Role of Genetics in Preventive Cardiology: Focused on Dyslipidemia
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2522107
- DOI: http://doi.org/10.4070/kcj.2021.0239
Abstract
- Dyslipidemia is a strong risk factor for cardiovascular disease as well as a major target for its prevention. Along with the progress in genetic research techniques and bioinformatics analysis, genetic knowledge helps manage individuals with dyslipidemia. Familial hypercholesterolemia, the most common monogenic lipid disorder, can be diagnosed clinically without confirming pathogenic mutations. However, it can be difficult to do so due to uncertain family history, and genetic testing is of vital importance in such cases. Conversely, recent studies have revealed that combination effect of rare and common variants is frequent in people with other extreme lipid phenotypes. Genetic characteristics are helpful for prediction and selection of patients with high risk for cardiovascular disease or poor response to lipid-lowering therapy. In the past decade, studies using new genetic techniques have identified novel associations among lipid metabolism-associated genes, intermediate lipid phenotypes, and cardiovascular health. Such findings shed light on new drug targets. With improvements in the platforms and processes for drug development, several recent clinical trials showed promising results regarding lipid control and potential cardiovascular disease prevention.
Figure
-
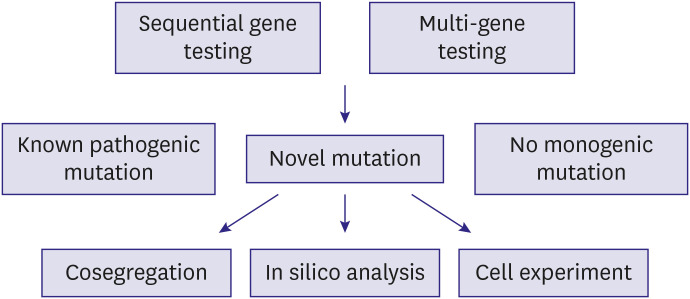
Figure 1 Flow of genetic testing for diagnosis of familial hypercholesterolemia. Any of the sequential or multi-gene testing methods can be used to identify pathogenic mutations. When novel mutations are found, their functionality can be examined through familial cosegregation, in silico analysis, or in vitro experiment assessing the function of low-density lipoprotein uptake.
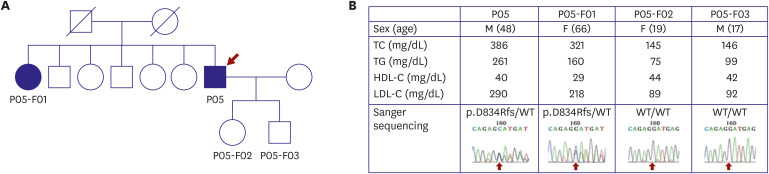
Figure 2 Example of familial cosegregation of a potential pathogenic mutation. (A) Pedigree shows people whose DNA was examined. The proband (P05), proband's sister (P05-F01), proband's daughter (P05-F02), and proband's son (P05-F03) were included. (B) The cholesterol levels of the proband and his sister were compatible with FH, whereas his 2 children had normal levels. Sanger sequencing revealed the same heterozygous mutation in the proband and his sister, whereas no mutations were present in his children (from Han et al.6)). The study including this figure was approved by the Institutional Review Board of Severance Hospital, Seoul, Korea (No. 4-2008-0267) and the participants gave written informed consent.
