Anesth Pain Med.
2022 Oct;17(4):445-453. 10.17085/apm.22157.
A randomized double-blind controlled study comparing erector spinae plane block and thoracic paravertebral block for postoperative analgesia after breast surgery
- Affiliations
-
- 1Department of Anesthesiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
- 2Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
- KMID: 2535345
- DOI: http://doi.org/10.17085/apm.22157
Abstract
- Background
Thoracic paravertebral block (PVB) is an effective regional block for pain control after breast surgery. However, accidentally puncturing adjacent vital structures may cause undesirable complications. Erector spinae plane block (ESPB) has been considered a safer proxy of PVB for beginners. This study aimed to evaluate the analgesic effects of ultrasound-guidance PVB and ESPB after breast surgery.
Methods
This randomized control trial was conducted in patients who underwent mastectomy. Forty-four females were randomly allocated into PVB group or ESPB group. All patients received a block with 20 ml of 0.5% levobupivacaine before general anesthesia. The primary outcome was the 24-h postoperative morphine requirements. The other outcomes of interest were postoperative pain scores, time to first analgesic request, dermatome of sensory blockade, block-related complications, and opioid adverse events.
Results
The 24-h morphine requirements were significantly lower in PVB compared to the ESPB group (3.5 ± 3.3 vs. 8.6 ± 3.8 mg, P < 0.001). The overall pain scores were also lower in the PVB group (P < 0.001). Only 14 patients in the PVB group requested additional morphine, whereas all patients in the ESPB group requested it (P = 0.004). The dermatome of sensory blockade was wider in the PVB group (7 vs. 4 levels, P = 0.019). No serious complications occurred in either group.
Conclusions
Compared to ESPB, PVB provided lower postoperative opioid requirements, lower pain scores, and wider sensory blockade after mastectomy.
Figure
-

Fig. 1. Ultrasound images of PVB (A) and ESPB (B). PVB: thoracic paravertebral block, ESPB: erector spinae plane block, ESM: erector spinae muscle, IIM: internal intercostal membrane, PVS: paravertebral space (a wedge shape), TP: transverse process, white dash-line represented needle trajectory.
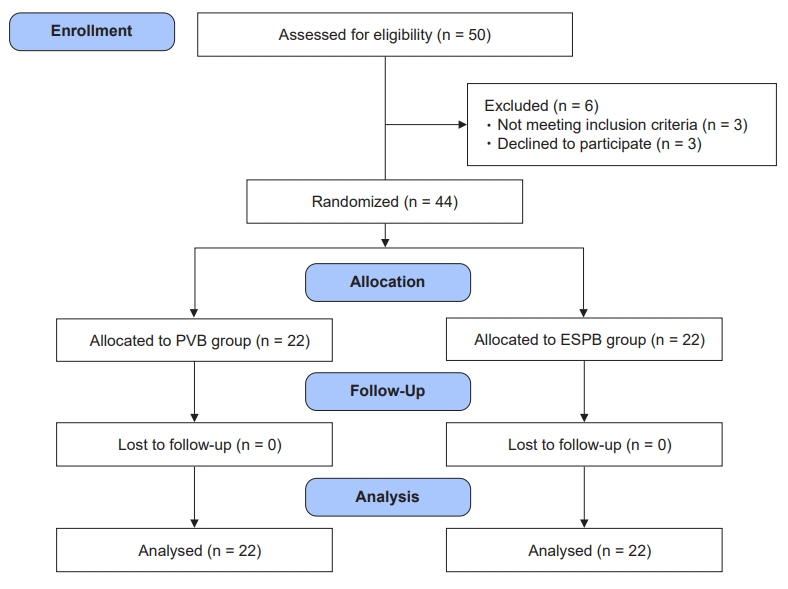
Fig. 2. CONSORT flow diagram for the study. CONSORT: Consolidated Standards for Reporting of Trials, PVB: thoracic paravertebral block, ESPB: erector spinae plane block.

Fig. 3. Dermatome of sensory blockade following PVB and ESPB. PVB: thoracic paravertebral block, ESPB: erector spinae plane block, T: thoracic level.
Reference
-
1. Ghoncheh M, Pournamdar Z, Salehiniya H. Incidence and mortality and epidemiology of breast cancer in the world. Asian Pac J Cancer Prev. 2016; 17(S3):43–6.
Article2. Kulkarni AR, Pusic AL, Hamill JB, Kim HM, Qi J, Wilkins EG, et al. Factors associated with acute postoperative pain following breast reconstruction. JPRAS Open 2017; 11: 1-13. Erratum in: JPRAS Open. 2021; 30:170–1.3. Gärtner R, Jensen MB, Nielsen J, Ewertz M, Kroman N, Kehlet H. Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA 2009; 302: 1985-92. Erratum in: JAMA. 2012; 308:1973.4. Thapa P, Euasobhon P. Chronic postsurgical pain: current evidence for prevention and management. Korean J Pain. 2018; 31:155–73.
