal resurfacing status and the effectiveness of salvage operations.
Methods
. Twenty-seven patients who underwent endoscopic debridement were retrospectively analyzed. The patients were divided into two groups according to the initial surgical modality: debridement with a nasoseptal flap (NSF; n=21) and debridement only (no NSF; n=6). Clinical features, postoperative mucosal status, internal carotid artery (ICA) rupture, survival, and final mucosal status were evaluated. The NSF group was categorized according to flap viability to analyze risk factors for flap failure.
Results
. Regardless of the initial modality, most patients experienced symptom improvement (96.0% for headache and 100% for foul odor); however, complete cranial nerve palsy did not improve in any patients. In the NSF group, complete healing was observed in 66.7%, while all patients in the no-NSF group underwent salvage surgery because none maintained complete healing. In the NSF group, 19.0% of patients required salvage surgery. After the last operation, favorable symptom improvement was noted (100% for headache and 90.0% for foul odor), and 77.8% had completely healed mucosa, whereas only 14.8% and 7.4% had partial healing and persistent necrotic mucosal status. The necrotic or uncovered NSF subgroup showed statistically non-significant tendencies for old age, advanced necrosis stage, advanced T stage, ICA involvement, high frequency and dose of radiation therapy, diabetes mellitus, and underlying comorbidities. Two ICA ruptures and three deaths occurred.
Conclusion
. Resurfacing the nasopharynx with NSF after endoscopic debridement showed better outcomes than debridement only for PRNN treatment. Despite initial NSF failure, additional resurfacing reconstructive surgery offers advantages in symptom mitigation, quality of life, and survival.
Keyword
Figure
-
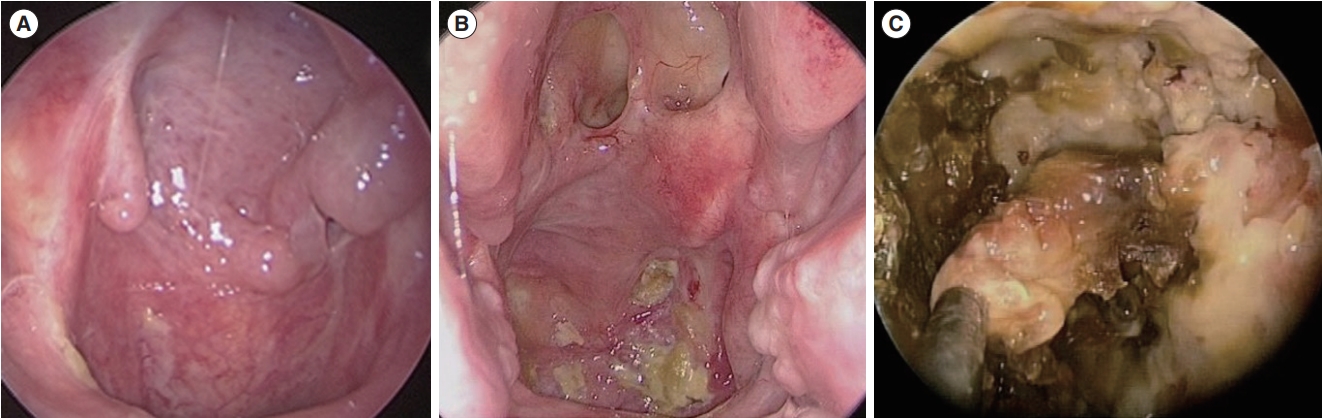
Fig. 1. Postoperative mucosal status. (A) Complete healing. (B) Partial healing. (C) Persistent necrosis.

Fig. 2. Stages of necrosis. (A) Early: mucosal necrosis alone. (B) Middle: necrosis involving mucosa, muscle, and tendon. (C) Late: osteoradionecrosis.
