Acute Pulmonary Embolism and Chronic Thromboembolic Pulmonary Hypertension: Clinical and Serial CT Pulmonary Angiographic Features
- Affiliations
-
- 1Department of Radiology, Samsung ChangWon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea
- 2Department of Radiology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- 3Division of Cardiology, Cardiac and Vascular Center, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2526983
- DOI: http://doi.org/10.3346/jkms.2022.37.e76
Abstract
- In acute pulmonary embolism (PE), circulatory failure and systemic hypotension are important clinically for predicting poor prognosis. While pulmonary artery (PA) clot loads can be an indicator of the severity of current episode of PE or treatment effectiveness, they may not be used directly as an indicator of right ventricular (RV) failure or patient death. In other words, pulmonary vascular resistance or patient prognosis may not be determined only with mechanical obstruction of PAs and their branches by intravascular clot loads on computed tomography pulmonary angiography (CTPA), but determined also with vasoactive amines, reflex PA vasoconstriction, and systemic arterial hypoxemia occurring during acute PE. Large RV diameter with RV/left ventricle (LV) ratio > 1.0 and/or the presence of occlusive clot and pulmonary infarction on initial CTPA, and clinically determined high baseline PA pressure and RV dysfunction are independent predictors of oncoming chronic thromboembolic pulmonary hypertension (CTEPH). In this pictorial review, authors aimed to demonstrate clinical and serial CTPA features in patients with acute massive and submassive PE and to disclose acute CTPA and clinical features that are related to the prediction of oncoming CTEPH.
Keyword
Figure
-
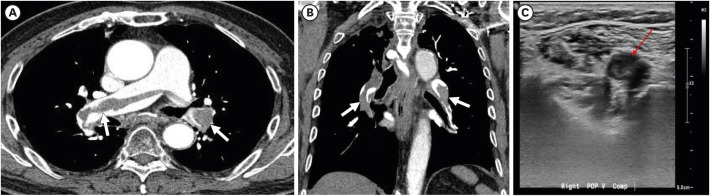
Fig. 1 Acute pulmonary embolism in a 79-year-old man who has deep vein thrombosis. (A) Transverse image of enhanced CT scan obtained at level of bronchus intermedius demonstrates filling defects in a linear manner in proximal right pulmonary and interlobar artery and also in proximal left lower lobar arteries (arrows). (B) Coronal reformatted image depicts filling defects (arrows) in right interlobar and lower lobar and left lower lobar arteries with so-called railway-track sign. (C) Ultrasonography obtained at right popliteal vein discloses isoechoic recently-developed deep vein thrombosis (thin red arrow).
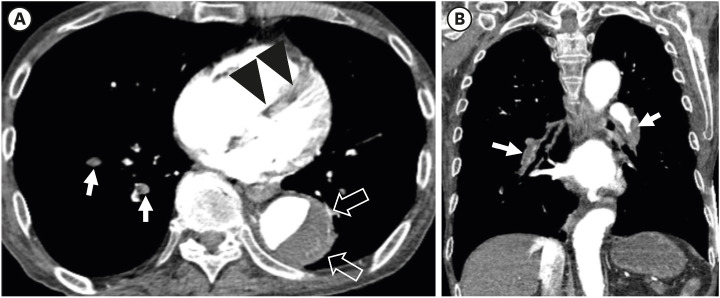
Fig. 2 Triple-rule-out technique showing acute massive pulmonary embolism and aortic dissection simultaneously in a 73-year-old man. (A) Transverse image of enhanced CT scan obtained at level segmental bronchi of lower lobes demonstrates filling defects in a linear manner in segmental right lower lobar arteries (arrows). Also note flattening of interventricular septum (arrowheads) reflecting the presence of right ventricular strain, and aortic dissection (open arrows) in descending thoracic aorta. (B) Coronal reformatted image depicts filling defects (arrows) in right lower lobar and proximal left lower lobar arteries. Note both lower lobar arteries are completely occluded with emboli. Patient showed hypotension and died of the disease. Laboratory test results were as follows: ProBNP, 2,261 pg/mL (normal, 125–450 pg/mL) and Troponin-I, 0.0839 ng/mL (normal, below 0.04 ng/mL). Initially, the mortality risk was classified into high group in this patient.
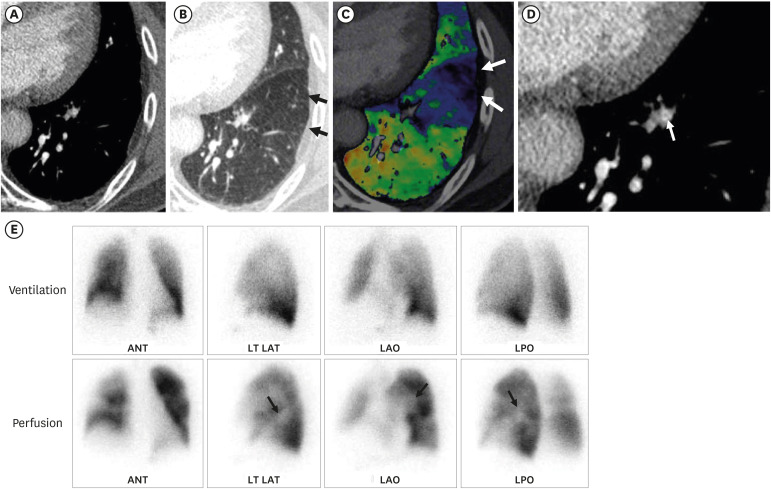
Fig. 3 Segmental pulmonary embolism detected with dual-energy CT in a 67-year-old man with chronic thromboembolic pulmonary hypertension. (A) Transverse image of CT scan obtained at level of left ventricle shows no identifiable filling defect in left lower lobe. (B, C) Lung window (B) and color-coded (C) images of CT scan obtained at same level to (A) demonstrate mosaic attenuation of triangular shape (arrows in B) and perfusion defect on color-coded image (arrows in C) within same pulmonary segment to (A), suggesting possible presence of segmental embolism. (D) After reviewing CT pulmonary angiography and color-coded iodine map images, presence of segmental pulmonary embolism was considered in retrospect especially on magnified view of transverse image showing partially occlusive thrombi as intraluminal “bands” within anterior basal segmental artery of the left lower pulmonary artery (arrow). (E) Corresponding ventilation (upper row) and perfusion (lower row) scintigraphy with multiplanar imaging (from left to right: anterior, left lateral, left anterior oblique and left posterior oblique views) showing V/Q mismatch (perfusion defects) within left lower lobe (arrows).CT = computed tomography, ANT = anterior, LT LAT = left lateral, LAO = left anterior oblique, LPO = left posterior oblique.
