Implementation and improvement of Enhanced Recovery After Surgery protocols for colorectal cancer surgery
- Affiliations
-
- 1Division of Vascular and Transplant Surgery, Department of Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Division of Colorectal Surgery, Department of Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2527839
- DOI: http://doi.org/10.4174/astr.2022.102.4.223
Abstract
- Purpose
Enhanced Recovery After Surgery (ERAS) reduces postoperative complications and shortens hospital stays. We aimed to describe the implementation and improvement of ERAS protocols in our institution through a multidisciplinary team approach.
Methods
A multidisciplinary team comprised of colorectal surgeons, anesthesiologists, nurses, pharmacists, nutritionists, and a performance improvement team was launched to develop the ERAS protocol. The ERAS protocol was followed in patients who underwent colonic and rectal surgery between January and November 2017. The ERAS protocol comprised 22 elements in the preoperative, intraoperative, and postoperative phases. After the initial application, ERAS compliance was monitored and audited every 4–6 months and improvements made as necessary.
Results
The length of hospital stay significantly decreased after the application of the ERAS protocols for colon cancer in 2017 and 2018. And there was no significant difference in the duration of hospital stay after applying the rectal cancer ERAS protocol. Moreover, after starting the colon ERAS, there was a significant decrease in the complication rate. Since December 2017, there was a continuous increase in the colorectal ERAS clinical pathway application rate, which remained high (>90%). The patient compliance rate significantly increased between 2017 and 2018, but slightly decreased again in 2019.
Conclusion
The application and continual improvement of an ERAS protocol are crucial. Improving compliance may result in better clinical outcomes. Additionally, the basic guidelines of ERAS must be applied and developed according to each hospital’s situation based on the team approach.
Keyword
Figure
-
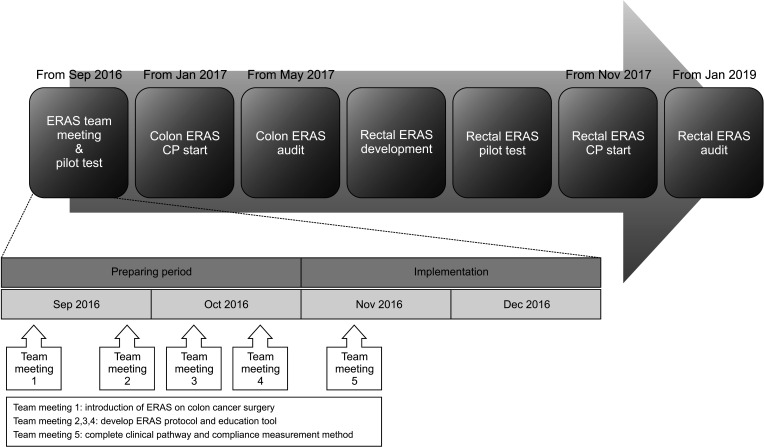
Fig. 1 The setup process for Enhanced Recovery After Surgery (ERAS) protocol. CP, clinical pathway.