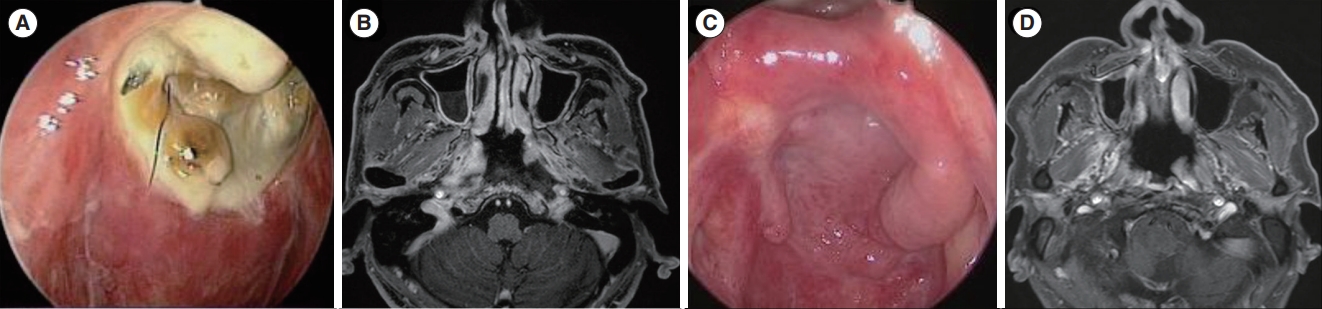
Fig. 3. A representative example of debridement with a nasoseptal flap (NSF) as the initial operation (case 14). (A) Preoperative endoscopic image of radionecrosis. (B) Preoperative magnetic resonance imaging (MRI) shows extensive necrotic lesions on both sides of the nasopharynx, extending to the left internal carotid artery and eroding the clivus. (C) Seventeen months after the operation, a viable NSF with complete mucosal healing was achieved. (D) MRI shows fully viable nasopharyngeal tissue without any remnant necrotic tissue.

Fig. 4. A case of a salvage operation with an anterolateral thigh free flap (ALTFF) (case 4). (A) Preoperative endoscopic image shows extensive necrosis throughout the entire nasopharynx, nearly extending to the superior margin of the oropharyngeal wall. (B) Intraoperative endoscopic image after debridement; resurfacing with a flap was not performed. (C) A postoperative examination shows extensive necrotic tissue again. (D) Four months after a salvage operation with repetitive debridement and ALTFF; complete healing was achieved.
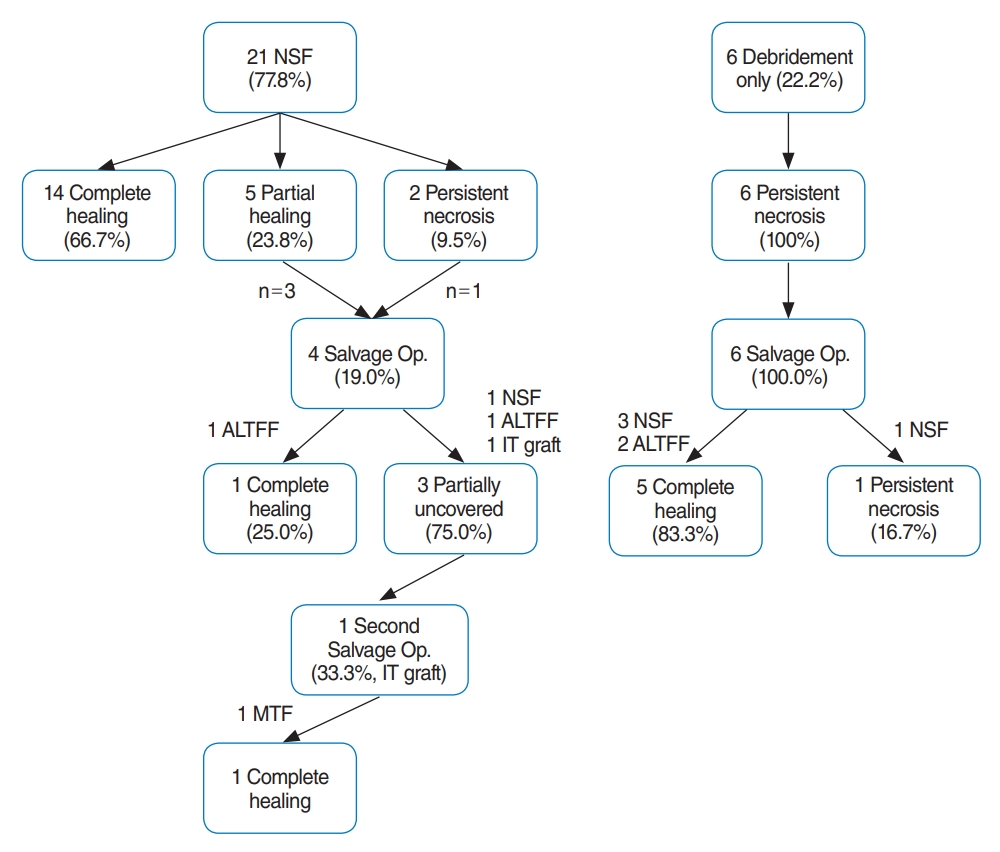
Fig. 5. Flowchart and treatment outcomes. NSF, nasoseptal flap; Op, operation; ALTFF, anterolateral thigh free flap; IT, inferior turbinate; MTF, middle turbinate flap.