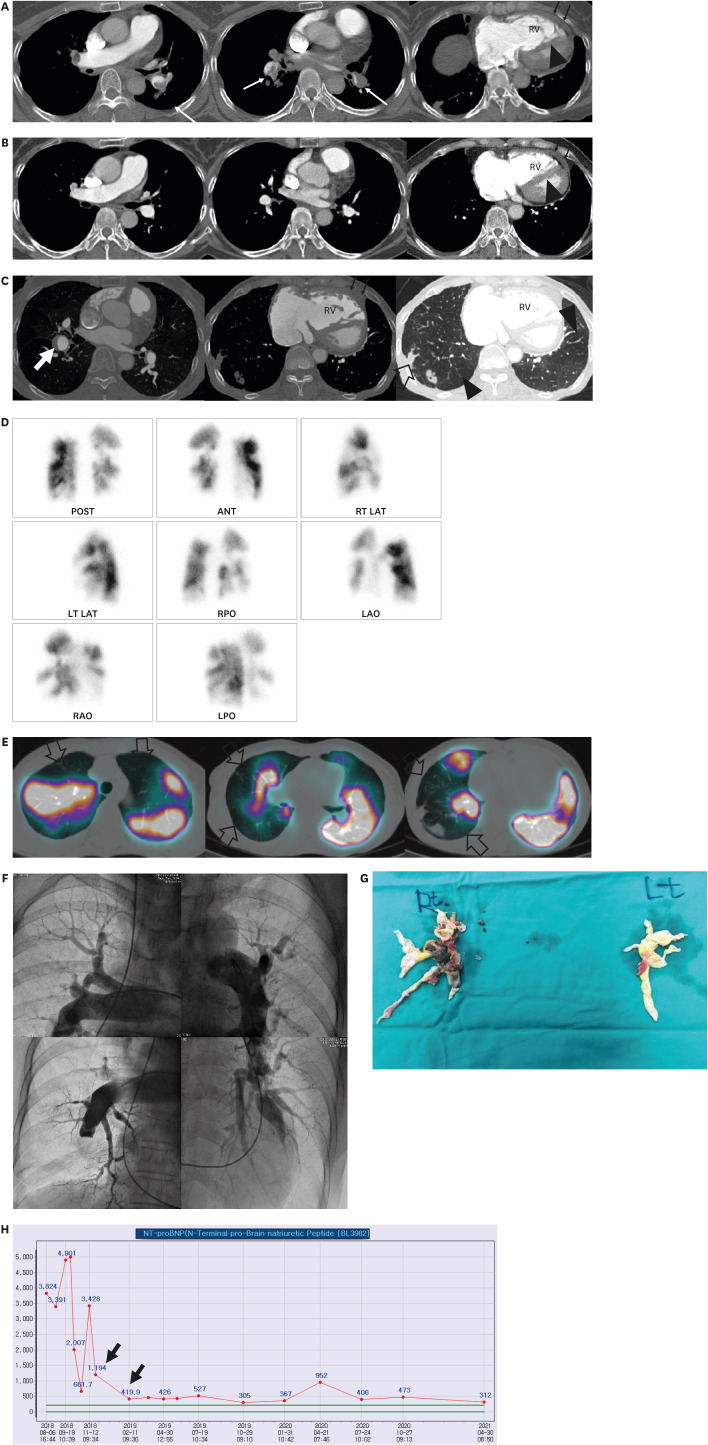
Fig. 4 Evolution of acute submassive pulmonary embolism to chronic thromboembolic pulmonary hypertension in a 70-year-old woman. (A) Consecutive transverse enhanced CT scans obtained in January 2012 show filling defects (arrows) in bilateral pulmonary arteries and their branches. Please note occlusive defect in left lower lobar artery (arrow in second Fig.). Also note larger RV than LV (RV/LV ratio, 1.20), flattening of interventricular septum (arrowhead) and thickened RV free wall (thin arrows, measuring up to 7 mm). Short axis of RV is measured from inner wall to inner wall where tricuspid valve is scanned, whereas short axis of left ventricle is measured from inner wall to inner wall where mitral valve is scanned. Among related factors of oncoming CTEPH, the patient showed RV dysfunction with RV/LV ratio greater than 1.0 when diagnosed with acute PE. (B) CT scans obtained in March 2012 demonstrate that all emboli have resolved completely. But please note again enlarged RV, thickened RV free wall (thin arrows), and flattened interventricular septum (arrowhead). (C) Mixed lung and mediastinal window images obtained in August 2018 depict evolution into chronic thromboembolic pulmonary hypertension. Please note enlarged lobar and segmental pulmonary arteries, unusually tortuous branch arteries, eccentric embolus in right lower lobar artery (arrow), large areas (arrowheads) of mosaic perfusion, and pulmonary infarction areas (open arrow). Also note enlarged RV and its thickened anterior free wall (thin arrows), and flattened interventricular septum. (D) Perfusion scintigraphy with multiplanar imaging obtained at similar time to (C) displays multifocal areas of perfusion defects in both lungs, typical features that can be seen in chronic thromboembolic pulmonary hypertension. (E) Dual-energy CT and its color-coded perfusion map images obtained in August 2018 before thromboendarterectomy clearly show multifocal areas of perfusion defects (open arrows) in both lungs, features well matched with prior perfusion scintigraphy (D). (F) Digital subtraction angiography obtained in August 2018 before thromboendarterectomy demonstrates pruned-tree appearance of pulmonary vasculature and multifocal areas of non-perfused lung areas. (G) Gross pathologic specimens depict pulmonary thromboendarterectomy byproducts which had filled pulmonary vessels heading toward non-perfused lung areas. (H) Serial measurements of NT-proBNP level before