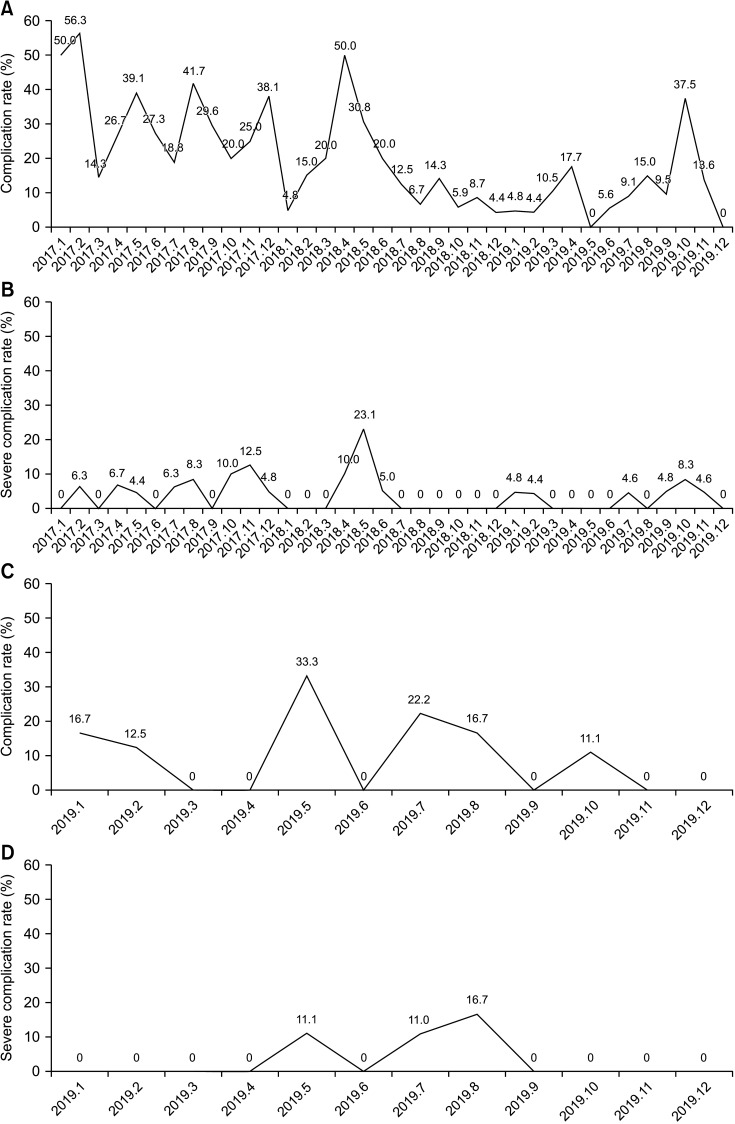
Fig. 2 (A, B) Complication rates (A) and severe complication rates (B) for colon cancer surgery after application of the Enhanced Recovery After Surgery (ERAS) protocol. (C, D) Complication rates (C) and severe complication rate (D) for rectal cancer surgery after application of the ERAS protocol.
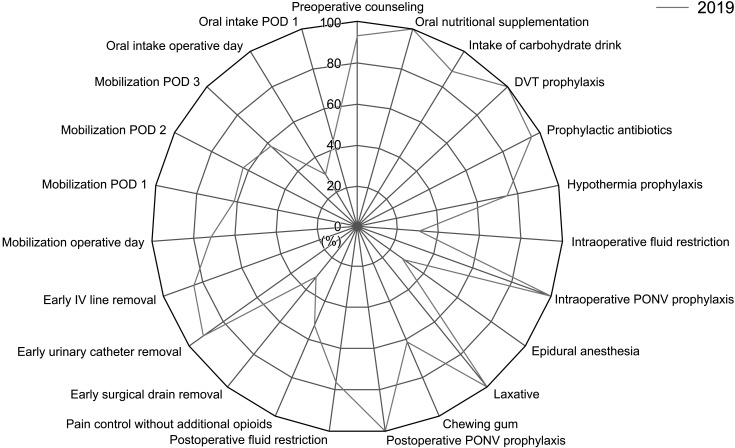
Fig. 3 Compliance rates of rectal cancer Enhanced Recovery After Surgery protocol. DVT, deep venous thrombosis; PONV, postoperative nausea and vomiting; IV, intravenous; POD, postoperative day.
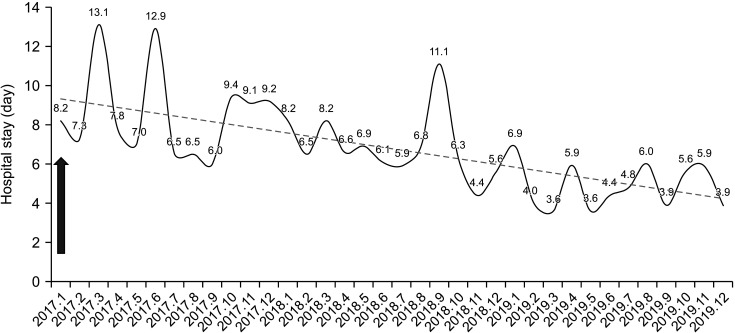
Fig. 4 Hospital stay of colon cancer surgery. Arrow indicates the start time of colon cancer Enhanced Recovery After Surgery (January 2017).
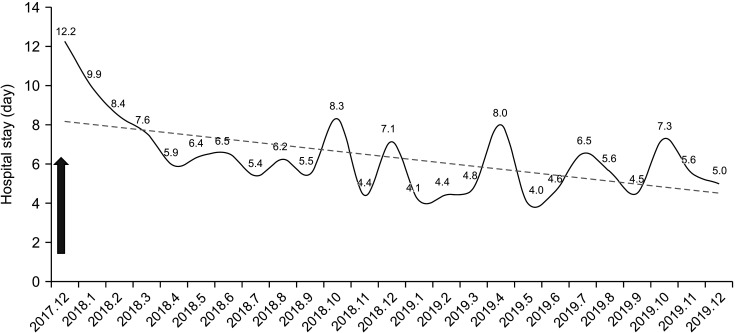
Fig. 5 Hospital stay of rectal cancer surgery. Arrow indicates the start time of rectal cancer Enhanced Recovery After Surgery (December 2017).
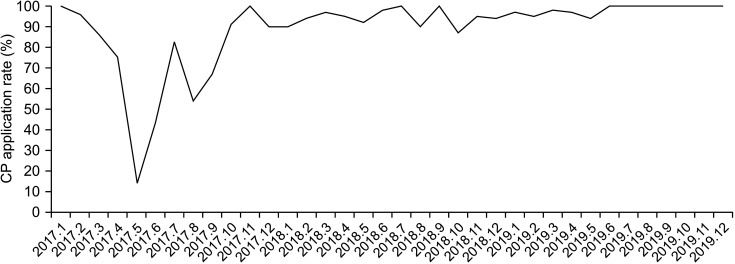
Fig. 6 Colorectal cancer Enhanced Recovery After Surgery clinical pathway (CP) application rates.
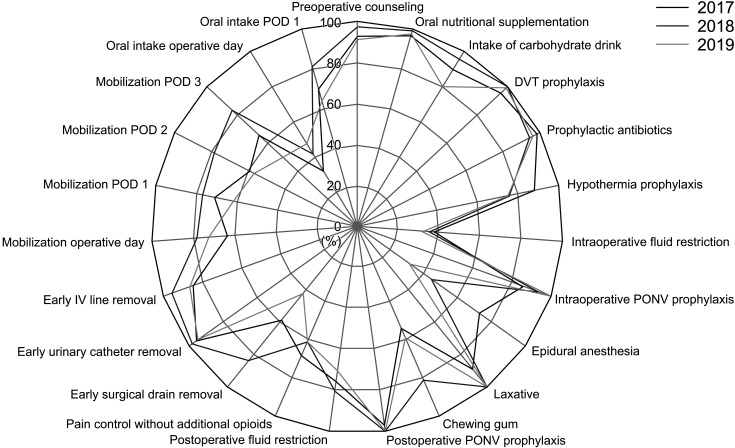
Fig. 7 Compliance rates of colon cancer Enhanced Recovery After Surgery protocol. DVT, deep venous thrombosis; PONV, postoperative nausea and vomiting; IV, intravenous; POD, postoperative day.
Cited by 1 articles
-
Challenging issues of implementing enhanced recovery after surgery programs in South Korea
Soo-Hyuk Yoon, Ho-Jin Lee
Anesth Pain Med. 2024;19(1):24-34. doi: 10.17085/apm.23096.
Reference
-
1. Wainwright TW. The quality improvement challenge: how nurses and allied health professionals can solve the knowing-doing gap in Enhanced Recovery After Surgery (ERAS). Medicina (Kaunas). 2020; 56:652.2. Jaloun HE, Lee IK, Kim MK, Sung NY, Turkistani SA, Park SM, et al. Influence of the Enhanced Recovery After Surgery protocol on postoperative inflammation and short-term postoperative surgical outcomes after colorectal cancer surgery. Ann Coloproctol. 2020; 36:264–272. PMID: 32674557.
Article3. Lee CS, Han SR, Kye BH, Bae JH, Koh W, Lee IK, et al. Surgical skin adhesive bond is safe and feasible wound closure method to reduce surgical site infection following minimally invasive colorectal cancer surgery. Ann Surg Treat Res. 2020; 99:146–152. PMID: 32908846.
Article4. Kim MK, Kim JG, Lee G, Won DD, Lee YS, Kye BH, et al. Comparison of the effects of an ERAS program and a single-port laparoscopic surgery on postoperative outcomes of colon cancer patients. Sci Rep. 2019; 9:11998. PMID: 31427651.
Article5. Koh W, Lee CS, Bae JH, Al-Sawat A, Lee IK, Jin HY. Clinical validation of implementing Enhanced Recovery After Surgery protocol in elderly colorectal cancer patients. Ann Coloproctol. 2021; 38:47–52.
Article6. Golder HJ, Papalois V. Enhanced Recovery After Surgery: history, key advancements and developments in transplant surgery. J Clin Med. 2021; 10:1634. PMID: 33921433.
Article7. Pędziwiatr M, Mavrikis J, Witowski J, Adamos A, Major P, Nowakowski M, et al. Current status of Enhanced Recovery After Surgery (ERAS) protocol in gastrointestinal surgery. Med Oncol. 2018; 35:95. PMID: 29744679.
Article8. Pisarska M, Gajewska N, Małczak P, Wysocki M, Major P, Milian-Ciesielska K, et al. Is it possible to maintain high compliance with the Enhanced Recovery After Surgery (ERAS) protocol?: a cohort study of 400 consecutive colorectal cancer patients. J Clin Med. 2018; 7:412.9. Rauwerdink A, Jansen M, de Borgie CA, Bemelman WA, Daams F, Schijven MP, et al. Improving Enhanced Recovery After Surgery (ERAS): ERAS APPtimize study protocol, a randomized controlled trial investigating the effect of a patient-centred mobile application on patient participation in colorectal surgery. BMC Surg. 2019; 19:125. PMID: 31477107.
Article10. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations: 2018. World J Surg. 2019; 43:659–695. PMID: 30426190.
Article11. Carmichael JC, Keller DS, Baldini G, Bordeianou L, Weiss E, Lee L, et al. Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American Society of Colon and Rectal Surgeons and Society of American Gastrointestinal and Endoscopic Surgeons. Dis Colon Rectum. 2017; 60:761–784. PMID: 28682962.
Article12. Wei IH, Pappou EP, Smith JJ, Widmar M, Nash GM, Weiser MR, et al. Monitoring an ongoing Enhanced Recovery After Surgery (ERAS) Program: adherence improves clinical outcomes in a comparison of three thousand colorectal cases. Clin Surg. 2020; 5:2909. PMID: 33163851.13. Ripollés-Melchor J, Ramírez-Rodríguez JM, Casans-Francés R, Aldecoa C, Abad-Motos A, Logroño-Egea M, et al. Association between use of Enhanced Recovery After Surgery protocol and postoperative complications in colorectal surgery: the Postoperative Outcomes Within Enhanced Recovery After Surgery Protocol (POWER) Study. JAMA Surg. 2019; 154:725–736. PMID: 31066889.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical outcomes and future directions of enhanced recovery after surgery in colorectal surgery: a narrative review
- Which patients with gastric cancer should be candidates for Enhanced Recovery After Surgery protocols?
- Enhanced recovery after surgery: importance of compliance audits
- Standardizing the Protocols for Enhanced Recovery From Colorectal Cancer Surgery: Are We a Step Closer to Ideal Recovery?
- Diet Modification Based on the Enhanced Recovery After Surgery Program (ERAS) in Patients Undergoing Laparoscopic Colorectal Resection
