Tuberc Respir Dis.
2008 Aug;65(2):121-124.
Sarcoidosis Initially Presenting as a Nasal Cavity Mass Misdiagnosed as Tuberculosis
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. droij@chonnam.ac.kr
Abstract
- We experienced a rare case of sinonasal sarcoidosis initially presenting as nasal cavitary mass. When the clinical course was different from that of typical tuberculosis, physician should think the possibility of sarcoidosis, and re-biopsy or retrospective review of pathological findings might be helpful.
Keyword
Figure
-
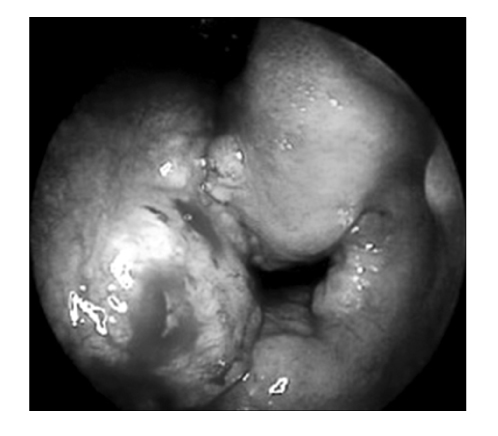
Figure 1 Endoscopic findings of nose shows massive hypertrophy of nasal septum and inferior turbinate.
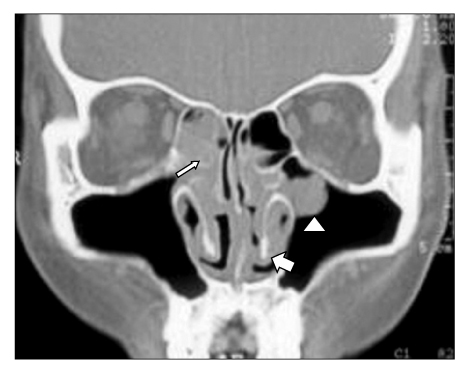
Figure 2 Coronal nasal CT shows soft tissue density (thin arrow) filling in both inferior ethmoid sinus, round soft tissue attenuated lesion (arrow head) in left maxillary sinus and lining mucosal thickening (thick arrow) of nasal septum and inferior turbinate.
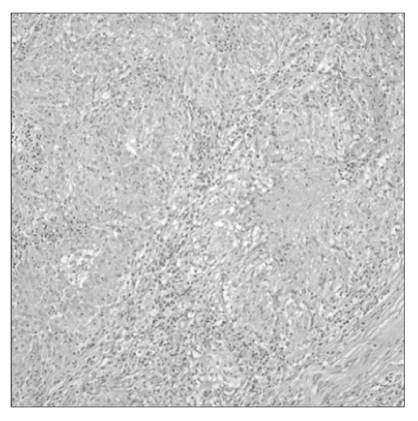
Figure 3 The nasal biopsy specimen shows multiple non-caseating granulomas. Granular necrosis is also visible in this specimen (H&E stain, ×200).
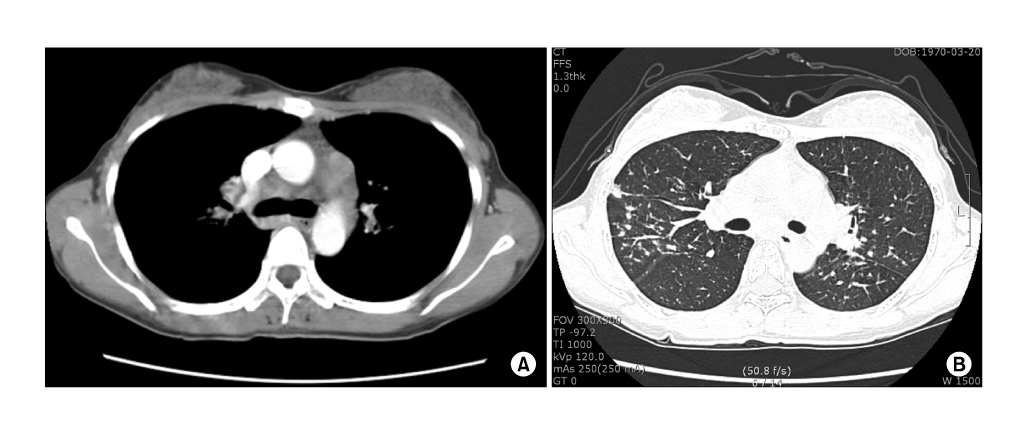
Figure 4 Chest CT shows multiple hilar lymphadenopathies (A). Multiple small nodules with peribronchovascular distribution, and small branching structures in RML (B).
Reference
-
1. Zeitlin JF, Tami TA, Baughman R, Winget D. Nasal and sinus manifestations of sarcoidosis. Am J Rhinol. 2000. 14:157–161.2. Tay HL, Vaughan-Jones R, Qureshi SS. Ethmoidal sarcoidosis. J Laryngol Otol. 1994. 108:682–684.3. Mana J, Badrinas F, Morera J, Fite E, Manresa F, Fernandez-Nogues F. Sarcoidosis in Spain. Sarcoidosis. 1992. 9:118–122.4. James GD. Sarcoidosis and other granulomatous disorders. 1994. 1st ed. New York: Marcel Dekker.5. Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med. 1999. 160:736–755.6. Sheffield EA, Williams WJ. James DG, editor. Pathology. Sarcoidosis and other granulomatous disorders. 1994. New York: Marcel Dekker;45–67.7. McCaffrey TV, McDonald TJ. Sarcoidosis of the nose and paranasal sinuses. Laryngoscope. 1983. 93:1281–1284.8. Krespi YP, Kuriloff DB, Aner M. Sarcoidosis of the sinonasal tract: a new staging system. Otolaryngol Head Neck Surg. 1995. 112:221–227.9. Braun JJ, Gentine A, Pauli G. Sinonasal sarcoidosis: review and report of fifteen cases. Laryngoscope. 2004. 114:1960–1963.10. Kim DS. Sarcoidosis in Korea: report of the Second Nationwide Survey. SarcoidosisVasc Diffuse Lung Dis. 2001. 18:176–180.11. Domestic Statistics "Trend of case notification rate per 100,000 by year, 2001-2005". The Korean National Tuberculosis Association. 16 Jul. 2007. Available from: http://www.knta.or.kr/korea/study/study05.asp.12. Marks SC, Goodman RS. Surgical management of nasal and sinus sarcoidosis. Otolaryngol Head Neck Surg. 1998. 118:856–858.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Primary Sarcoidosis of the Nasal Cavity
- A Case of Nasal Involvement of Sarcoidosis
- A Case of Nasopharyngeal Tuberculosis Which Was Difficult to Differentiate From Sarcoidosis
- Six Cases of Nasal Cavity and Nasopharyngeal Tuberculosis
- A Case of Huge Fungus Ball in Nasal Cavity Misdiagnosed as Rhinolith on Nasal Septum