and after thromboendarterectomy display sharp decline (arrows) of its level after surgical procedures.RV = right ventricle, POST = posterior, ANT = anterior, RT LAT right lateral, LT LAT = left lateral, RPO = right posterior oblique, LAO = left anterior oblique, RAO = right anterior oblique, LPO = left posterior oblique, NT-proBNP = N-terminal pro-brain natriuretic peptide, CT = computed tomography.
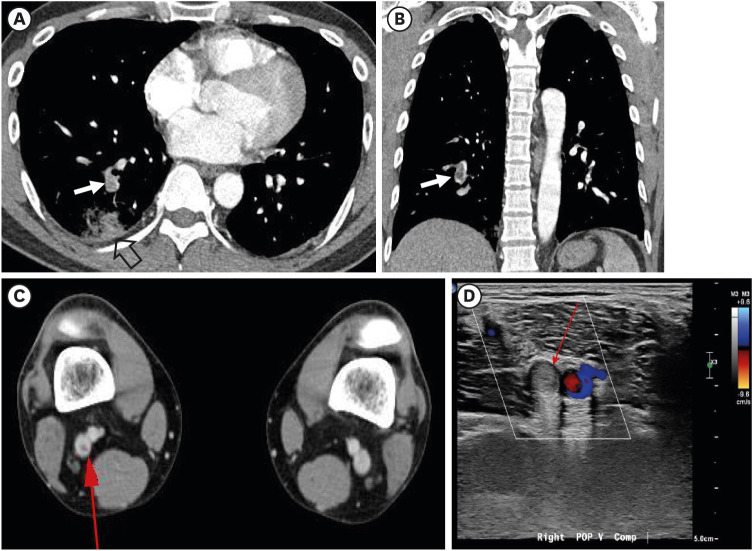
Fig. 5 Acute pulmonary embolism and deep vein thrombosis detected with CT pulmonary angiography and indirect CT venography, respectively, in a 38-year-old man complaining of right flank pain. (A) Enhanced transverse CT scan obtained at level of segmental arteries shows a filling defect (arrow) in right posterior basal segmental artery. Also note segmental consolidation (open arrow) representing bland infarction in posterior basal segment of right lower lobe, related to embolism. (B) Coronal reformatted image also demonstrates filling defect (arrow) in posterior basal segmental artery. (C) Indirect CT venography obtained two minutes after contrast medium injection demonstrate filling defect (thin arrow) in right popliteal vein. (D) Color-Doppler ultrasonography depicts deep vein thrombosis (thin arrow) in right popliteal vein.CT = computed tomography.
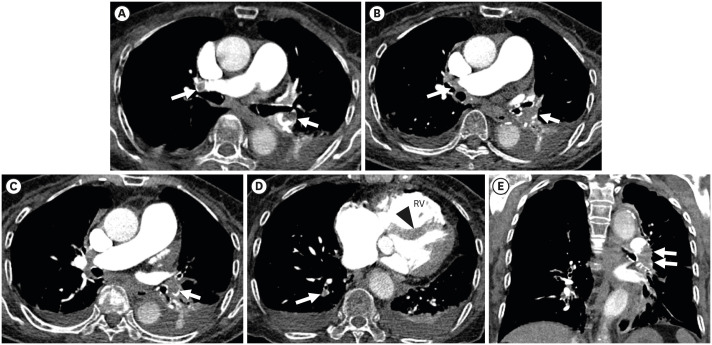
Fig. 6 Submassive and acute pulmonary embolism in an 87-year-old woman complaining of dyspnea. (A) Transverse image of enhanced CT scans obtained at level of upper lobar bronchus demonstrates filling defects in a linear manner in right proximal interlobar artery and left lower lobar artery (arrow). (B) CT scan obtained at cardiac ventricular level depicts leftward bowing (arrowhead) of interventricular septum suggesting presence of right ventricular strain. Also note enlarged RV. Pulmonary embolism is also present in posterior basal segmental artery (arrow). Pleural effusions are associated bilaterally (C, D). (E) Coronal reformatted image discloses filling defect (arrows) occluding left lower lobar artery. Laboratory test results were as follows: ProBNP, 6,758 pg/mL (normal, 125–450 pg/mL) and Troponin-I, 0.2495 ng/mL (normal, below 0.04 ng/mL). Initial vital signs were stable except peripheral and arterial oxygen saturation were slightly lower. The patient underwent echocardiography and it showed moderate to severe RV dysfunction. The mortality risk was classified into intermediate group.RV = right ventricle, CT = computed tomography.
