Pasireotide treatment for severe congenital hyperinsulinism due to a homozygous ABCC8 mutation
- Mooij CF
 1
1 - Tacke CE1
- van Albada ME2
- Barthlen W3
- Bikker H4
- Mohnike K5
- Oomen MW6
- van Trotsenburg AP1
- Zwaveling-Soonawala N1
- Affiliations
-
- 1Department of Pediatric Endocrinology, Emma Children’s Hospital, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands
- 2Department of Pediatric Endocrinology, Beatrix Children’s Hospital, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands
- 3Department of Pediatric Surgery, Evangelisches Klinikum Bethel, Bielefeld, Germany
- 4Department of Clinical Genetics, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands
- 5Department of Pediatrics, Ottovon-Guericke University, Magdeburg, Germany
- 6Department of Pediatric Surgery, Emma Children’s Hospital, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands
- KMID: 2523835
- DOI: http://doi.org/10.6065/apem.2142010.005
Abstract
- ABCC8 and KCJN11 mutations cause the most severe diazoxide-resistant forms of congenital hyperinsulinism (CHI). Somatostatin analogues are considered as secondline treatment in diazoxide-unresponsive cases. Current treatment protocols include the first-generation somatostatin analogue octreotide, although pasireotide, a second-generation somatostatin analogue, might be more effective in reducing insulin secretion. Herein we report the first off-label use of pasireotide in a boy with a severe therapy-resistant form of CHI due to a homozygous ABCC8 mutation. After partial pancreatectomy, hyperinsulinism persisted; in an attempt to prevent further surgery, off-label treatment with pasireotide was initiated. Short-acting pasireotide treatment caused high blood glucose level shortly after injection. Long-acting pasireotide treatment resulted in more stable glycemic control. No side effects (e.g., central adrenal insufficiency) were noticed during a 2-month treatment period. Because of recurrent hypoglycemia despite a rather high carbohydrate intake, the boy underwent near-total pancreatectomy at the age of 11 months. In conclusion, pasireotide treatment slightly improved glycemic control without side effects in a boy with severe CHI. However, the effect of pasireotide was not sufficient to prevent near-total pancreatectomy in this case of severe CHI.
Figure
-
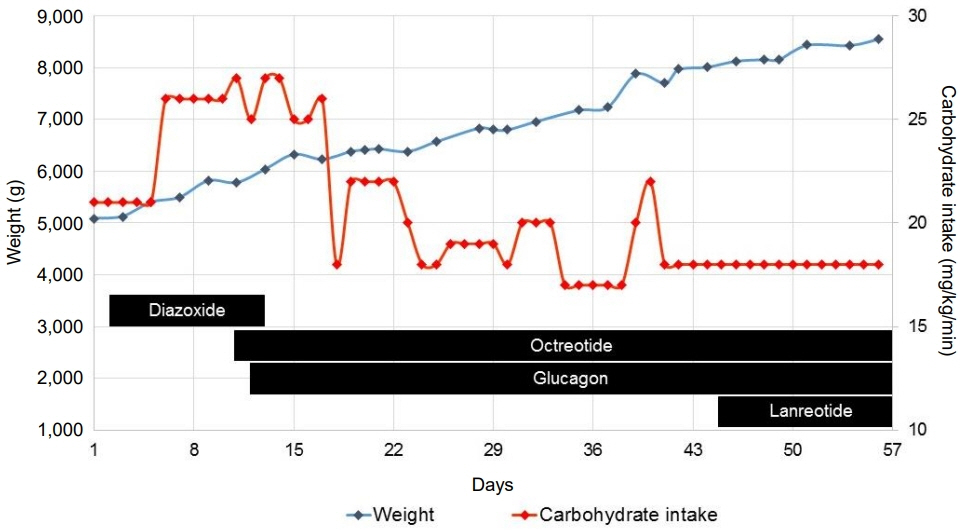
Fig. 1. Schematic overview of carbohydrate intake, patient's weight, and treatment during the first 56 days of life.
