Embarrassed Radiofrequency Catheter Ablation of Supraventricular Tachycardia in Pectus Excavatum
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University College of Medicine, Seoul, Korea
- KMID: 2532212
- DOI: http://doi.org/10.12771/emj.2022.e6
Abstract
- A 16-year-old patient with pectus excavatum visited our hospital because of palpitation. He underwent first Nuss operations at the age of 3. When he was 13 years old, the slow-fast type atrioventricular nodal reentrant tachycardia was documented during electrophysiology study. However, the catheter ablation was not conducted because of recurrent atrial fibrillation during procedure. At that time, second Nuss operation was performed due to progressive chest wall deformity. And then, atrioventricular nodal reentrant tachycardia was successfully treated by radiofrequency catheter ablation at the higher position than usual slow pathway zone under the modified fluoroscopic view with the cranial angle although distorted right atrial geometry and radiographic obstacle of Nuss operation bar. The concern about abnormal cardiac and electrical anatomy, and the accurate and modified procedure technique are essential in patients with pectus excavatum. (Ewha Med J 2022;45(3):e6)
Keyword
Figure
-
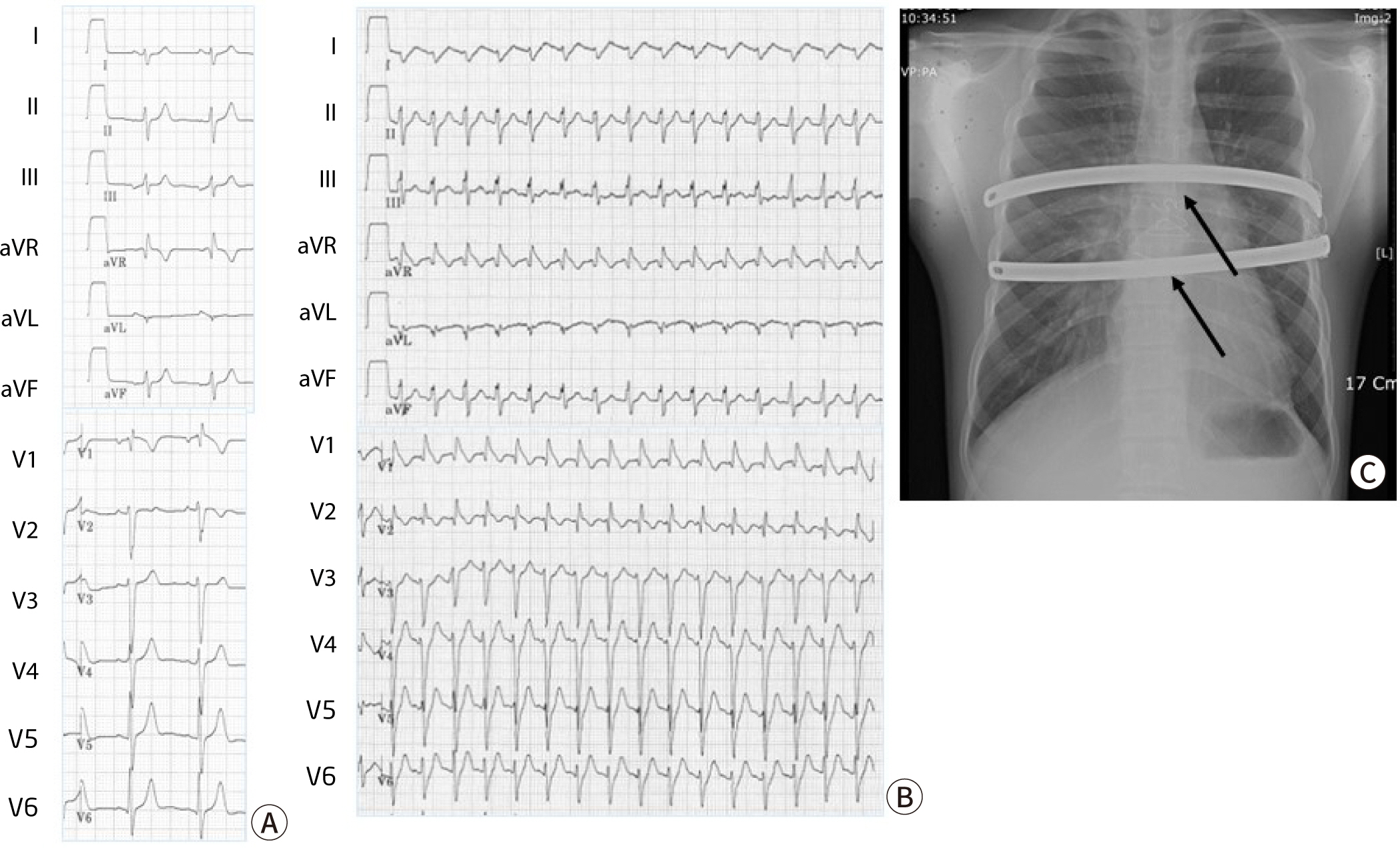
Fig. 1. 12-lead surface electrocardiogram and Chest X-ray. (A) The baseline surface electrocardiogram showing incomplete right bundle branch block. (B) A wide QRS tachycardia with heart rate of 180 bpm suggesting supraventricular tachycardia with incomplete right bundle branch block pattern. (C) Chest X-ray showing Nuss operation bar (arrows).
