Modified Transseptal Approach: An Adjunct to Prelacrimal Recess Approach for Extensive Inverted Papilloma of Maxillary Sinus, How We Do It
- Affiliations
-
- 1Department of ENT, GV ENT Clinic, Kerala, India
- KMID: 2528319
- DOI: http://doi.org/10.18787/jr.2021.00368
Abstract
- The transseptal approach to the maxillary sinus has been described for resection of extensive tumours of the nose and paranasal sinuses. We describe a modification of this method in a patient diagnosed with inverted papilloma for which he had undergone two previous operations. This method provides complete access to the maxillary sinus, particularly the anterior wall, to provide adequate reach and ensure complete removal of tumours. We describe a technique modifying the existing transseptal approach used as an adjunct to prelacrimal recess approach, wherein a hemitransfixation incision placed in the contralateral nasal cavity along the septum provides access to the maxillary sinus with angled instruments. This modified transseptal approach provided better reach and access to the maxillary sinus. Postoperatively, there was no evidence of septal scarring or perforation and no evidence of lesion recurrence. Our technique is an easy modification to the transseptal approach that is a useful tool to access hidden areas of the maxillary sinus without associated morbidity.
Keyword
Figure
-

Fig. 1. Preoperative diagnostic nasal endoscopy.
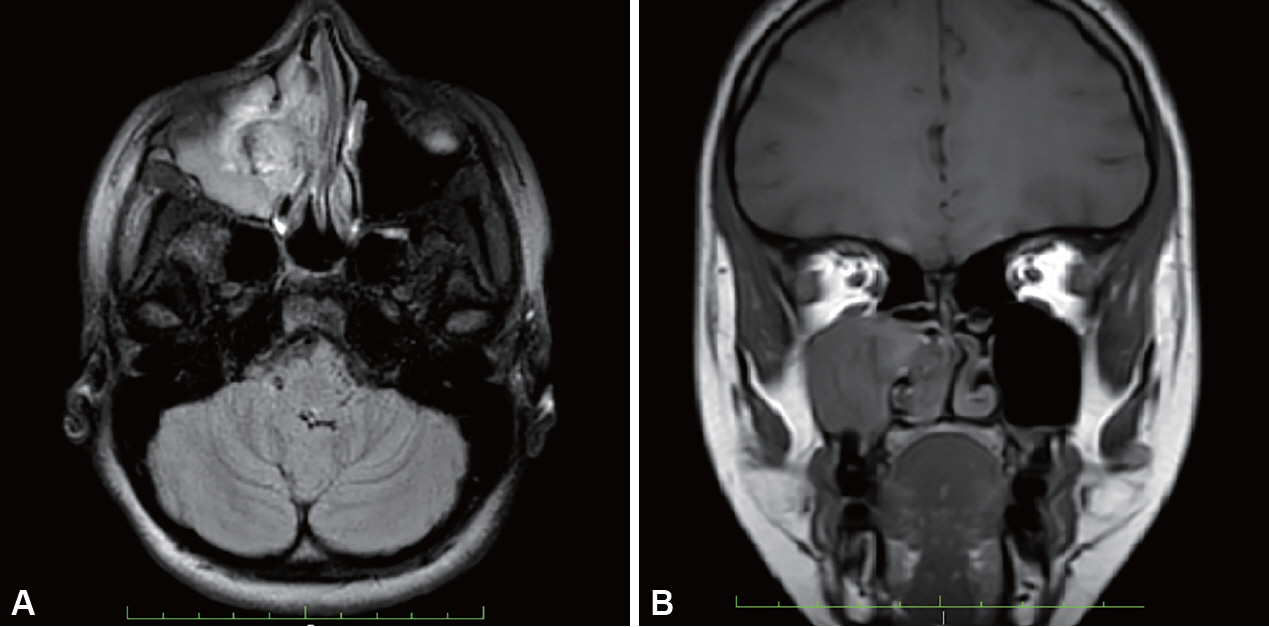
Fig. 2. Contrast enhanced magnetic resonance imaging of paranasal sinuses. (A) Axial and (B) coronal cut.