Article5. Soni S, Soni A, Bapugol M, Mohammed S, Karnawat R, Tulsiani KL. Comparision of thoracic epidural block vs paravertebral block in patients under going breast surgery. IJCA. 2015; 2:48–56.6. Aoyama Y, Sakura S, Tsuchiya R, Wittayapairoj A, Saito Y. Erector spinae plane block and paravertebral block for breast surgery: a retrospective propensity-matched noninferiority trial. J Pain Res. 2020; 13:2367–76.7. Gürkan Y, Aksu C, Kuş A, Yörükoğlu UH, Kılıç CT. Ultrasound guided erector spinae plane block reduces postoperative opioid consumption following breast surgery: a randomized controlled study. J Clin Anesth. 2018; 50:65–8.
Article8. Singh S, Kumar G. Ultrasound-guided erector spinae plane block for postoperative analgesia in modified radical mastectomy: a randomised control study. Indian J Anaesth. 2019; 63:200–4.
Article9. El Ghamry MR, Amer AF. Role of erector spinae plane block versus paravertebral block in pain control after modified radical mastectomy. A prospective randomised trial. Indian J Anaesth. 2019; 63:1008–14.
Article10. Gürkan Y, Aksu C, Kuş A, Yörükoğlu UH. Erector spinae plane block and thoracic paravertebral block for breast surgery compared to IV-morphine: a randomized controlled trial. J Clin Anesth. 2020; 59:84–8.
Article11. Moustafa MA, Alabd AS, Ahmed AMM, Deghidy EA. Erector spinae versus paravertebral plane blocks in modified radical mastectomy: randomised comparative study of the technique success rate among novice anaesthesiologists. Indian J Anaesth. 2020; 64:49–54.
Article12. Swisher MW, Wallace AM, Sztain JF, Said ET, Khatibi B, Abanobi M, et al. Erector spinae plane versus paravertebral nerve blocks for postoperative analgesia after breast surgery: a randomized clinical trial. Reg Anesth Pain Med. 2020; 45:260–6.
Article13. Shibata Y, Nishiwaki K. Ultrasound-guided intercostal approach to thoracic paravertebral block. Anesth Analg. 2009; 109:996–7.
Article14. Sarhadi NS, Shaw Dunn J, Lee FD, Soutar DS. An anatomical study of the nerve supply of the breast, including the nipple and areola. Br J Plast Surg. 1996; 49:156–64.
Article15. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016; 41:621–7.16. Ivanusic J, Konishi Y, Barrington MJ. A cadaveric study investigating the mechanism of action of erector spinae blockade. Reg Anesth Pain Med. 2018; 43:567–71.
Article17. Yang HM, Choi YJ, Kwon HJ, O J, Cho TH, Kim SH. Comparison of injectate spread and nerve involvement between retrolaminar and erector spinae plane blocks in the thoracic region: a cadaveric study. Anaesthesia. 2018; 73:1244–50.
Article18. Schwartzmann A, Peng P, Maciel MA, Alcarraz P, Gonzalez X, Forero M. A magnetic resonance imaging study of local anesthetic spread in patients receiving an erector spinae plane block. Can J Anaesth. 2020; 67:942–8.
Article19. Behr AU, Chan VWS, Stecco C. Living versus cadaver fascial plane injection. Reg Anesth Pain Med. 2020; 45:156–7.
Article20. Zhang J, He Y, Wang S, Chen Z, Zhang Y, Gao Y, et al. The erector spinae plane block causes only cutaneous sensory loss on ipsilateral posterior thorax: a prospective observational volunteer study. BMC Anesthesiol. 2020; 20:88.
Article21. Elsharkawy H, Pawa A, Mariano ER. Interfascial plane blocks: back to basics. Reg Anesth Pain Med. 2018; 43:341–6.
Article22. Renes SH, Bruhn J, Gielen MJ, Scheffer GJ, van Geffen GJ. In-plane ultrasound-guided thoracic paravertebral block: a preliminary report of 36 cases with radiologic confirmation of catheter position. Reg Anesth Pain Med. 2010; 35:212–6.23. Uppal V, Sondekoppam RV, Sodhi P, Johnston D, Ganapathy S. Single-injection versus multiple-injection technique of ultrasound-guided paravertebral blocks: a randomized controlled study comparing dermatomal spread. Reg Anesth Pain Med. 2017; 42:575–81.24. Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. 2010; 105:842–52.
Article25. Wadhwa A, Kandadai SK, Tongpresert S, Obal D, Gebhard RE. Ultrasound guidance for deep peripheral nerve blocks: a brief review. Anesthesiol Res Pract. 2011; 2011:262070.
Article26. Shoar S, Esmaeili S, Safari S. Pain management after surgery: a brief review. Anesth Pain Med. 2012; 1:184–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomical classification and clinical application of thoracic paraspinal blocks
- Erector spinae plane block for spinal surgery: a systematic review and meta-analysis
- Analgesic Effect of Erector Spinae Plane Block at T2 Level in Arm Surgery
- Erector spinae plane block for pediatric hip surgery: a case report
- Modified pectoral nerve block versus bi-level erector spinae plane block for postoperative analgesia after radical mastectomy surgery: a prospective, randomized, controlled trial