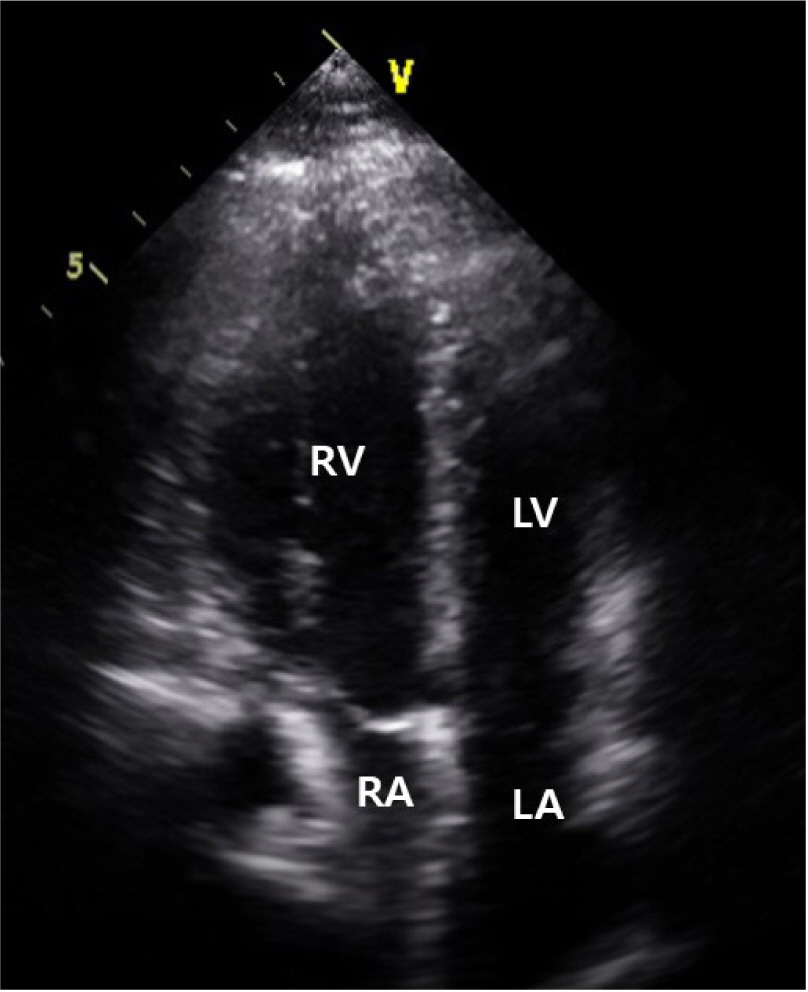
Fig. 2. Transthoracic echocardiography showing the compression of right atrium on apical four chamber view. RV, right ventricle; LV, left ventricle; RA, right atrium; LA, left atrium.