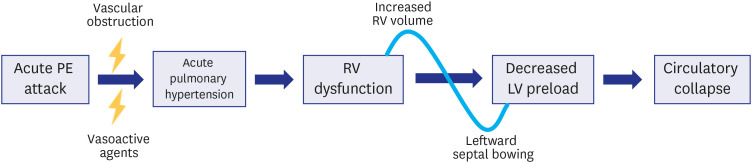
Fig. 7 Diagram explaining cascade events from acute massive pulmonary embolism to systemic hypotension and circulatory collapse. With massive emboli, vascular obstruction and related vasoactive agents cause acute pulmonary hypertension which leads to morphologic changes of right ventricular volume and leftward interventricular septal bowing and right ventricular dysfunction. Decreased venous return due to right ventricular dysfunction and decreased left ventricular volume related to interventricular septal bowing elicit decreased left ventricular preload and resultant circulatory collapse (Modified from reference 26: Ghaye et al. Radiographics 2006; 26: 23-39).PE = pulmonary embolism, RV = right ventricle, LV = left ventricle.
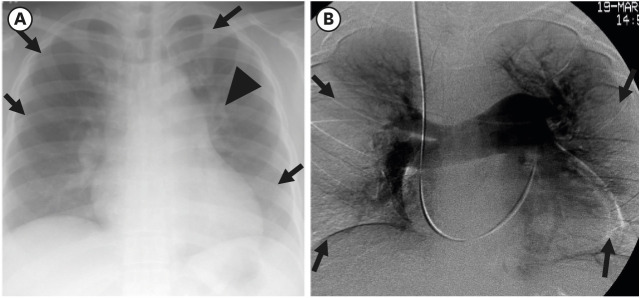
Fig. 8 Chest radiographic and DSA pulmonary angiography explaining unusual pulmonary vascularity and asymmetric pulmonary hypoperfusion in a 58-year-old woman having chronic thromboembolic pulmonary hypertension. (A) Chest radiograph shows enlarged bilateral hila and unusually tortuous and prominent left upper lobar arteries (arrowheads). Also note pulmonary oligemia in right upper and middle lung zone and left upper and lower lung zones (arrows). Cardiomegaly is also seen with right ventricular enlargement (elevated left lower cardiac border). (B) DSA pulmonary angiography depicts absent pulmonary perfusion (arrows) in bilateral middle and lower lung zones owing to vascular occlusion with chronic emboli.DSA = digital subtraction angiographic.
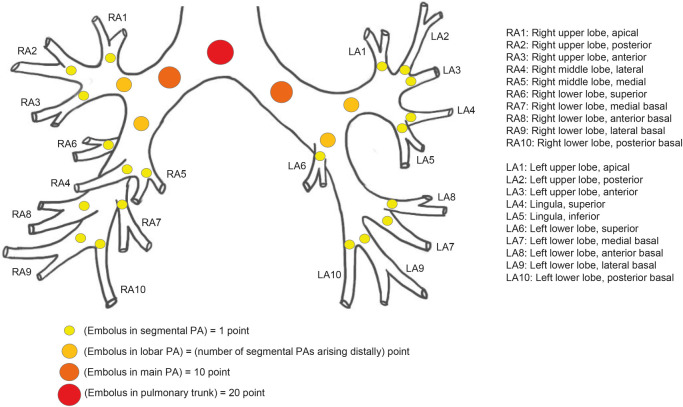
Fig. 9 Schematic diagram of Qanadli scoring system of acute pulmonary embolism. To quantify arterial obstruction in pulmonary embolism (percentage of vascular obstruction on CT scans), Qanadli et al. proposed new CT index using following simple formula; Σ(n · d) / 40 × 100), where n is value of proximal thrombus in pulmonary arterial tree equal to number of segmental branches arising distally (minimum, 1; maximum, 20). And d is a kind of weighing factor depending on degree of obstruction (no thrombus, 0; partially occluded, 1; total occlusion, 2). For example, when pulmonary trunk is completely occluded, the score is 40 (maximum score; 20 point by weighing factor 2) and it is like complete occlusion of bilateral main pulmonary artery (10 point by weighing factor 2 by two main arteries). Right upper lobar artery supplies three segmental arteries, whereas left upper lobar artery supplies five segmental arteries. In contrast, right lower lobar artery covers seven segmental arteries, whereas left lower lobar artery covers five segmental arteries (Schema drawn in consideration of descriptive text from reference 39: Qanadli et al. AJR Am J Roentgenol 2001; 176: 1415-1420).RA = right atrial, LA = left atrial, PA = pulmonary artery, CT = computed tomography.