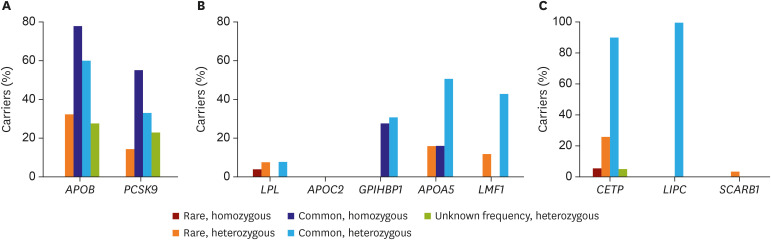
Figure 3 The prevalence of rare and common variant carriers in populations with 3 extreme lipid phenotypes. (A) Carriers of APOB or PCSK9 variants in people with very low low-density lipoprotein cholesterol level (from Lee et al.8)). (B) Carriers of LPL, APOC2, GPIHBP1, APOA5, or LMF1 variants in people with very high triglyceride levels (from Lee et al.).9) (C) Carriers of CETP, LIPC, or SCARB1 variant in people with very high high-density lipoprotein cholesterol levels (from Lee et al.).10)
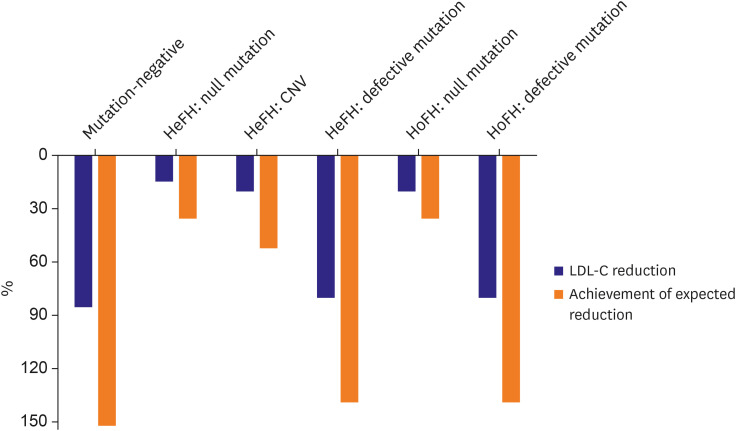
Figure 4 Achievement of expected LDL-C reduction through evolocumab treatment in patients with FH. Blue bars indicate LDL-C reduction following addition of evolocumab to the statin/ezetimibe regimen. Orange bars indicate the achievement of expected LDL-C reduction (adjusted lipid-lowering response) following addition of evolocumab to the statin/ezetimibe regimen. Differences in LDL-C reduction and adjusted response are observed according to mutation type, irrespective of disease homozygosity (From Kim et al.15)).CNV = copy number variation; FH = familial hypercholesterolemia; HeFH = heterozygous familial hypercholesterolemia; HoFH = homozygous familial hypercholesterolemia; LDL-C = low-density lipoprotein cholesterol.
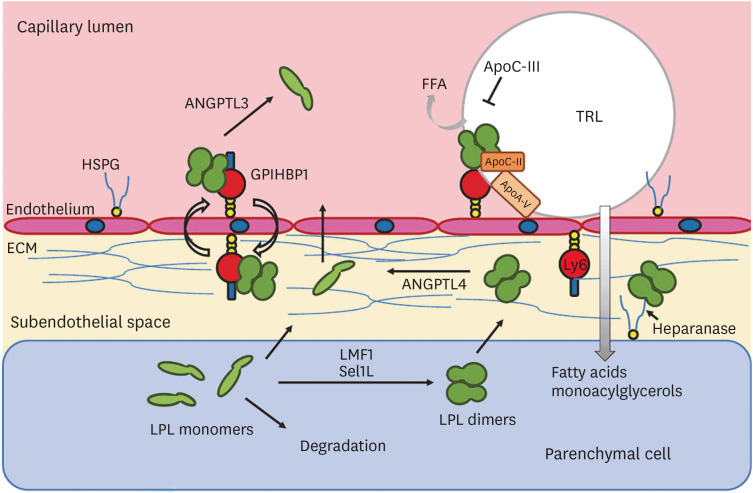
Figure 5 LPL and other related proteins supporting or inhibiting this enzyme acting in endothelial cells (from Olivecrona with permission20)). In the last decade, some of these genes and their proteins have shown considerable influence on the risk of coronary artery disease, suggesting a causal effect.ANGPTL = angiopoietin-like protein; ECM = extracellular matrix; FFA = free fatty acid; HSPG = heparan sulfate proteoglycan; GPIHBP1 = glycosylphosphatidylinositol anchored high density lipoprotein binding protein 1; LMF1 = lipase maturation factor 1; LPL = lipoprotein lipase; Sel1L = sel-1 suppressor of lin-12-like 1; TRL = triglyceride-rich lipoprotein.