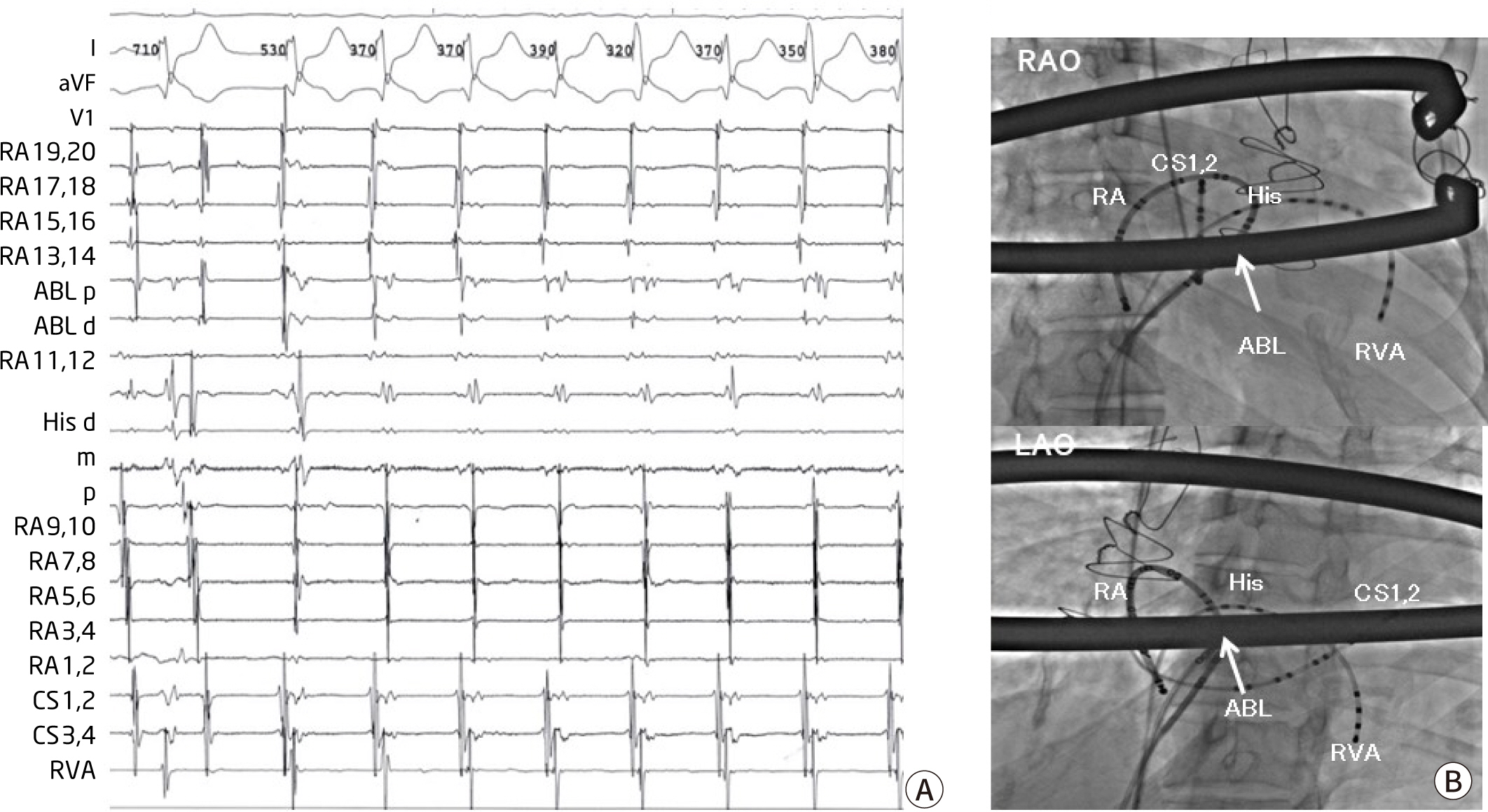
Fig. 3. Successful ablation site of atrioventricular nodal reentrant tachycardia. (A) Intra-cardiac electrogram showing the atrioventricular nodal reentrant tachycardia with earliest atral activation site of His area at a cycle length of 380 ms. (B) Fluoroscopic images in the left anterior oblique (LAO) and right anterior oblique (RAO) projection showing the masablation catheter positioned at the higher site than usual slow pathway zone. RA, right atrium; CS, coronary sinus; ABL, ablation catheter; RV, right ventricular catheter; His, His potential.
