Pediatric Sarcoidosis Misdiagnosed as Hepatosplenic Abscesses: A Case Report and Review
- Affiliations
-
- 1Department of Pediatrics, Severance Children’s Hospital, Yonsei University College of Medicine, Seoul, Korea
- 2Department of Pathology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- 3Institute for Immunology and Immunological Diseases, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2530682
- DOI: http://doi.org/10.4078/jrd.2022.29.3.181
Abstract
- Sarcoidosis is a systemic granulomatous disorder of unknown etiology characterized by granuloma formation. Due to the limited incidence of sarcoidosis in pediatric patients, little is known about the clinical course of this disease. A combination of clinical, radiologic, and pathologic examination is necessary to exclude other differential diagnoses (i.e., infection and granulomatous inflammatory disorder) and establish a diagnosis of sarcoidosis. Here, we report a case of histologically confirmed sarcoidosis initially misdiagnosed as hepatosplenic abscesses in an 11-year-old male. Treatment with corticosteroids improved his symptoms and resolved his skin and hepatosplenic lesions. A three-year follow-up was uneventful. This study emphasizes the importance of considering sarcoidosis in children presenting with findings of multi-organ involvement in the presence of histologic evidence of granuloma.
Keyword
Figure
-
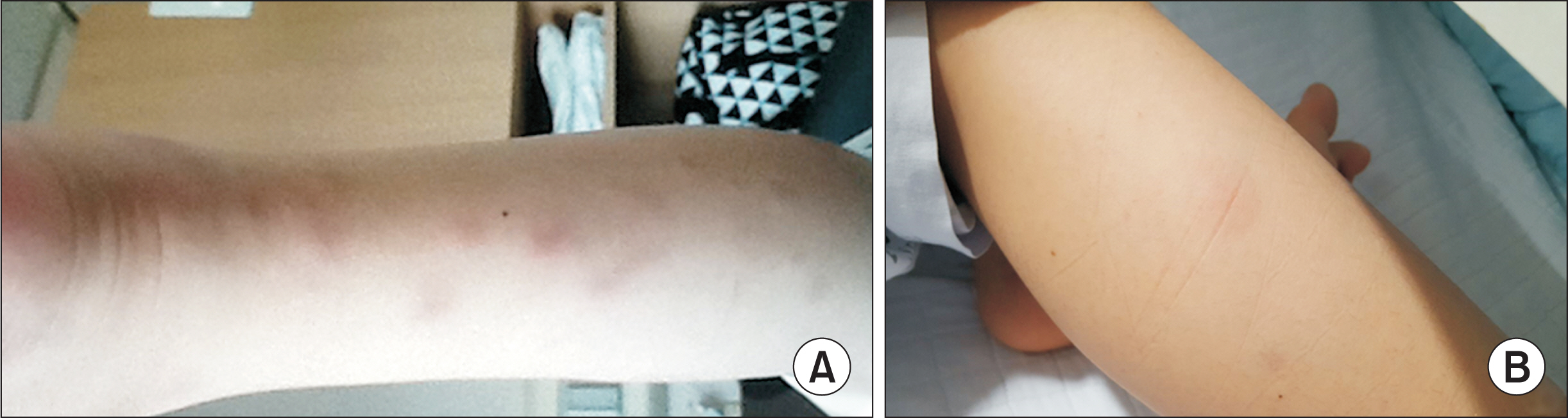
Fig. 1 Skin lesions. (A) The patient presented with skin rashes with multiple erythematous indurated nodules on both legs two months prior to consult. The figure is the lesions in the posterior part of the left lower leg. (B) The patient presented with multiple painful, erythematous indurated nodules in anterior aspect of the right lower leg on hospital day 18.