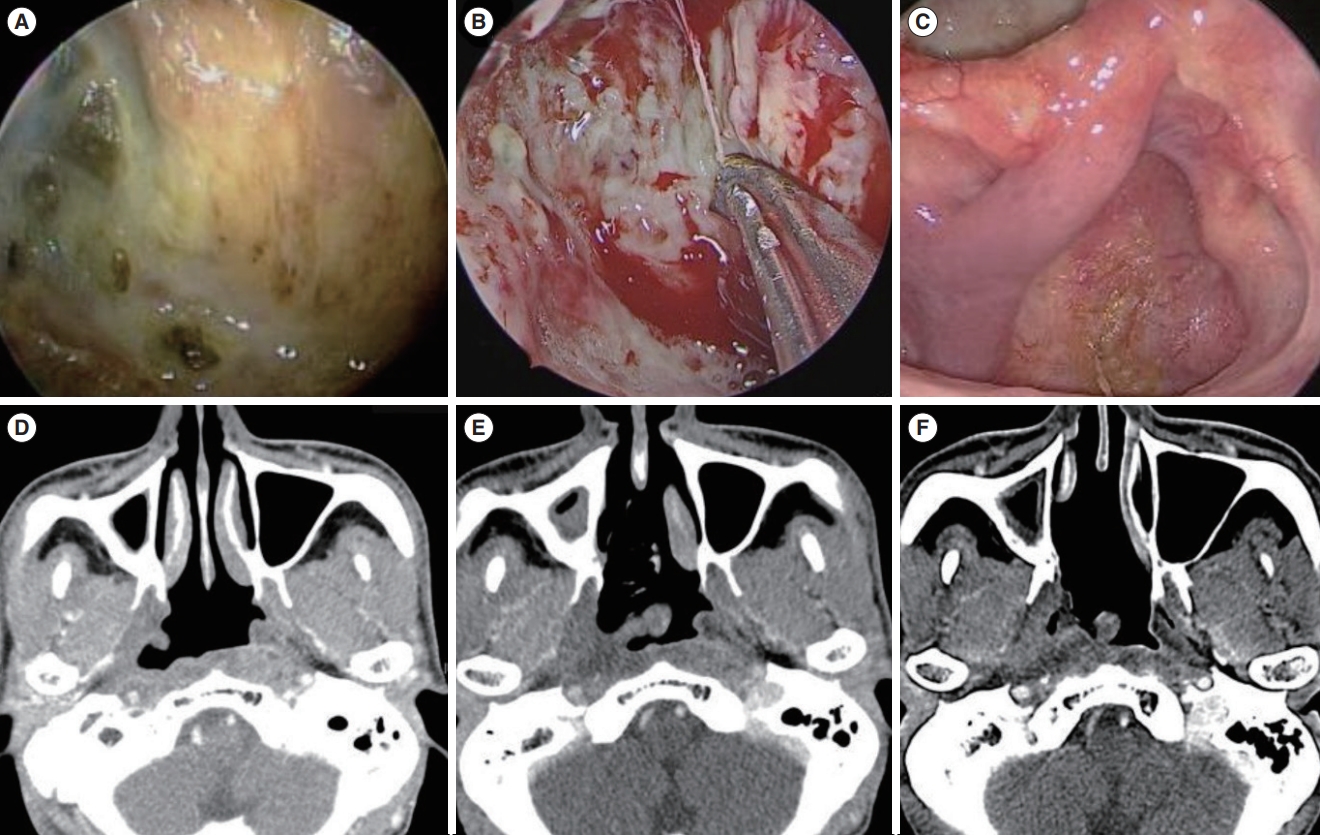
Fig. 6. An example of persistent necrosis under completely healed mucosa in a patient who was free of symptoms (case 8). (A) Preoperative endoscopic image of radionecrosis. (B) Intraoperative endoscopic image after the debridement of necrotic tissue. (C) Fifty-two months after debridement with a nasoseptal flap (NSF); completely healed mucosa with a viable NSF is observed. (D) Preoperative computed tomography (CT) scan shows radionecrosis involving the nasopharyngeal deep tissue near the right internal carotid artery (ICA). (E) CT scan 4 months postoperatively. (F) CT scan 52 months postoperatively; remaining necrotic tissue is seen near the ICA, without any progression compared to the preoperative imaging.
