Comparative study on Kirschner-wire and screw fixation for intra-articular fractures of the proximal phalanx head
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Gwangmyeong Sungae General Hospital, Gwangmyeong, Korea
- KMID: 2532735
- DOI: http://doi.org/10.12790/ahm.22.0025
Abstract
- Purpose
This study compared screw and Kirschner-wire (K-wire) fixation for intra-articular fractures of the proximal phalanx head regarding the success of union and functional outcomes.
Methods
In this retrospective study, we enrolled patients with closed intra-articular fractures of the proximal phalangeal head treated between January 2011 and December 2021. Patients with open wounds, tendon or neurovascular injuries, comminuted fractures, or middle phalangeal fractures were excluded. Patients’ demographics, bone union, proximal interphalangeal (PIP) joint range of motion (ROM), grip power, and complications were collected and analyzed. The percentage of intra-articular surface involvement and the number of bone fragments were also analyzed in relation to the functional results.
Results
Among 41 patients, 21 were managed with screw fixation, and the remaining 20 with K-wire fixation. The mean union rate was 100% in the screw fixation group and 95.0% in the K-wire fixation group, with no statistically significant difference (p=0.488). Other functional parameters (PIP joint ROM, time to bone union, and grip power) were not significantly different between the two groups. Regardless of the treatment modality, the PIP joint ROM showed significant negative associations with the involvement of more intra-articular surfaces (p<0.001) and the presence of a greater number of bone fragments (p=0.040).
Conclusion
In intra-articular fractures of the proximal phalanx head, the treatment modality (screw or K-wire) did not affect the treatment outcome. Instead, the percentage of intra-articular surface involvement and the number of bone fragments showed significant negative associations with the PIP joint ROM after treatment.
Figure
-
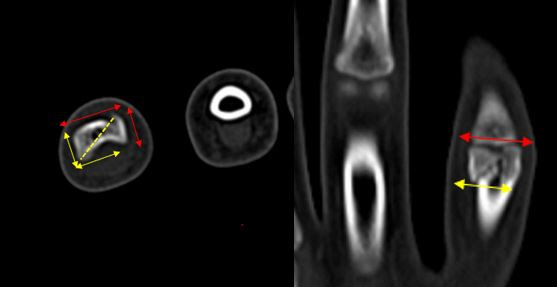
Fig. 1. An example of the intra-articular surface assessment. The red arrows indicate the width and diameter of the entire articular surface, and the yellow arrows indicate that of the dominant (i.e. the largest) bone fragment.
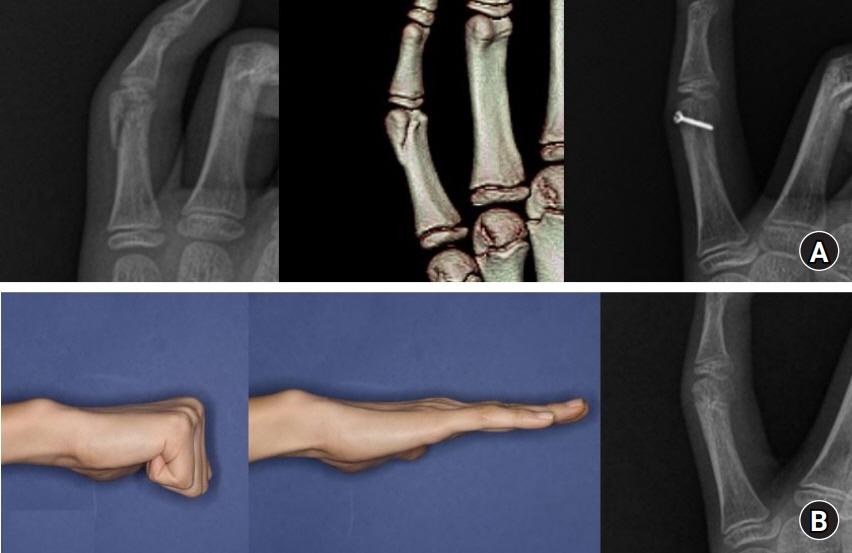
Fig. 2. Twelve-year-old boy came with a proximal phalanx head fracture by physical fight. (A) Preoperative plain X-ray, computed tomography, and immediate postoperative X-ray follow-up with single-screw fixation. (B) Follow-up images at the 49.7th week, showing return to nearly full range of active proximal interphalangeal joint motion and X-ray showing bone union.
