Endoscopic balloon dilations for strictures of rectum, ileocecal valve and duodenum in a patient with X-linked inhibitor of apoptosis deficiency: a case report
- Affiliations
-
- 1Department of Gastroenterology and Hepatology, Hokkaido University Graduate School of Medicine, Sapporo, Japan
- 2Department of Gastroenterology and Hepatology, Hokkaido University Hospital, Sapporo, Japan
- 3Department of Hematology, Hokkaido University Hospital, Sapporo, Japan
- KMID: 2529574
- DOI: http://doi.org/10.5217/ir.2021.00029
Abstract
- X-linked inhibitor of apoptosis (XIAP) deficiency is a rare primary immunodeficiency and gastrointestinal (GI) lesions in XIAP deficiency are similar to Crohn’s disease. For patients with Crohn’s disease, endoscopic balloon dilation (EBD) is known to be a standard procedure for intestinal strictures including upper GI tract. However, there are no articles which mention the efficacy of EBDs for the strictures in upper GI tract in patients with XIAP deficiency. Herein, we describe an 18-year-old male with XIAP deficiency in whom EBDs for the rectum, ileocecal valve (ICV), and duodenum were performed. Before hematopoietic stem cell transplantation (HSCT), GI endoscopy revealed strictures of the rectum, ICV and duodenum with active ulcers. Although these ulcers healed after HSCT, the strictures progressed. Therefore, we performed EBDs for the strictures of the rectum, ICV, and duodenum. In contrast studies, we did not find any other strictures in the small intestine. Throughout the patient’s clinical course, no complications of EBD occurred. He started eating after EBDs, but abdominal symptoms did not relapse without any dietary restrictions. Our case suggests that EBD could be an effective and safe procedure for intestinal strictures including upper GI tract after HSCT in patients with XIAP deficiency.
Keyword
Figure
-
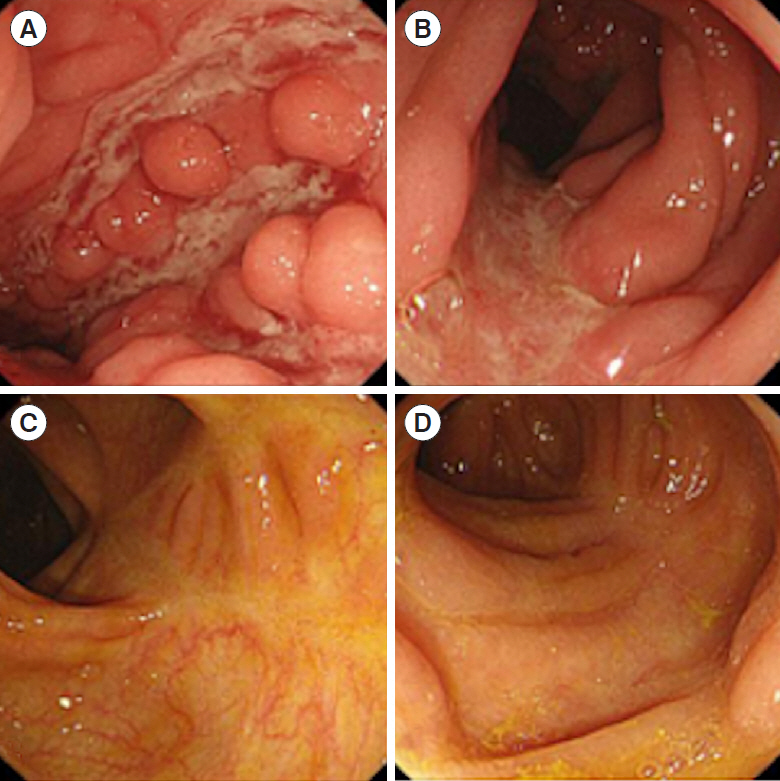
Fig. 1. Endoscopic images of the large intestine. Before hematopoietic stem cell transplantation (HSCT), multiple longitudinal ulcers in the transverse colon (A) and descending colon (B) were observed. After HSCT, these ulcers were healing in the transverse colon (C) and descending colon (D).