Reference
-
1. Yu MC, Yuan JM. Epidemiology of nasopharyngeal carcinoma. Semin Cancer Biol. 2002; Dec. 12(6):421–9.
Article2. Chua ML, Wee JT, Hui EP, Chan AT. Nasopharyngeal carcinoma. Lancet. 2016; Mar. 387(10022):1012–24.
Article3. Ma J, Mai HQ, Hong MH, Min HQ, Mao ZD, Cui NJ, et al. Results of a prospective randomized trial comparing neoadjuvant chemotherapy plus radiotherapy with radiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma. J Clin Oncol. 2001; Mar. 19(5):1350–7.
Article4. Zhang W, Dou H, Lam C, Liu J, Zhou J, Liu Y, et al. Concurrent chemoradiotherapy with or without adjuvant chemotherapy in intermediate and locoregionally advanced nasopharyngeal carcinoma. Tumour Biol. 2013; Jun. 34(3):1729–36.
Article5. Zhang MX, Li J, Shen GP, Zou X, Xu JJ, Jiang R, et al. Intensity-modulated radiotherapy prolongs the survival of patients with nasopharyngeal carcinoma compared with conventional two-dimensional radiotherapy: a 10-year experience with a large cohort and long follow-up. Eur J Cancer. 2015; Nov. 51(17):2587–95.
Article6. Mao YP, Tang LL, Chen L, Sun Y, Qi ZY, Zhou GQ, et al. Prognostic factors and failure patterns in non-metastatic nasopharyngeal carcinoma after intensity-modulated radiotherapy. Chin J Cancer. 2016; Dec. 35(1):103.
Article7. Huang XM, Zheng YQ, Zhang XM, Mai HQ, Zeng L, Liu X, et al. Diagnosis and management of skull base osteoradionecrosis after radiotherapy for nasopharyngeal carcinoma. Laryngoscope. 2006; Sep. 116(9):1626–31.
Article8. Hua YJ, Chen MY, Qian CN, Hong MH, Zhao C, Guo L, et al. Postradiation nasopharyngeal necrosis in the patients with nasopharyngeal carcinoma. Head Neck. 2009; Jun. 31(6):807–12.
Article9. Yu YH, Xia WX, Shi JL, Ma WJ, Li Y, Ye YF, et al. A model to predict the risk of lethal nasopharyngeal necrosis after re-irradiation with intensity-modulated radiotherapy in nasopharyngeal carcinoma patients. Chin J Cancer. 2016; Jun. 35(1):59.
Article10. Yang Q, Zou X, You R, Liu YP, Han Y, Zhang YN, et al. Proposal for a new risk classification system for nasopharyngeal carcinoma patients with post-radiation nasopharyngeal necrosis. Oral Oncol. 2017; Apr. 67:83–8.
Article11. Chen MY, Mai HQ, Sun R, Guo X, Zhao C, Hong MH, et al. Clinical findings and imaging features of 67 nasopharyngeal carcinoma patients with postradiation nasopharyngeal necrosis. Chin J Cancer. 2013; Oct. 32(10):533–8.
Article12. Ryu G, So YK, Seo MY, Park W, Kim HY, Dhong HJ, et al. Using the nasoseptal flap for reconstruction after endoscopic debridement of radionecrosis in nasopharyngeal carcinoma. Am J Rhinol Allergy. 2018; Jan. 32(1):61–5.
Article13. Chen KC, Yen TT, Hsieh YL, Chen HC, Jiang RS, Chen WH, et al. Postirradiated carotid blowout syndrome in patients with nasopharyngeal carcinoma: a case-control study. Head Neck. 2015; Jun. 37(6):794–9.