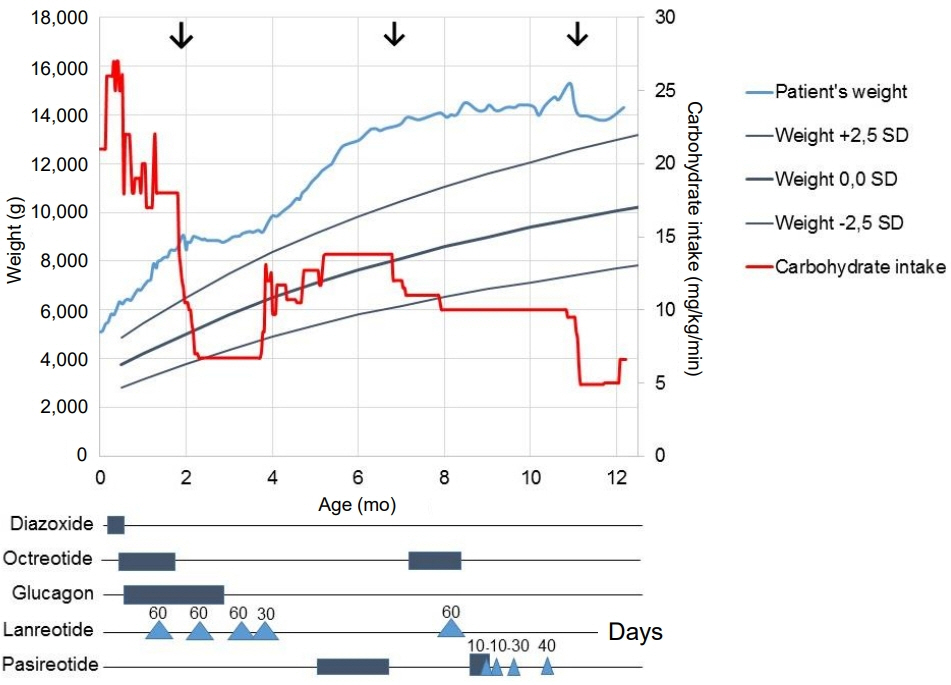
Fig. 2. Schematic overview of carbohydrate intake, patient's weight, and treatment during the first year of life. Surgical treatments are indicated by the 3 arrows. Diazoxide was given 3 times a day at the maximum dose of 20 mg/kg/day. Octreotide was given for the first 2 months of life as continuous intravenous injection with a maximum dose of 15 μg/kg/day. Octreotide was given at 7–8 months of age as continuous subcutaneous injection with a maximum dose of 40 μg/kg/day. Glucagon was initially given subcutaneously and later intravenously at a maximum dose of 20 μg/kg/hr. Lanreotide was given subcutaneously with four-week intervals; indicated by triangles with doses in mg. Short-acting pasireotide was given subcutaneously, indicated by boxes, at a maximum dose of 0.3 mg 4 times daily. Long-acting pasireotide was given as indicated by triangles with doses in mg. SD, standard deviation.
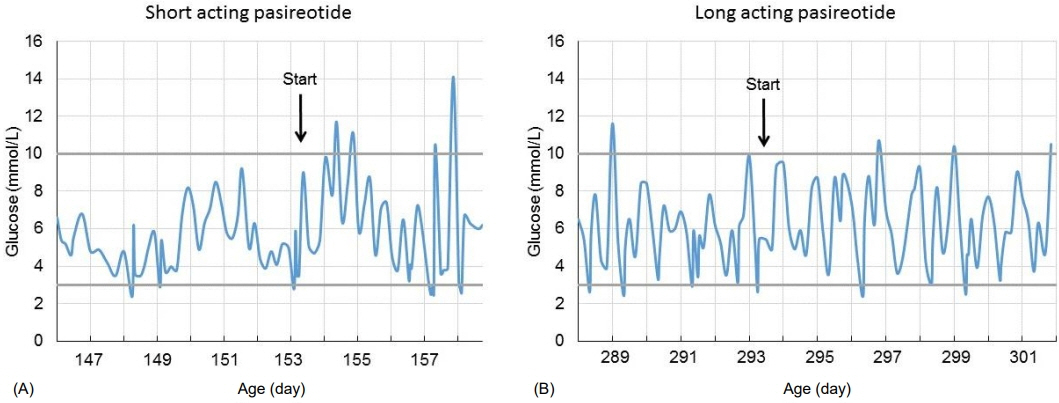
Fig. 3. Blood glucose levels (mmol/L) after initiating short-acting pasireotide (A) and after initiating long-acting pasireotide (B).