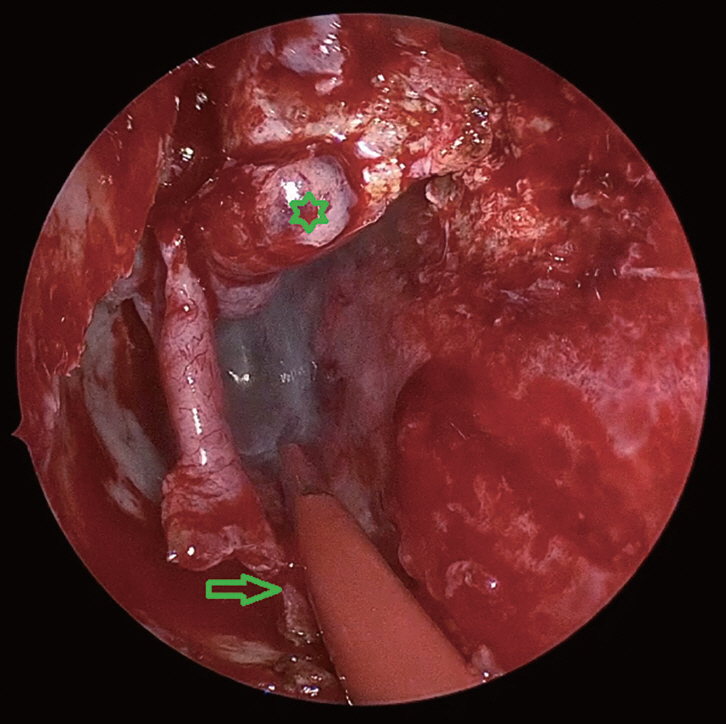
Fig. 3. Incision made anterior to right inferior turbinate and extended along the floor of nose, posteriorly (star indicates inverted papilloma and arrow indicates remnant of inferior turbinate).
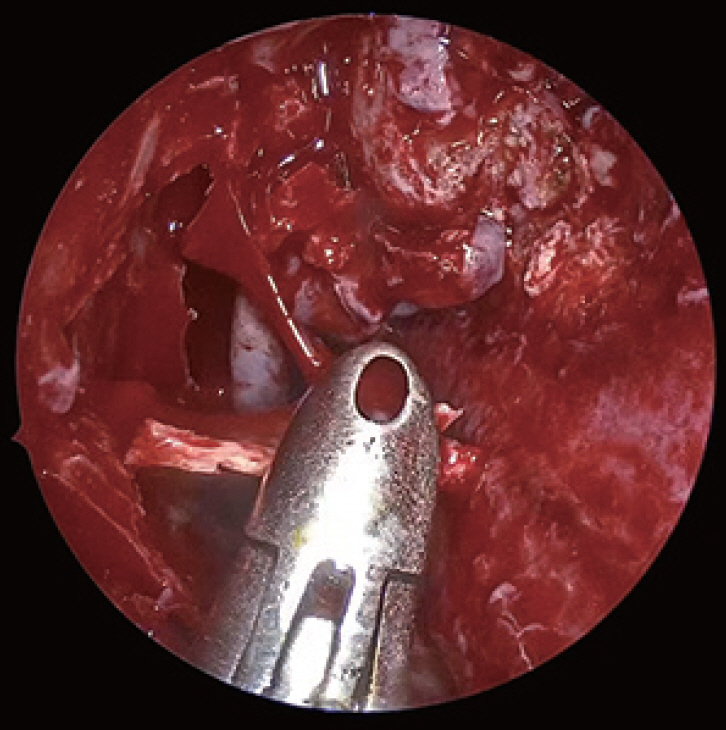
Fig. 4. Flap elevated exposing entire lateral wall of nose.