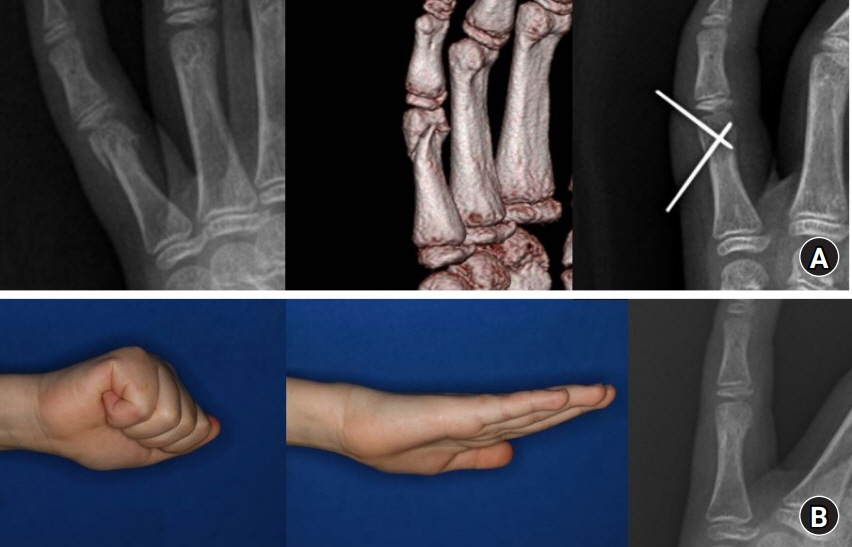
Fig. 3. Ten-year-old girl came with proximal phalanx head fracture during playing volleyball. (A) Preoperative plain X-ray, computed tomography, and immediate postoperative X-ray follow-up with double Kirschner-wire fixation. (B) Follow-up images at the 15.6th week, showing return to nearly full range of active proximal interphalangeal joint motion and X-ray showing bone union.
Reference
-
References
1. Van Oosterom FJ, Brete GJ, Ozdemir C, Hovius SE. Treatment of phalangeal fractures in severely injured hands. J Hand Surg Br. 2001; 26:108–11.2. Borgohain B, Borgohain N, Tittal P. Double parabolic Kirschner-wires as dynamic distractor for treatment of unstable intraarticular phalangeal fractures of hand. Indian J Orthop. 2012; 46:680–4.3. Goldman SB, Amaker RJ, Espinosa RA. James traction splinting for PIP fractures. J Hand Ther. 2008; 21:209–15.4. Freeland AE, Sud V. Unicondylar and bicondylar proximal phalangeal fractures. J Am Soc Surg Hand. 2001; 1:14–24.5. Hamilton SC, Stern PJ, Fassler PR, Kiefhaber TR. Mini-screw fixation for the treatment of proximal interphalangeal joint dorsal fracture-dislocations. J Hand Surg Am. 2006; 31:1349–54.6. James JI. Fractures of the proximal and middle phalanges of the fingers. Acta Orthop Scand. 1962; 32:401–12.7. Aladin A, Davis TR. Dorsal fracture-dislocation of the proximal interphalangeal joint: a comparative study of percutaneous Kirschner wire fixation versus open reduction and internal fixation. J Hand Surg Br. 2005; 30:120–8.8. London PS. Sprains and fractures involving the interphalangeal joints. Hand. 1971; 3:155–8.9. Minamikawa Y, Horii E, Amadio PC, Cooney WP, Linscheid RL, An KN. Stability and constraint of the proximal interphalangeal joint. J Hand Surg Am. 1993; 18:198–204.10. Jupiter JB, Koniuch MP, Smith RJ. The management of delayed union and nonunion of the metacarpals and phalanges. J Hand Surg Am. 1985; 10:457–66.11. Chinchalkar SJ, Gan BS. Management of proximal interphalangeal joint fractures and dislocations. J Hand Ther. 2003; 16:117–28.12. Barton NJ. Fractures of the hand. J Bone Joint Surg Br. 1984; 66:159–67.13. Chin KR, Jupiter JB. Treatment of triplane fractures of the head of the proximal phalanx. J Hand Surg Am. 1999; 24:1263–8.14. Gregory S, Lalonde DH, Fung Leung LT. Minimally invasive finger fracture management: wide-awake closed reduction, K-wire fixation, and early protected movement. Hand Clin. 2014; 30:7–15.15. Carpenter S, Rohde RS. Treatment of phalangeal fractures. Hand Clin. 2013; 29:519–34.16. Weiss AP, Hastings H 2nd. Distal unicondylar fractures of the proximal phalanx. J Hand Surg Am. 1993; 18:594–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A comparative analysis of antegrade and retrograde Kirschner wire fixation for proximal phalanx base fractures
- Comparison between Two Kirschner Wire Fixation and Three Wire Fixation, in Treating of Metacarpal Neck Fracture Using Multiple Retrograde Kirschner Wire Fixation
- Operative Treatment of Metacarpal Shaft Fracture>: Comparision of Low-Profile Miniplating System and Kirschner Wire Fixation
- Minimal Invasive Fixation Methods for the Metacarpal Fracture
- Cannulated Screw and Wire Fixation with Predrilling for Olecranon Osteotomy in Intra-articular Comminuted Distal Humerus Fractures