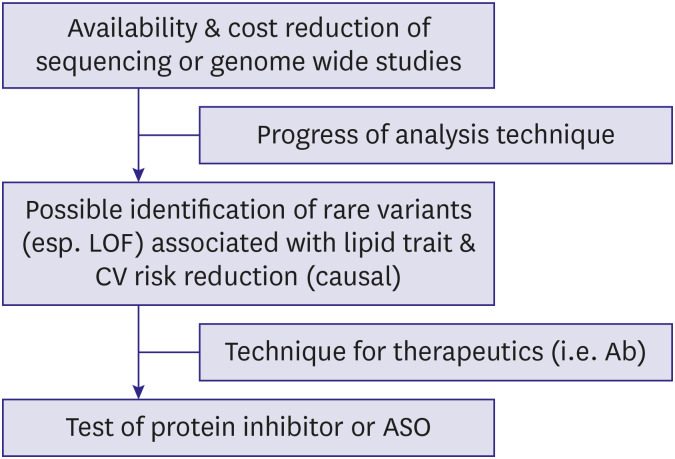
Figure 6 Flow of target discovery and drug development based on recent genetic studies. Progress and cost reduction in genetic analysis and bioinformatics helped the identification of rare functional variants that would have been previously impossible. Improvement in production of gene-targeting therapeutics improved the success rate in drug development.Ab = antibody; ASO = antisense oligonucleotide; CV = cardiovascular; LOF = loss-of-function..
Reference
-
1. Koo BK, Park S, Han KD, Moon MK. Hypertriglyceridemia is an independent risk factor for cardiovascular diseases in Korean adults aged 30–49 years: a nationwide population-based study. J Lipid Atheroscler. 2021; 10:88–98. PMID: 33537256.
Article2. Cho SM, Lee H, Lee HH, et al. Dyslipidemia fact sheets in Korea 2020: an analysis of nationwide population-based data. J Lipid Atheroscler. 2021; 10:202–209. PMID: 34095012.
Article3. McPherson R, Tybjaerg-Hansen A. Genetics of coronary artery disease. Circ Res. 2016; 118:564–578. PMID: 26892958.
Article4. Lee CJ, Lee JH, Choi S, et al. Screening, diagnosis, and treatment of familial hypercholesterolemia: symposium of the education committee, Korean Society of Lipid and Atherosclerosis. J Lipid Atheroscler. 2018; 7:122–154.
Article5. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020; 41:111–188. PMID: 31504418.6. Han SM, Hwang B, Park TG, et al. Genetic testing of Korean familial hypercholesterolemia using whole-exome sequencing. PLoS One. 2015; 10:e0126706. PMID: 25962062.
Article7. Yamashita S, Sprecher DL, Sakai N, Matsuzawa Y, Tarui S, Hui DY. Accumulation of apolipoprotein E-rich high density lipoproteins in hyperalphalipoproteinemic human subjects with plasma cholesteryl ester transfer protein deficiency. J Clin Invest. 1990; 86:688–695. PMID: 2118552.
Article8. Lee CJ, Lee Y, Park S, et al. Rare and common variants of APOB and PCSK9 in Korean patients with extremely low low-density lipoprotein-cholesterol levels. PLoS One. 2017; 12:e0186446. PMID: 29036232.
Article9. Lee CJ, Oum CY, Lee Y, et al. Variants of lipolysis-related genes in Korean patients with very high triglycerides. Yonsei Med J. 2018; 59:148–153. PMID: 29214790.
Article10. Lee CJ, Park MS, Kim M, et al. CETP, LIPC, and SCARB1 variants in individuals with extremely high high-density lipoprotein-cholesterol levels. Sci Rep. 2019; 9:10915. PMID: 31358896.