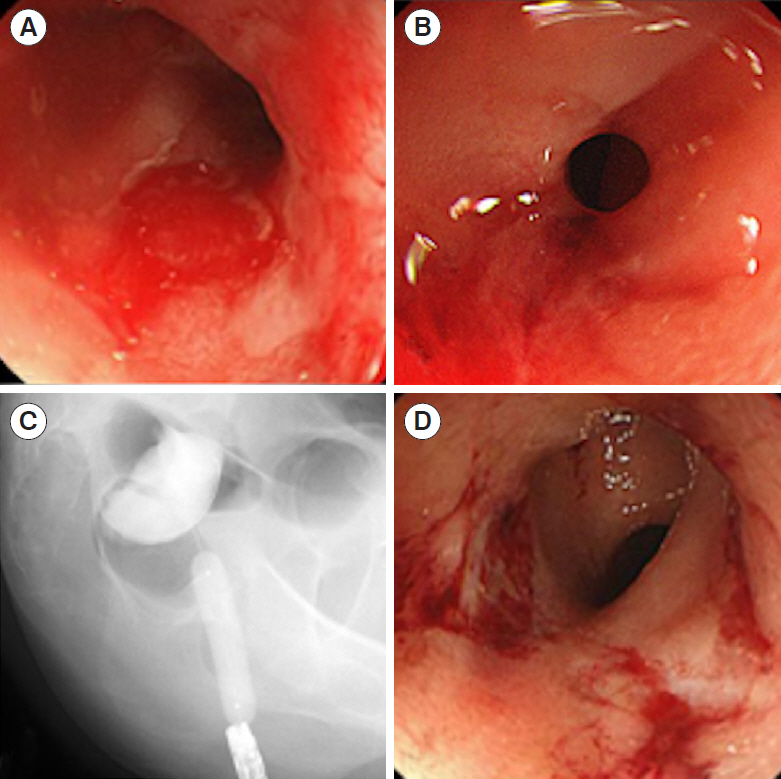
Fig. 2. Endoscopic and fluoroscopic images of the rectum. Before hematopoietic stem cell transplantation (HSCT), the rectum was mildly stenosed with active ulcers (A). After HSCT, active ulcers were healing; however, the stricture of the rectum progressed (B). We performed endoscopic balloon dilations for the rectum up to 12 mm (C, D).

Fig. 3. Endoscopic and fluoroscopic images of the ileocecal valve (ICV). Before hematopoietic stem cell transplantation (HSCT), the ICV was severely stenosed with an active ulcer (A). After HSCT, the active ulcer was healing, and the stricture of the ICV remained severe (B). We performed endoscopic balloon dilations for the ICV up to 10 mm (C, D).
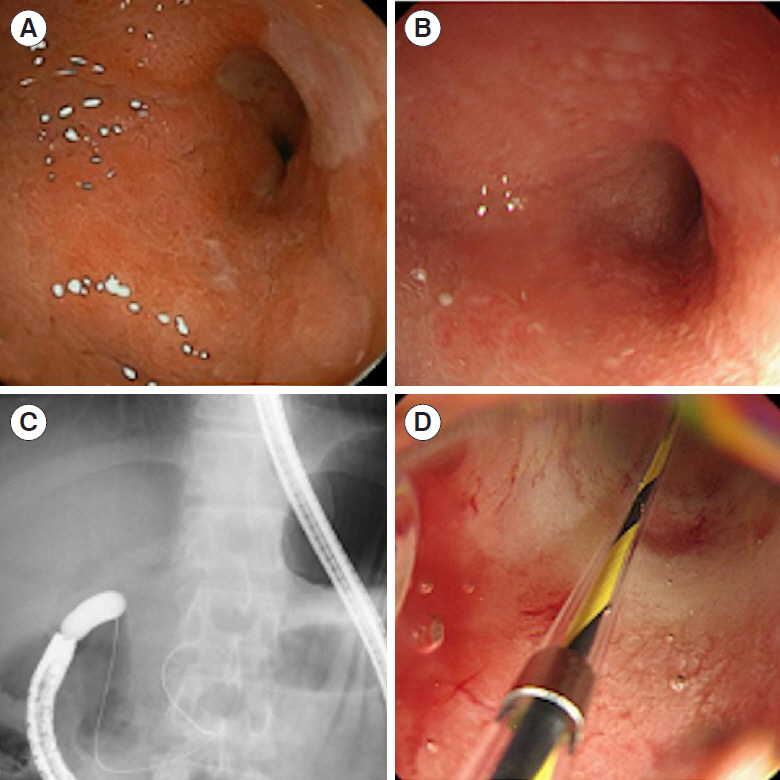
Fig. 4. Endoscopic and fluoroscopic images of the duodenum. Before hematopoietic stem cell transplantation (HSCT), the duodenum bulb was mildly stenosed with an active ulcer (A). After HSCT, the active ulcer was healing; however, the stricture of the duodenum progressed (B). We performed endoscopic balloon dilations for the rectum up to 10 mm (C, D).