Reference
-
References
1. Tran NT, Klein JL, Mounsey JP, Chung EH, Schwartz JD, Pursell I, et al. Lone atrial fibrillation is associated with pectus excavatum. Heart Rhythm. 2013; 10:1263–1269. DOI: 10.1016/j.hrthm.2013.05.010. PMID: 23692892.
Article2. Hak CW, Lim YP, Liew R, Hsu LF. Pectus excavatum: uncommon electrical abnormalities caused by extrinsic right ventricular compression. J Cardiovasc Electrophysiol. 2014; 25:324–327. DOI: 10.1111/jce.12336. PMID: 24303874.
Article3. Wang G, Yu Z, Zhang C, Zang H, Monti L, Jeong JY, et al. Pectus excavatum requiring temporary pacemaker implantation before Nuss procedure: a case report. J Thorac Dis. 2020; 12:4985–4990. DOI: 10.21037/jtd-20-2312. PMID: 33145072. PMCID: PMC7578454.
Article4. Media AS, Christensen TD, Katballe N, Pilegaard HK, De Paoli FV. Prevalence of comorbidities in a surgical pectus excavatum population. J Thorac Dis. 2021; 13:1652–1657. DOI: 10.21037/jtd-20-3352. PMID: 33841956. PMCID: PMC8024824.
Article5. Rha EY, Kim JH, Yoo G, Ahn S, Lee J, Jeong JY. Changes in thoracic cavity dimensions of pectus excavatum patients following Nuss procedure. J Thorac Dis. 2018; 10:4255–4261. DOI: 10.21037/jtd.2018.06.159. PMID: 30174871. PMCID: PMC6105938.
Article6. Pimenta J, Vieira A, Henriques-Coelho T. Ventricular arrhythmia solved by surgical correction of pectus excavatum. Interact Cardiovasc Thorac Surg. 2018; 26:706–708. DOI: 10.1093/icvts/ivx397. PMID: 29244154.
Article7. Shaalan AM, Kasb I, Elwakeel EE, Elkamali YA. Outcome of surgical repair of pectus excavatum in adults. J Cardiothorac Surg. 2017; 12:72. DOI: 10.1186/s13019-017-0635-z. PMID: 28851442. PMCID: PMC5576375.
Article8. Tanaka A, Takemoto M, Kang H, Aoki R, Antoku Y, Mito T, et al. Paroxysmal atrial fibrillation in patients successfully treated by radiofrequency catheter ablation with severely compression, lateral displacement, and clockwise rotation of their hearts due to severe pectus excavatum. Intern Med. 2018; 57:3381–3384. DOI: 10.2169/internalmedicine.1313-18. PMID: 29984756. PMCID: PMC6306521.
Article9. De Simone CV, Sagar S, Moir C, Asirvatham SJ. Combined surgical and ablative cure for localized sternal compression-induced cardiomyopathy and ventricular tachyarrhythmia. J Thorac Cardiovasc Surg. 2012; 144:85–87. DOI: 10.1016/j.jtcvs.2012.03.033. PMID: 22502968.10. Nuss D, Kelly RE Jr, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg. 1998; 33:545–552. DOI: 10.1016/S0022-3468(98)90314-1.
Article11. Coln E, Carrasco J, Coln D. Demonstrating relief of cardiac compression with the Nuss minimally invasive repair for pectus excavatum. J Pediatr Surg. 2006; 41:683–686. DOI: 10.1016/j.jpedsurg.2005.12.009. PMID: 16567176.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Ablation of Resistant Left Lateral Accessory Pathway and Coexisting Atypical Atrioventricular Nodal Reentrant Tachycardia
- Safety of Radiofrequency Catheter Ablation in Patients with Supraventricular Tachycardia Confirmed by Means of Echocardiography
- Catheter ablation for treatment of tachyarrhythmia
- Atrioventricular Nodal Reentrant Tachycardia (AVNRT)
- Treatment of Supraventricular Tachycardia by Catheter Ablation Using Radiofrequency Currents in Children and Adolescents