Article14. Chen MY, Wang SL, Zhu YL, Shen GP, Qiu F, Luo DH, et al. Use of a posterior pedicle nasal septum and floor mucoperiosteum flap to resurface the nasopharynx after endoscopic nasopharyngectomy for recurrent nasopharyngeal carcinoma. Head Neck. 2012; Oct. 34(10):1383–8.
Article15. Zou X, Wang SL, Liu YP, Liu YL, Zou RH, Zhang YN, et al. A curativeintent endoscopic surgery for postradiation nasopharyngeal necrosis in patients with nasopharyngeal carcinoma. Cancer Commun (Lond). 2018; Dec. 38(1):74.
Article16. Cho SW, Han SY, Song Y, Kim JW, Kim HJ, Kim DY, et al. Aggressive treatment including endonasal surgical sequestrectomy with vascularized nasoseptal flap can improve outcomes of skull base osteoradionecrosis. J Neurol Surg B Skull Base. 2021; Jan. 83(Suppl 2):e15–23.
Article17. Hua YJ, Chen MY, Hong MH, Zhao C, Guo L, Han F, et al. Short-term efficacy of endoscopy-guided debridement on radiation-related nasopharyngeal necrosis in 20 nasopharyngeal carcinoma patients after radiotherapy. Ai Zheng. 2008; Jul. 27(7):729–33.18. Marx RE. Osteoradionecrosis: a new concept of its pathophysiology. J Oral Maxillofac Surg. 1983; May. 41(5):283–8.
Article19. Lou PJ, Chen WP, Tai CC. Delayed irradiation effects on nasal epithelium in patients with nasopharyngeal carcinoma: an ultrastructural study. Ann Otol Rhinol Laryngol. 1999; May. 108(5):474–80.
Article20. Wei WI, Sham JS. Nasopharyngeal carcinoma. Lancet. 2005; Jun. 365(9476):2041–54.
Article21. Adel M, Chang KP. Using a nasoseptal flap for the reconstruction of osteoradionecrosis in nasopharyngeal carcinoma: a case report. J Otolaryngol Head Neck Surg. 2016; Apr. 45:27.
Article22. Khoo ML, Soo KC, Gullane PJ, Neligan PC, Hong SW, Lee JC, et al. Resurfacing of the nasopharynx after nasopharyngectomy using a free radial forearm flap. Head Neck. 2001; Oct. 23(10):916–22.
Article23. Baek CH, Park W, Choi N, Gu S, Sohn I, Chung MK. Free flap outcome of salvage surgery compared to primary surgery for head and neck defects: a propensity score analysis. Oral Oncol. 2016; Nov. 62:85–9.
Article24. Gordin EA, Ducic Y. Microvascular free tissue reconstruction in the patient with multiple courses of radiation. Laryngoscope. 2014; Oct. 124(10):2252–6.
Article25. Choi NY, Kim HJ, Baek CH. Surgical management of extensive osteoradionecrosis in nasopharyngeal carcinoma patients with the maxillary swing approach and free muscular flaps. Clin Otolaryngol. 2017; Oct. 42(5):1100–4.
Article26. Vlantis AC, Wong EW, Chiu TW, Chan JY. Vastus lateralis muscle free flap for skull base osteoradionecrosis in nasopharyngeal carcinoma. J Neurol Surg B Skull Base. 2018; Aug. 79(4):349–52.
Article27. Cornes PG, Cox HJ, Rhys-Evans PR, Breach NM, Henk JM. Salvage treatment for inoperable neck nodes in head and neck cancer using combined iridium-192 brachytherapy and surgical reconstruction. Br J Surg. 1996; Nov. 83(11):1620–2.
Article28. Hao SP, Chen HC, Wei FC, Chen CY, Yeh AR, Su JL. Systematic management of osteoradionecrosis in the head and neck. Laryngoscope. 1999; Aug. 109(8):1324–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Free Flap Reconstruction after Endoscopic Debridemnt for Recalcitrant Nasopharyngeal Osteoradionecrosis Without Facial Incision
- Endoscopic Necrosectomy for Walled-Off Pancreatic Necrosis
- Combined Facial Rejuvenation Using Endoscopic Face Lift and Laser Resurfacing
- Delayed Radiation Necrosis in Both Temporal Lobes: A Case Report
- Two Cases of Recurrent Nasopharyngeal Stricture Treated with Nasoseptal Flap