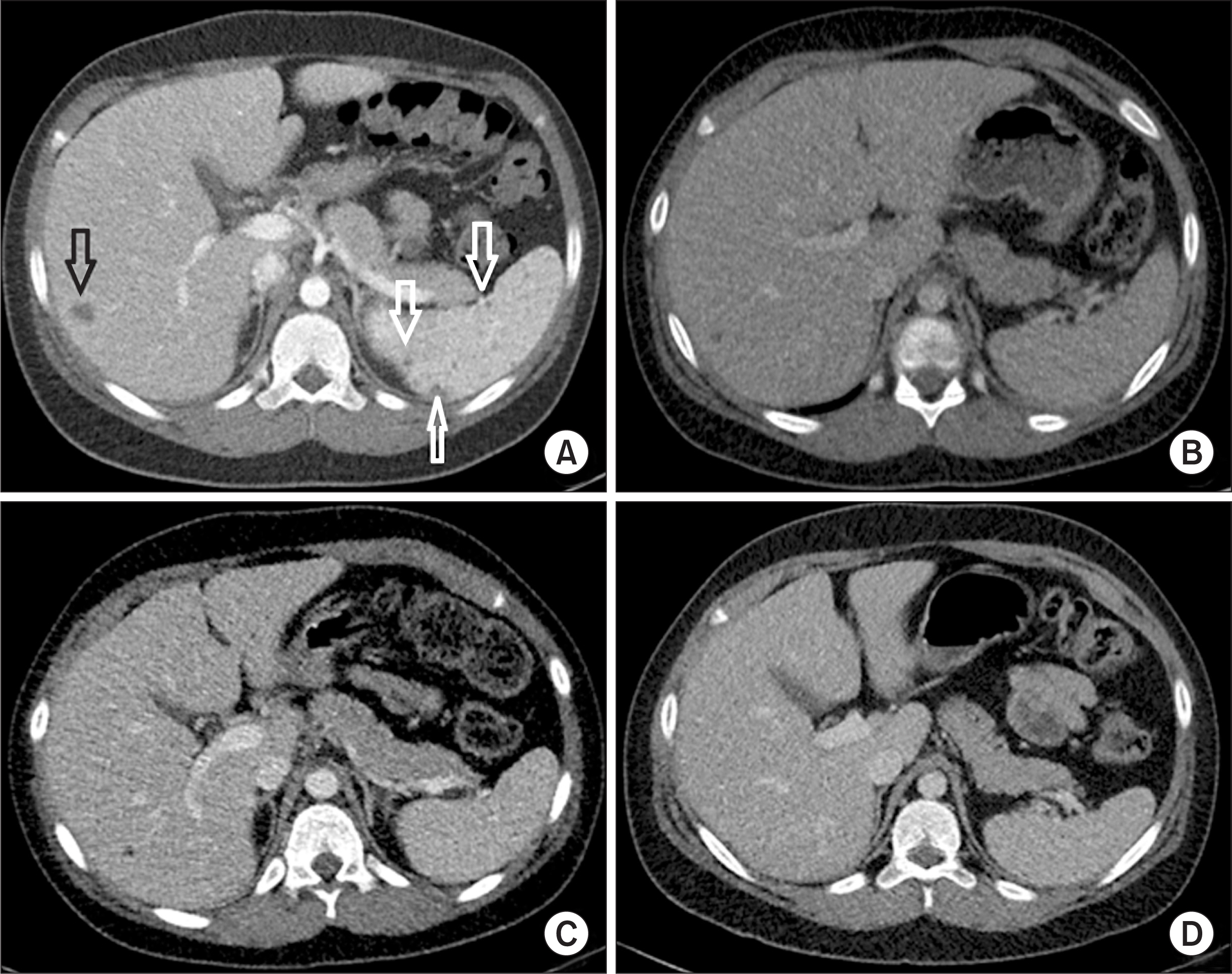
Fig. 2 Abdominal computed tomography (CT) findings. (A) CT taken at the other hospital 5 weeks before hospitalization showed multiple poorly defined small hypodense lesions in the spleen (white arrows), and a small hypodense lesion with mild peripheral enhancement in the liver (black arrow), suggestive of hepatosplenic abscesses. (B) Initial CT done in our hospital on the day of hospitalization revealed resolution of the splenic abscesses and size reduction of the low-attenuating lesion at the right hemiliver. (C) Follow-up CT on hospital day 17 showed further size reduction of the hepatic lesion. (D) Six months later in an outpatient clinic, no specific lesions were observed in abdominal CT.

Fig. 3 Clinical time course of the patient. CRP: C-reactive protein, ESR: erythrocyte sedimentation rate, WBC: white blood cell, IV: intravenous.

Fig. 4 Chest computed tomography (CT) findings. (A, B) Chest CT on hospital day 20 revealed multiple small nodular lesions in both lungs (arrow). (C, D) Six months later in an outpatient clinic, no specific lesions were observed in chest CT.