Article11. Tada H, Kawashiri MA, Nohara A, Inazu A, Mabuchi H, Yamagishi M. Impact of clinical signs and genetic diagnosis of familial hypercholesterolaemia on the prevalence of coronary artery disease in patients with severe hypercholesterolaemia. Eur Heart J. 2017; 38:1573–1579. PMID: 28159968.12. Santos PC, Morgan AC, Jannes CE, et al. Presence and type of low density lipoprotein receptor (LDLR) mutation influences the lipid profile and response to lipid-lowering therapy in Brazilian patients with heterozygous familial hypercholesterolemia. Atherosclerosis. 2014; 233:206–210. PMID: 24529145.
Article13. Santos PC, Pereira AC. Type of LDLR mutation and the pharmacogenetics of familial hypercholesterolemia treatment. Pharmacogenomics. 2015; 16:1743–1750. PMID: 26427613.
Article14. Perez de Isla L, Alonso R, Watts GF, et al. Attainment of LDL-cholesterol treatment goals in patients with familial hypercholesterolemia: 5-year SAFEHEART registry follow-up. J Am Coll Cardiol. 2016; 67:1278–1285. PMID: 26988947.15. Kim H, Lee CJ, Pak H, et al. GENetic characteristics and REsponse to lipid-lowering therapy in familial hypercholesterolemia: GENRE-FH study. Sci Rep. 2020; 10:19336. PMID: 33168860.
Article16. Postmus I, Trompet S, Deshmukh HA, et al. Pharmacogenetic meta-analysis of genome-wide association studies of LDL cholesterol response to statins. Nat Commun. 2014; 5:5068. PMID: 25350695.17. Natarajan P, Young R, Stitziel NO, et al. Polygenic risk score identifies subgroup with higher burden of atherosclerosis and greater relative benefit from statin therapy in the primary prevention setting. Circulation. 2017; 135:2091–2101. PMID: 28223407.
Article18. Teslovich TM, Musunuru K, Smith AV, et al. Biological, clinical and population relevance of 95 loci for blood lipids. Nature. 2010; 466:707–713. PMID: 20686565.19. Crosby J, Peloso GM, Auer PL, et al. Loss-of-function mutations in APOC3, triglycerides, and coronary disease. N Engl J Med. 2014; 371:22–31. PMID: 24941081.
Article20. Spiller W, Jung KJ, Lee JY, Jee SH. Precision medicine and cardiovascular health: insights from Mendelian randomization analyses. Korean Circ J. 2020; 50:91–111. PMID: 31845553.
Article21. Lee SH, Lee JY, Kim GH, et al. Two-sample Mendelian randomization study of lipid levels and ischemic heart disease. Korean Circ J. 2020; 50:940–948. PMID: 32812402.
Article22. Olivecrona G. Role of lipoprotein lipase in lipid metabolism. Curr Opin Lipidol. 2016; 27:233–241. PMID: 27031275.
Article23. Musunuru K, Pirruccello JP, Do R, et al. Exome sequencing, ANGPTL3 mutations, and familial combined hypolipidemia. N Engl J Med. 2010; 363:2220–2227. PMID: 20942659.24. Dewey FE, Gusarova V, O'Dushlaine C, et al. Inactivating variants in ANGPTL4 and risk of coronary artery disease. N Engl J Med. 2016; 374:1123–1133. PMID: 26933753.
Article25. Levin AA. Treating disease at the RNA level with oligonucleotides. N Engl J Med. 2019; 380:57–70. PMID: 30601736.
Article26. Raal FJ, Rosenson RS, Reeskamp LF, et al. Evinacumab for homozygous familial hyperchoelsterolemia. N Engl J Med. 2020; 383:711–720. PMID: 32813947.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New European Society of Cardiology/European Atherosclerosis Society Guideline for the Management of Dyslipidemia
- Epidemiology of dyslipidemia in Korea
- Prevalence of Dyslipidemia among Korean Adults: Korea National Health and Nutrition Survey 1998-2005
- Recent Guideline for the Management of Dyslipidemia in Patients with Diabetes
- Recent dyslipidemia guidelines for patients with diabetes mellitus