Reference
-
References
1. Gϋemes M, Rahman SA, Kapoor RR, Flanagan S, Houghton JAL, Misra S, et al. Hyperinsulinemic hypoglycemia in children and adolescents: recent advances in understanding of pathophysiology and management. Rev Endocr Metab Disord. 2020; 21:577–97.
Article2. Galcheva S, Al-Khawaga S, Hussain K. Diagnosis and management of hyperinsulinaemic hypoglycaemia. Best Pract Res Clin Endocrinol Metab. 2018; 32:551–73.
Article3. Demirbilek H, Hussain K. Congenital hyperinsulinism: diagnosis and treatment update. J Clin Res Pediatr Endocrinol. 2017; 9(Suppl 2):69–87.
Article4. De Cosio AP, Thornton P. Current and emerging agents for the treatment of hypoglycemia in patients with congenital hyperinsulinism. Paediatr Drugs. 2019; 21:123–36.
Article5. Banerjee I, Salomon-Estebanez M, Shah P, Nicholson J, Cosgrove KE, Dunne MJ. Therapies and outcomes of congenital hyperinsulinism-induced hypoglycaemia. Diabet Med. 2019; 36:9–21.
Article6. Modan-Moses D, Koren I, Mazor-Aronovitch K, Pinhas-Hamiel O, Landau H. Treatment of congenital hyperinsulinism with lanreotide acetate (Somatuline Autogel). J Clin Endocrinol Metab. 2011; 96:2312–7.
Article7. Shah P, Rahman SA, McElroy S, Gilbert C, Morgan K, Hinchey L, et al. Use of long-acting somatostatin analogue (lanreotide) in an adolescent with diazoxide-responsive congenital hyperinsulinism and its psychological impact. Horm Res Paediatr. 2015; 84:355–60.
Article8. van der Steen I, van Albada ME, Mohnike K, Christesen HT, Empting S, Salomon-Estebanez M, et al. A Multicenter experience with long-acting somatostatin analogues in patients with congenital hyperinsulinism. Horm Res Paediatr. 2018; 89:82–9.
Article9. Gomes-Porras M, Cárdenas-Salas J, Álvarez-Escolá C. Somatostatin analogs in clinical practice: a review. Int J Mol Sci. 2020; 21:1682.
Article10. de Heide LJ, Laskewitz AJ, Apers JA. Treatment of severe postRYGB hyperinsulinemic hypoglycemia with pasireotide: a comparison with octreotide on insulin, glucagon, and GLP-1. Surg Obes Relat Dis. 2014; 10:e31–3.
Article11. Schwetz V, Horvath K, Kump P, Lackner C, Perren A, Forrer F, et al. Successful medical treatment of adult nesidioblastosis with pasireotide over 3 years: a case report. Medicine (Baltimore). 2016; 95:e3272.12. Jindal R, Ahmad A, Siddiqui MA, Kochar IS, Wangnoo SK. Novel mutation c.597_598dup in exon 5 of ABCC8 gene causing congenital hyperinsulinism. Diabetes Metab Syndr. 2014; 8:45–7.
Article13. Beltrand J, Caquard M, Arnoux JB, Laborde K, Velho G, Verkarre V, et al. Glucose metabolism in 105 children and adolescents after pancreatectomy for congenital hyperinsulinism. Diabetes Care. 2012; 35:198–203.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A novel mutation of ABCC8 gene in a patient with diazoxide-unresponsive congenital hyperinsulinism
- Congenital hyperinsulinism: current status and future perspectives
- Congenital hyperinsulinism: 2 case reports with different rare variants in ABCC8
- Using low-dose octreotide with diazoxide-resistant congenital hyperinsulinism resulting from compound heterozygous mutations in the ABCC8 gene
- A Case of 2-Month-Old Infant with Persistent Hyperinsulinemic Hypoglycemia Presenting as Atonic Seizure