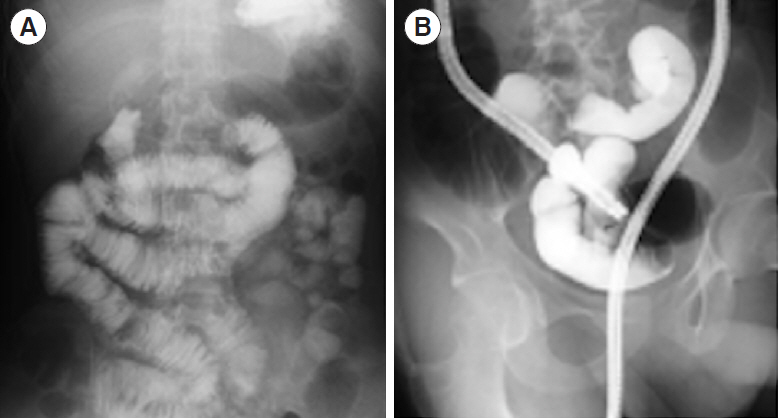
Fig. 5. Fluoroscopic images of the small intestine (A, B). In contrast studies, no other stricture in the small intestine was observed.
Reference
-
1. Latour S, Aguilar C. XIAP deficiency syndrome in humans. Semin Cell Dev Biol. 2015; 39:115–123.
Article2. Aguilar C, Lenoir C, Lambert N, et al. Characterization of Crohn disease in X-linked inhibitor of apoptosis-deficient male patients and female symptomatic carriers. J Allergy Clin Immunol. 2014; 134:1131–1141.
Article3. Zeissig Y, Petersen BS, Milutinovic S, et al. XIAP variants in male Crohn’s disease. Gut. 2015; 64:66–76.
Article4. Ono S, Okano T, Hoshino A, et al. Hematopoietic stem cell transplantation for XIAP deficiency in Japan. J Clin Immunol. 2017; 37:85–91.
Article5. Sunseri WM, Kugathasan S, Keljo DJ, et al. IBD LIVE case series: case 3: very early-onset inflammatory bowel disease: when genetic testing proves beneficial. Inflamm Bowel Dis. 2015; 21:2958–2968.6. Atreja A, Aggarwal A, Dwivedi S, et al. Safety and efficacy of endoscopic dilation for primary and anastomotic Crohn’s disease strictures. J Crohns Colitis. 2014; 8:392–400.
Article7. Otagiri S, Sugiura R, Katsurada T, et al. Gastrointestinal: endoscopic balloon dilations for an intestinal stricture in a patient with X-linked inhibitor of apoptosis deficiency. J Gastroenterol Hepatol. 2019; 34:1895.
Article8. Tsuma Y, Imamura T, Ichise E, et al. Successful treatment of idiopathic colitis related to XIAP deficiency with allo-HSCT using reduced-intensity conditioning. Pediatr Transplant. 2015; 19:E25–E28.
Article9. Chang CW, Wong JM, Tung CC, Shih IL, Wang HY, Wei SC. Intestinal stricture in Crohn’s disease. Intest Res. 2015; 13:19–26.
Article10. Klag T, Wehkamp J, Goetz M. Endoscopic balloon dilation for Crohn’s disease-associated strictures. Clin Endosc. 2017; 50:429–436.
Article11. Gustavsson A, Magnuson A, Blomberg B, Andersson M, Halfvarson J, Tysk C. Endoscopic dilation is an efficacious and safe treatment of intestinal strictures in Crohn’s disease. Aliment Pharmacol Ther. 2012; 36:151–158.
Article12. Bettenworth D, Mücke MM, Lopez R, et al. Efficacy of endoscopic dilation of gastroduodenal Crohn’s disease strictures: a systematic review and meta-analysis of individual patient data. Clin Gastroenterol Hepatol. 2019; 17:2514–2522.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Difficulty of balloon dilatation in corrosive esophageal strictures
- A Case of Dieulafoy-like Lesion with Massive Bleeding at Ileocecal Valve Following Acute Infectious Colitis in a Pediatric Patient
- Colitis Cystica Profunda Causing Intussusception: A Case Report
- A Case of Adenocarcinoma in Ileocecal Valve Mimicking Inflammatory Bowel Disease
- Clinical Outcomes of Dilation Therapy for Anastomotic Esophageal Stricture