Fig. 5 Histopathologic examination of skin biopsy specimen from the right lower leg. (A) Infiltration of mixed inflammatory cells (lymphocytes, histiocytes, plasma cells, etc.) is observed in subcutaneous fat lobules (arrows in A) (H&E stain, x100). (B) Noncaseating epithelioid and giant cell granuloma are noted (arrows in B) (H&E stain, x200).
Reference
-
1. Shetty AK, Gedalia A. 2000; Sarcoidosis in children. Curr Probl Pediatr. 30:149–76. DOI: 10.1067/mps.2000.105929. PMID: 10826082.
Article2. Chiu B, Chan J, Das S, Alshamma Z, Sergi C. 2019; Pediatric sarcoidosis: a review with emphasis on early onset and high-risk sarcoidosis and diagnostic challenges. Diagnostics (Basel). 9:160. DOI: 10.3390/diagnostics9040160. PMID: 31731423. PMCID: PMC6963233.
Article3. Fauroux B, Clément A. 2005; Paediatric sarcoidosis. Paediatr Respir Rev. 6:128–33. DOI: 10.1016/j.prrv.2005.03.007. PMID: 15911458.
Article4. Heinle R, Chang C. 2014; Diagnostic criteria for sarcoidosis. Autoimmun Rev. 13:383–7. DOI: 10.1016/j.autrev.2014.01.035. PMID: 24424172.
Article5. Nathan N, Sileo C, Calender A, Pacheco Y, Rosental PA, Cavalin C, et al. 2019; Paediatric sarcoidosis. Paediatr Respir Rev. 29:53–9. DOI: 10.1016/j.prrv.2018.05.003. PMID: 30917882.
Article6. Rybicki BA, Major M, Popovich J Jr, Maliarik MJ, Iannuzzi MC. 1997; Racial differences in sarcoidosis incidence: a 5-year study in a health maintenance organization. Am J Epidemiol. 145:234–41. DOI: 10.1093/oxfordjournals.aje.a009096. PMID: 9012596.
Article7. Rose CD, Wouters CH. Petty RE, Laxer RM, Lindsley CB, Wedderburn LR, Mellins ED, Fuhlbrigge RC, editors. 2021. Pediatric sarcoidosis. Textbook of pediatric rheumatology. 8th ed. Elsevier;Philadelphia: p. 559–66. e2.8. Gedalia A, Khan TA, Shetty AK, Dimitriades VR, Espinoza LR. 2016; Childhood sarcoidosis: Louisiana experience. Clin Rheumatol. 35:1879–84. DOI: 10.1007/s10067-015-2870-9. PMID: 25616361.
Article9. Hoffmann AL, Milman N, Byg KE. 2004; Childhood sarcoidosis in Denmark 1979-1994: incidence, clinical features and laboratory results at presentation in 48 children. Acta Paediatr. 93:30–6. DOI: 10.1111/j.1651-2227.2004.tb00670.x. PMID: 14989436.
Article10. Shetty AK, Gedalia A. 2008; Childhood sarcoidosis: a rare but fascinating disorder. Pediatr Rheumatol Online J. 6:16. DOI: 10.1186/1546-0096-6-16. PMID: 18811966. PMCID: PMC2559831.
Article11. Whang SW, Kim DS, Lee KH. 2000; A case of early-onset childhood sarcoidosis. Korean J Dermatol. 38:1696–8.12. Jang KA, Choi JH, Sung KJ, Moon KC, Koh JK, Kim HK. 1998; Sarcoidosis in a four-year-old girl. Korean J Dermatol. 36:331–4.13. Kim SA, Bae SY, Lee SY, Jeong DC, Chung SY, Kang JH. 2006; A case of pulmonary sarcoidosis in a 6-year-old girl. Pediatr Allergy Respir Dis. 16:253–8.14. Lee JH, Lim YJ, Lee S, Joo KB, Choi YY, Park CK, et al. 2012; Early-onset childhood sarcoidosis with incidental multiple enchondromatosis. J Korean Med Sci. 27:96–100. DOI: 10.3346/jkms.2012.27.1.96. PMID: 22219622. PMCID: PMC3247783.
Article