Fig. 10 Repeated attacks of acute pulmonary embolism without evolving into chronic thromboembolic pulmonary hypertension in a 72-year-old woman. (A, B) Transverse images of enhanced CT scans obtained at levels of bronchus intermedius (A) and right middle lobar bronchus take-off (B), respectively, and in January 2012, demonstrate filling defects in right proximal interlobar artery (arrow in A) and in bilateral lower lobar arteries (arrows in B). (C) Coronal reformatted image depicts filling defects in bilateral lower lobar arteries with railway-track sign (arrows). (D, E) Transverse images of enhanced CT scans obtained at levels of left inferior pulmonary vein (A) and subsegmental bronchi (B), respectively, and in November 2018, disclose filling defects in posterolateral basal trunk of right lower lobar pulmonary artery and anteromedial segmental artery of left lower lobe (arrows in D) and posterior basal segmental artery of right lower lobe and anteromedial basal segmental artery of left lower lobe (arrows in E). Between repeated attacks of pulmonary embolism, complete dissolution of emboli has been achieved with embolotherapy. Please note that even with repeated attacks of acute pulmonary embolism, chronic thromboembolic pulmonary hypertension features could not be seen on this follow-up CT. Chronic thromboembolic pulmonary hypertension has not occurred yet as of September 2021. None of the related clinical and CTPA features was related to the evolution to chronic thromboembolic pulmonary hypertension after acute embolic attack. Patient had no deep vein thrombosis; RV/LV ratio was lesser than 1.0 on CTPA; normal RV function on echocardiography; and absence of mosaic attenuation or lung infarction on CTPA.CT = computed tomography, CTPA = CT pulmonary angiography, RV = right ventricle, LV = left ventricle.
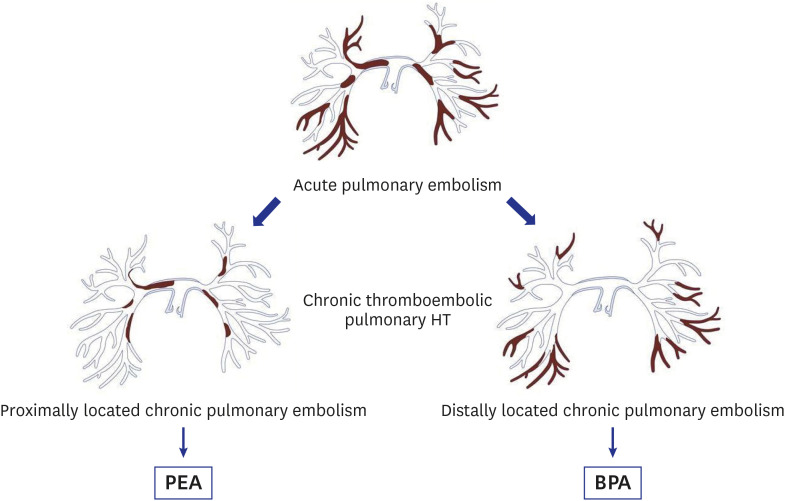
Fig. 11 Flowsheet for management of chronic thromboembolic pulmonary hypertension.When occlusive lesions are located centrally and patient condition is acceptable for surgery, PEA is performed. When occlusive lesions are mainly located peripherally, BPA is considered management method.HT = hypertension, PEA = pulmonary endarterectomy, BPA = balloon pulmonary angioplasty.
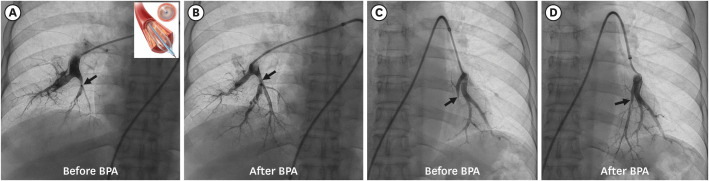
Fig. 12 Successful BPA for chronic thromboembolic pulmonary hypertension in a 71-year-old woman. (A) Right basal trunk pulmonary angiography shows web-like narrowing (arrow) of medial basal segmental artery of right lower lobe. Inset: balloon angioplasty device. (B) Follow-up angiography after angioplasty demonstrates narrowed segment is dilated with maintained arterial lumen (arrow). (C) Left basal trunk pulmonary angiography shows near complete occlusion (arrow) of medial basal branch artery of left lower lobe. (D) Follow-up angiography after angioplasty demonstrates occluded segmental lumen is penetrated and opened (arrow).BPA = balloon pulmonary angioplasty.
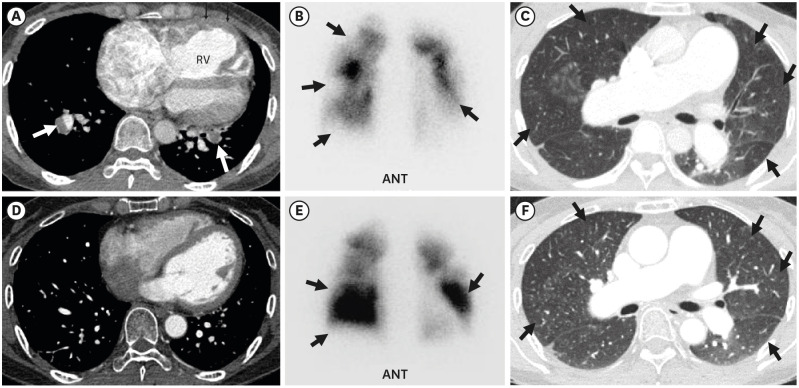
Fig. 13 Imaging features before and after balloon pulmonary angioplasty in a 56-year-old woman having chronic thromboembolic pulmonary hypertension. (A) Transverse image of enhanced CT scan obtained at basal segmental pulmonary artery level shows filling defects (arrows) in basal segmental arteries. Also note flattening of interventricular septum, RV enlargement, and RV wall thickening (small arrows). (B) Anterior view of perfusion scintigraphy demonstrates multiple areas (arrows)of perfusion defects in both lungs. (C) Lung window of CT scan obtained at distal main bronchus level depicts multiple areas (arrows) of perfusion deficiency and/or oligemia. Please compare lung attenuation and vascularity of this image with those of (F) (after balloon angioplasty). (D) Follow-up CT scan obtained at similar level to (A) shows reversal of interventricular septal morphology with normal right-sided bowing. Also note absence of filling defect in segmental pulmonary arteries. (E) Anterior view of follow-up perfusion scintigraphy after balloon angioplasty demonstrates perfusion improvement (arrows) particularly in lower lung zones. (F) Lung window of follow-up CT scan obtained at similar level to (C) and after balloon angioplasty depicts improved perfusion and vascularity (arrows) in bilateral lungs. Please compare perfusion and vascularity with those of (C).ANT = anterior, RV = right ventricle, CT = computed tomography.