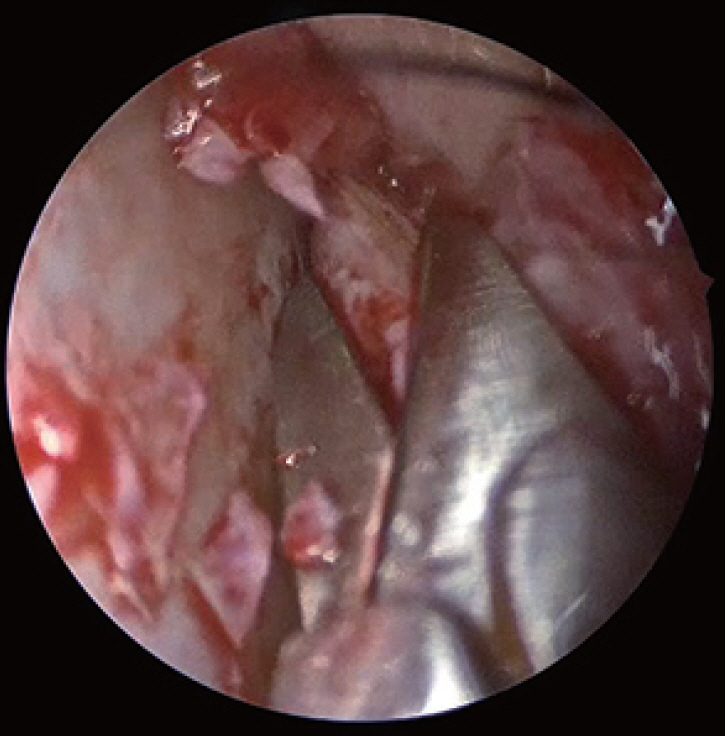
Fig. 5. Incision was extended posteriorly, horizontal along the superior part of nasal septum beneath the nasal roof (left side).
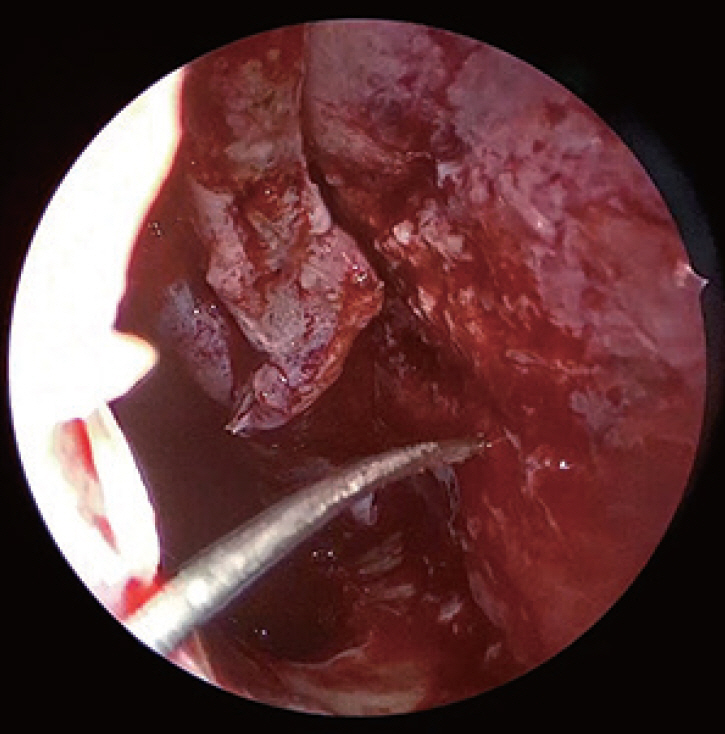
Fig. 6. A curved needle (Ethilon 3-0, Ethicon, Johnson and Johnson, Piscataway, NJ, USA) is introduced from the diseased side corresponding to the maxillary sinus opening.
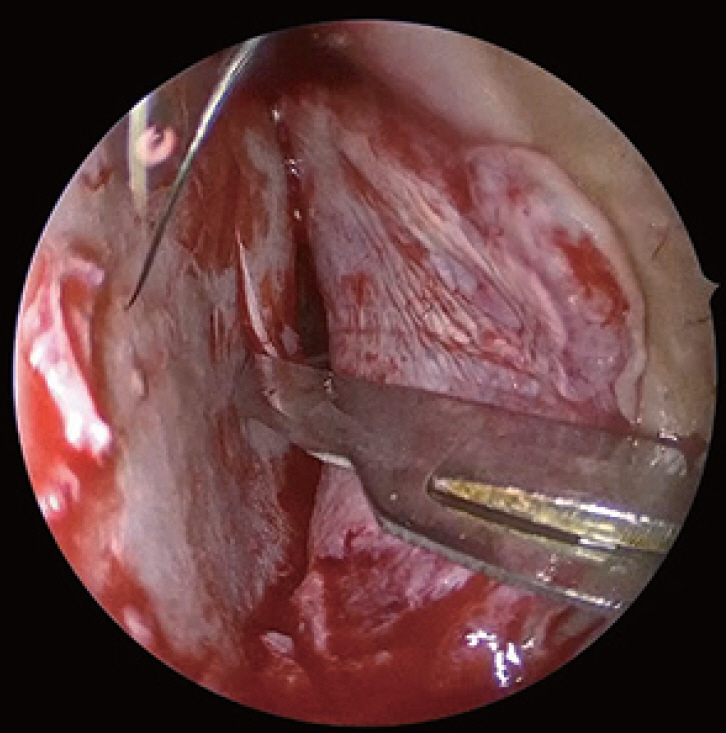
Fig. 7. Cruciate incision made along contralateral part of septal cartilage, corresponding to the point of entry of the curved needle (Ethilon 3-0, Ethicon, Johnson and Johnson, Piscataway, NJ, USA).
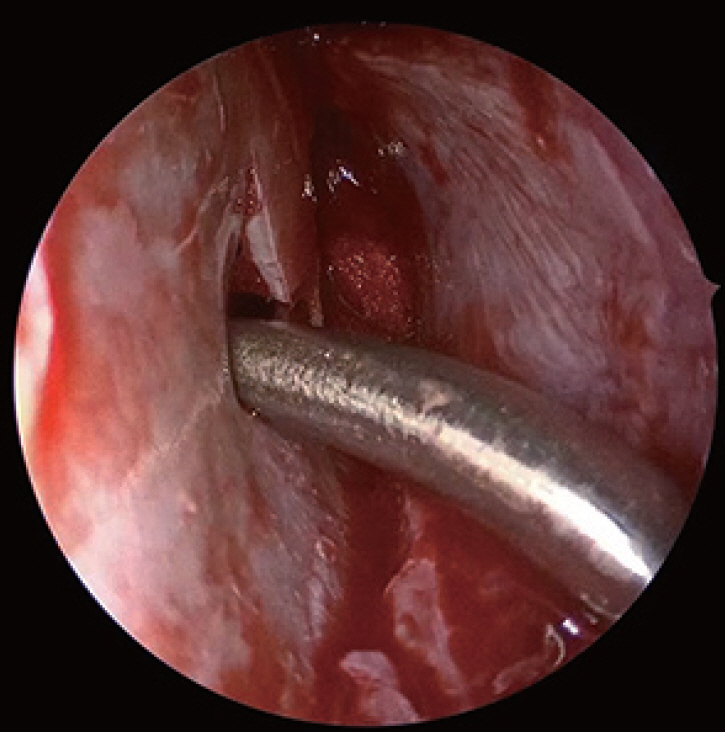
Fig. 8. Curved instruments (Rad Blades 15, 40 and 60 degree, Medtronic Xomed Inc., Jacksonville, FL, USA) are introduced through this incision providing access to entire anterior wall of maxillary sinus on diseased side.
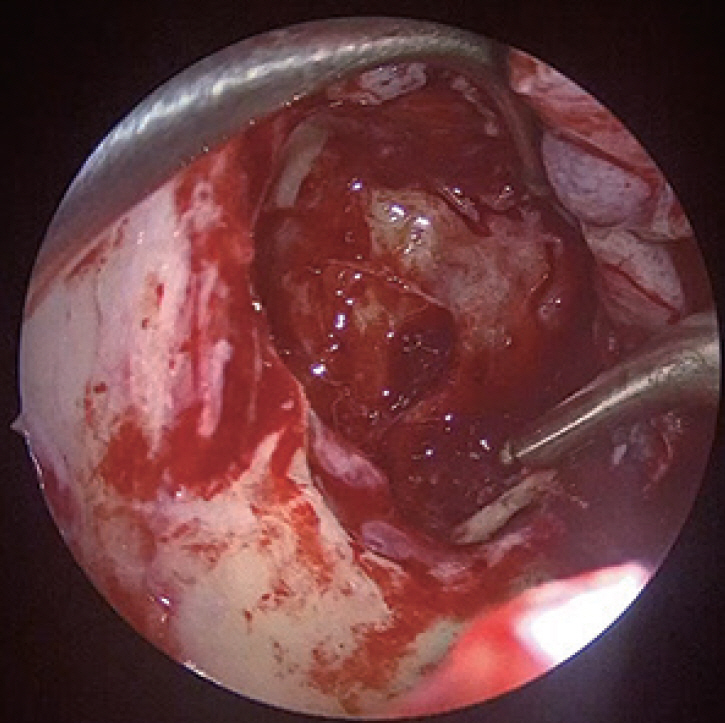
Fig. 9. Bone lying beneath tumour attachment is drilled.
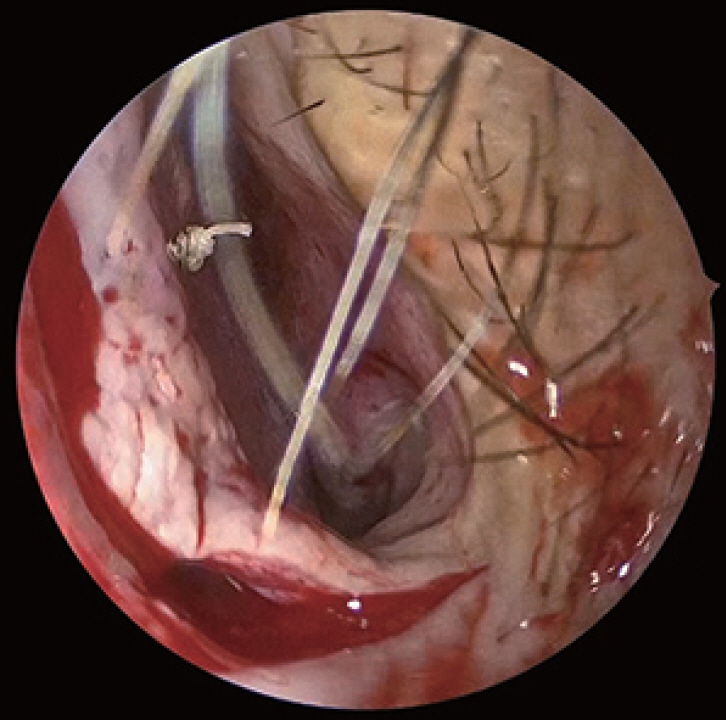
Fig. 10. The 3-0 Vicryl RapideTM (Vicryl Rapide, Ethicon, Johnson and Johnson, Piscataway, NJ, USA) with a knot at one end was used for flap suturing.
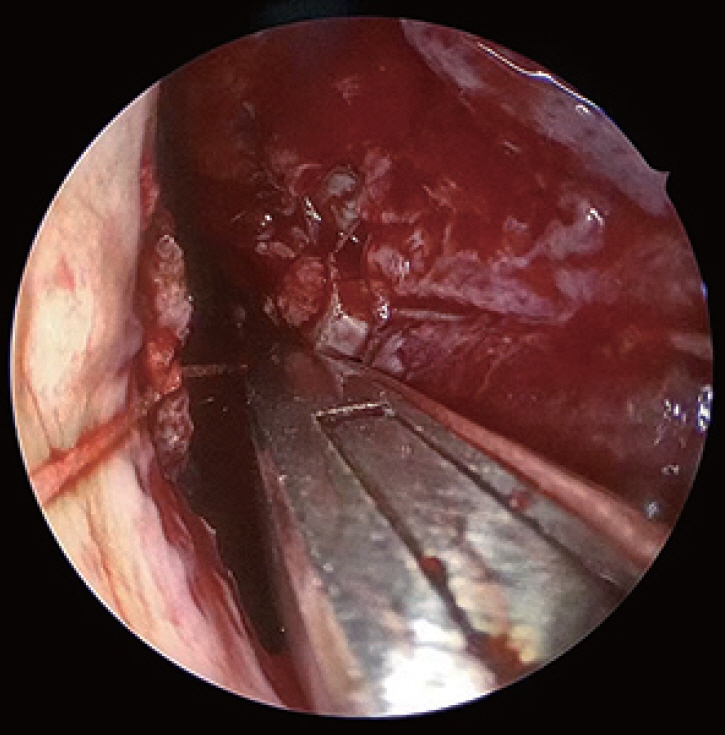
Fig. 11. Septal suturing done.
Reference
-
1. Lund VJ, Stammberger H, Nicolai P, Castelnuovo P, Beal T, Beham A, et al. European position paper on endoscopic management of tumours of the nose, paranasal sinuses and skull base. Rhinol Suppl. 2010; 22:1–143.2. Pagella F, Pusateri A, Matti E, Avato I, Zaccari D, Emanuelli E, et al. "TuNa-saving" endoscopic medial maxillectomy: a surgical technique for maxillary inverted papilloma. Eur Arch Otorhinolaryngol. 2017; 274(7):2785–91.
Article3. Morrissey DK, Wormald PJ, Psaltis AJ. Prelacrimal approach to the maxillary sinus. Int Forum Allergy Rhinol. 2016; 6(2):214–8.
Article4. Harvey RJ, Sheehan PO, Debnath NI, Schlosser RJ. Transseptal approach for extended endoscopic resections of the maxilla and infratemporal fossa. Am J Rhinol Allergy. 2009; 23(4):426–32.
Article5. Hari C, Marnane C, Wormald PJ. Quilting sutures for nasal septum. J Laryngol Otol. 2008; 122(5):522–3.
Article6. Chiu AG, Jackman AH, Antunes MB, Feldman MD, Palmer JN. Radiographic and histologic analysis of the bone underlying inverted papillomas. Laryngoscope. 2006; 116(9):1617–20.
Article7. Yu QQ, Guan G, Zhang NK, Zhang XW, Jiang Y, Lian YY, et al. Intranasal endoscopic prelacrimal recess approach for maxillary sinus inverted papilloma. Eur Arch Otorhinolaryngol. 2018; 275(9):2297–302.
Article8. Douglas R, Wormald PJ. Endoscopic surgery for juvenile nasopharyngeal angiofibroma: where are the limits? Curr Opin Otolaryngol Head Neck Surg. 2006; 14(1):1–5.
Article9. Ramakrishnan VR, Suh JD, Chiu AG, Palmer JN. Septal dislocation for endoscopic access of the anterolateral maxillary sinus and infratemporal fossa. Am J Rhinol Allergy. 2011; 25(2):128–30.
Article10. Dean NR, Illing EA, Woodworth BA. Endoscopic resection of anterolateral maxillary sinus inverted papillomas. Laryngoscope. 2015; 125(4):807–12.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prelacrimal Recess Approach for Maxillary Sinus Inverted Papilloma: Preliminary Study
- Comparison Between Endoscopic Prelacrimal Medial Maxillectomy and Caldwell-Luc Approach for Benign Maxillary Sinus Tumors
- Endoscopic Resection of Inverted Papilloma in the Maxillary Sinus - ‘Prelacrimal Approach,’ ‘Origin Site Cauterization and Drilling (Painting and Washing)’
- Comparison of Surgical Outcomes for Treatment of Maxillary Sinus Inverted Papilloma: Endoscopic Prelacrimal Recess Approach versus Caldwell-Luc Approach
- A Case of Removal of Medial Maxillary Intraosseous Hemangioma through an Intranasal Endoscopic Prelacrimal Recess Approach