Reference
-
1. Carson JL, Kelley MA, Duff A, Weg JG, Fulkerson WJ, Palevsky HI, et al. The clinical course of pulmonary embolism. N Engl J Med. 1992; 326(19):1240–1245. PMID: 1560799.
Article2. Mayo J, Thakur Y. Pulmonary CT angiography as first-line imaging for PE: image quality and radiation dose considerations. AJR Am J Roentgenol. 2013; 200(3):522–528. PMID: 23436840.
Article3. Mayo J, Thakur Y. Acute pulmonary embolism: from morphology to function. Semin Respir Crit Care Med. 2014; 35(1):41–49. PMID: 24481758.
Article4. Remy-Jardin M, Pistolesi M, Goodman LR, Gefter WB, Gottschalk A, Mayo JR, et al. Management of suspected acute pulmonary embolism in the era of CT angiography: a statement from the Fleischner Society. Radiology. 2007; 245(2):315–329. PMID: 17848685.
Article5. Halpern EJ. Triple-rule-out CT angiography for evaluation of acute chest pain and possible acute coronary syndrome. Radiology. 2009; 252(2):332–345. PMID: 19703877.
Article6. Weikert T, Winkel DJ, Bremerich J, Stieltjes B, Parmar V, Sauter AW, et al. Automated detection of pulmonary embolism in CT pulmonary angiograms using an AI-powered algorithm. Eur Radiol. 2020; 30(12):6545–6553. PMID: 32621243.
Article7. Soffer S, Klang E, Shimon O, Barash Y, Cahan N, Greenspana H, et al. Deep learning for pulmonary embolism detection on computed tomography pulmonary angiogram: a systematic review and meta-analysis. Sci Rep. 2021; 11(1):15814. PMID: 34349191.
Article8. Fedullo P, Kerr KM, Kim NH, Auger WR. Chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med. 2011; 183(12):1605–1613. PMID: 21330453.
Article9. Tunariu N, Gibbs SJ, Win Z, Gin-Sing W, Graham A, Gishen P, et al. Ventilation-perfusion scintigraphy is more sensitive than multidetector CTPA in detecting chronic thromboembolic pulmonary disease as a treatable cause of pulmonary hypertension. J Nucl Med. 2007; 48(5):680–684. PMID: 17475953.
Article10. Wang M, Wu D, Ma R, Zhang Z, Zhang H, Han K, et al. Comparison of V/Q SPECT and CT angiography for the diagnosis of chronic thromboembolic pulmonary hypertension. Radiology. 2020; 296(2):420–429. PMID: 32427559.
Article11. Hong YJ, Shim J, Lee SM, Im DJ, Hur J. Dual-energy CT for pulmonary embolism: current and evolving clinical applications. Korean J Radiol. 2021; 22(9):1555–1568. PMID: 34448383.
Article12. Im DJ, Hur J, Han K, Suh YJ, Hong YJ, Lee HJ, et al. Prognostic value of dual-energy CT-based iodine quantification versus conventional CT in acute pulmonary embolism: a propensity-match analysis. Korean J Radiol. 2020; 21(9):1095–1103. PMID: 32691545.
Article13. Zhang LJ, Chai X, Wu SY, Zhao YE, Hu XB, Hu YX, et al. Detection of pulmonary embolism by dual energy CT: correlation with perfusion scintigraphy and histopathological findings in rabbits. Eur Radiol. 2009; 19(12):2844–2854. PMID: 19657658.
Article14. Boroto K, Remy-Jardin M, Flohr T, Faivre JB, Pansini V, Tacelli N, et al. Thoracic applications of dual-source CT technology. Eur J Radiol. 2008; 68(3):375–384. PMID: 18929452.
Article15. Fink C, Johnson TR, Michaely HJ, Morhard D, Becker C, Reiser M, et al. Dual-energy CT angiography of the lung in patients with suspected pulmonary embolism: initial results. RoFo Fortschr Geb Rontgenstr Nuklearmed. 2008; 180(10):879–883. PMID: 19238637.
Article16. Pontana F, Faivre JB, Remy-Jardin M, Flohr T, Schmidt B, Tacelli N, et al. Lung perfusion with dual-energy multidetector-row CT (MDCT): feasibility for the evaluation of acute pulmonary embolism in 117 consecutive patients. Acad Radiol. 2008; 15(12):1494–1504. PMID: 19000866.17. Henzler T, Fink C, Schoenberg SO, Schoepf UJ. Dual-energy CT: radiation dose aspects. AJR Am J Roentgenol. 2012; 199(5):Suppl. S16–S25. PMID: 23097163.
Article18. Ciccotosto C, Goodman LR, Washington L, Quiroz FA, Indirect CT. Indirect CT venography following CT pulmonary angiography: spectrum of CT findings. J Thorac Imaging. 2002; 17(1):18–27. PMID: 11828208.19. Yavas US, Calisir C, Ozkan IR. The interobserver agreement between residents and experienced radiologists for detecting pulmonary embolism and DVT with using CT pulmonary angiography and indirect CT venography. Korean J Radiol. 2008; 9(6):498–502. PMID: 19039265.
Article20. Kulkarni NM, Sahani DV, Desai GS, Kalva SP. Indirect computed tomography venography of the lower extremities using single-source dual-energy computed tomography: advantage of low-kiloelectron volt monochromatic images. J Vasc Interv Radiol. 2012; 23(7):879–886. PMID: 22633619.
Article21. Ma CL, Chen XX, Lei YX, Zhang XR, Jia YJ, Tian X, et al. Clinical value of dual-energy spectral imaging with adaptive statistical iterative reconstruction for reducing contrast medium dose in CT portal venography: in comparison with standard 120-kVp imaging protocol. Br J Radiol. 2016; 89(1062):20151022. PMID: 27031376.
Article22. Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011; 123(16):1788–1830. PMID: 21422387.
Article23. Sista AK, Kuo WT, Schiebler M, Madoff DC. Stratification, imaging, and management of acute massive and submassive pulmonary embolism. Radiology. 2017; 284(1):5–24. PMID: 28628412.
Article24. Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002; 121(3):877–905. PMID: 11888976.25. Belenkie I, Dani R, Smith ER, Tyberg JV. The importance of pericardial constraint in experimental pulmonary embolism and volume loading. Am Heart J. 1992; 123(3):733–742. PMID: 1539525.
Article26. Ghaye B, Ghuysen A, Bruyere PJ, D'Orio V, Dondelinger RF. Can CT pulmonary angiography allow assessment of severity and prognosis in patients presenting with pulmonary embolism? What the radiologist needs to know. Radiographics. 2006; 26(1):23–39. PMID: 16418240.
Article27. Aujesky D, Obrosky DS, Stone RA, Auble TE, Perrier A, Cornuz J, et al. Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med. 2005; 172(8):1041–1046. PMID: 16020800.
Article28. Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014; 35(43):3033–3069. PMID: 25173341.29. Renard B, Remy-Jardin M, Santangelo T, Faivre JB, Tacelli N, Remy J, et al. Dual-energy CT angiography of chronic thromboembolic disease: can it help recognize links between the severity of pulmonary arterial obstruction and perfusion defects? Eur J Radiol. 2011; 79(3):467–472. PMID: 20488639.
Article30. Roberge G, Carrier M. How to manage patients with symptomatic subsegmental pulmonary embolism? Pol Arch Intern Med. 2020; 130(4):310–316. PMID: 32091505.
Article31. Yoo HH, Marin FL. Isolated subsegmental pulmonary embolism: current therapeutic challenges. Pol Arch Intern Med. 2020; 130(11):986–991. PMID: 32426959.32. Ekici M, Ekici A, İleri Ş. Chronic CT features in PE patients with co-existing DVT. Am J Emerg Med. 2021; 46:126–131. PMID: 33744749.
Article33. Alias S, Redwan B, Panzenboeck A, Winter MP, Schubert U, Voswinckel R, et al. Defective angiogenesis delays thrombus resolution: a potential pathogenetic mechanism underlying chronic thromboembolic pulmonary hypertension. Arterioscler Thromb Vasc Biol. 2014; 34(4):810–819. PMID: 24526692.34. King MA, Ysrael M, Bergin CJ. Chronic thromboembolic pulmonary hypertension: CT findings. AJR Am J Roentgenol. 1998; 170(4):955–960. PMID: 9530043.
Article35. Chan AL, Juarez MM, Shelton DK, MacDonald T, Li CS, Lin TC, et al. Novel computed tomographic chest metrics to detect pulmonary hypertension. BMC Med Imaging. 2011; 11(1):7. PMID: 21447184.
Article36. Lin FY, Devereux RB, Roman MJ, Meng J, Jow VM, Jacobs A, et al. Cardiac chamber volumes, function, and mass as determined by 64-multidetector row computed tomography: mean values among healthy adults free of hypertension and obesity. JACC Cardiovasc Imaging. 2008; 1(6):782–786. PMID: 19356515.
Article37. Ascha M, Renapurkar RD, Tonelli AR. A review of imaging modalities in pulmonary hypertension. Ann Thorac Med. 2017; 12(2):61–73. PMID: 28469715.
Article38. Bankier AA, Janata K, Fleischmann D, Kreuzer S, Mallek R, Frossard M, et al. Severity assessment of acute pulmonary embolism with spiral CT: evaluation of two modified angiographic scores and comparison with clinical data. J Thorac Imaging. 1997; 12(2):150–158. PMID: 9179827.39. Qanadli SD, El Hajjam M, Vieillard-Baron A, Joseph T, Mesurolle B, Oliva VL, et al. New CT index to quantify arterial obstruction in pulmonary embolism: comparison with angiographic index and echocardiography. AJR Am J Roentgenol. 2001; 176(6):1415–1420. PMID: 11373204.40. Mastora I, Remy-Jardin M, Masson P, Galland E, Delannoy V, Bauchart JJ, et al. Severity of acute pulmonary embolism: evaluation of a new spiral CT angiographic score in correlation with echocardiographic data. Eur Radiol. 2003; 13(1):29–35. PMID: 12541107.
Article41. van der Meer RW, Pattynama PM, van Strijen MJ, van den Berg-Huijsmans AA, Hartmann IJ, Putter H, et al. Right ventricular dysfunction and pulmonary obstruction index at helical CT: prediction of clinical outcome during 3-month follow-up in patients with acute pulmonary embolism. Radiology. 2005; 235(3):798–803. PMID: 15845793.
Article42. Wu AS, Pezzullo JA, Cronan JJ, Hou DD, Mayo-Smith WW. CT pulmonary angiography: quantification of pulmonary embolus as a predictor of patient outcome--initial experience. Radiology. 2004; 230(3):831–835. PMID: 14739314.
Article43. Collomb D, Paramelle PJ, Calaque O, Bosson JL, Vanzetto G, Barnoud D, et al. Severity assessment of acute pulmonary embolism: evaluation using helical CT. Eur Radiol. 2003; 13(7):1508–1514. PMID: 12835961.
Article44. Ghaye B, Ghuysen A, Willems V, Lambermont B, Gerard P, D’Orio V, et al. Severe pulmonary embolism:pulmonary artery clot load scores and cardiovascular parameters as predictors of mortality. Radiology. 2006; 239(3):884–891. PMID: 16603659.
Article45. Araoz PA, Gotway MB, Trowbridge RL, Bailey RA, Auerbach AD, Reddy GP, et al. Helical CT pulmonary angiography predictors of in-hospital morbidity and mortality in patients with acute pulmonary embolism. J Thorac Imaging. 2003; 18(4):207–216. PMID: 14561905.
Article46. Lualdi JC, Goldhaber SZ. Right ventricular dysfunction after acute pulmonary embolism: pathophysiologic factors, detection, and therapeutic implications. Am Heart J. 1995; 130(6):1276–1282. PMID: 7484782.
Article47. Smulders YM. Pathophysiology and treatment of haemodynamic instability in acute pulmonary embolism: the pivotal role of pulmonary vasoconstriction. Cardiovasc Res. 2000; 48(1):23–33. PMID: 11033105.
Article48. Pengo V, Lensing AW, Prins MH, Marchiori A, Davidson BL, Tiozzo F, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004; 350(22):2257–2264. PMID: 15163775.
Article49. Remy-Jardin M, Ryerson CJ, Schiebler ML, Leung AN, Wild JM, Hoeper MM, et al. Imaging of pulmonary hypertension in adults: a position paper from the Fleischner Society. Radiology. 2021; 298(3):531–549. PMID: 33399507.
Article50. Rashidi F, Parvizi R, Bilejani E, Mahmoodian B, Rahimi F, Koohi A. Evaluation of the incidence of chronic thromboembolic pulmonary hypertension 1 year after first episode of acute pulmonary embolism: a cohort study. Lung. 2020; 198(1):59–64. PMID: 31894412.
Article51. Asl Fallah S, Ghodsi S, Soleimani H, Mohebi M, Hossein Sabet A, Ariannejad H, et al. Incidence and predictors of chronic thromboembolic pulmonary hypertension following first episode of acute pulmonary embolism. Adv Respir Med. 2020; 88(6):539–547. PMID: 33393646.
Article52. Park JS, Ahn J, Choi JH, Lee HW, Oh JH, Lee HC, et al. The predictive value of echocardiography for chronic thromboembolic pulmonary hypertension after acute pulmonary embolism in Korea. Korean J Intern Med. 2017; 32(1):85–94. PMID: 27044855.
Article53. Lorenz G, Saeedan MB, Bullen J, Klok FA, Kroft LJ, Meijboom LJ, et al. CT-based biomarkers for prediction of chronic thromboembolic pulmonary hypertension after an acute pulmonary embolic event. AJR Am J Roentgenol. 2020; 215(4):800–806. PMID: 32809861.
Article54. Ende-Verhaar YM, Cannegieter SC, Vonk Noordegraaf A, Delcroix M, Pruszczyk P, Mairuhu AT, et al. Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: a contemporary view of the published literature. Eur Respir J. 2017; 49(2):1601792. PMID: 28232411.
Article55. Park SY, Lee SM, Shin JW, Choi BW, Kim H, Lee JS, et al. Epidemiology of chronic thromboembolic pulmonary hypertension in Korea: results from the Korean registry. Korean J Intern Med. 2016; 31(2):305–312. PMID: 26689916.
Article56. Brenot P, Jaïs X, Taniguchi Y, Garcia Alonso C, Gerardin B, Mussot S, et al. French experience of balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension. Eur Respir J. 2019; 53(5):1802095. PMID: 31023842.
Article57. Ogawa A, Satoh T, Fukuda T, Sugimura K, Fukumoto Y, Emoto N, et al. Balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: results of a multicenter registry. Circ Cardiovasc Qual Outcomes. 2017; 10(11):e004029. PMID: 29101270.
Article58. Kawakami T, Ogawa A, Miyaji K, Mizoguchi H, Shimokawahara H, Naito T, et al. Novel angiographic classification of each vascular lesion in chronic thromboembolic pulmonary hypertension based on selective angiogram and results of balloon pulmonary angioplasty. Circ Cardiovasc Interv. 2016; 9(10):e003318. PMID: 27729418.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Year in Review of Pulmonary Vascular Disease
- The Role of Lung Ventilation/Perfusion Scan in the Management of Chronic Thromboembolic Pulmonary Hypertension
- A Case of Chronic Thromboembolic Pulmonary Hypertension Arising from Right Atrial Thrombi Underlying Rheumatic Valvular Heart Disease and Thoracic Aorta Atherosclerotic Stenosis
- Chronic Thromboembolic Pulmonary Hypertension: Endovascular Treatment
- Pulmonary Thromboendarterectomy Under Total Circulatory Arrest
