Infiltrative hepatocellular carcinoma with multiple lung metastasis completely cured using nivolumab: a case report
- Affiliations
-
- 1Department of Gastroenterology, Ajou University School of Medicine, Suwon, Korea
- KMID: 2520904
- DOI: http://doi.org/10.17998/jlc.2021.08.26
Abstract
- The current Food and Drug Administration-approved systemic treatments for advanced hepatocellular carcinoma (HCC) include multikinase inhibitors (tyrosine kinase inhibitor [TKI]) and immune checkpoint inhibitors (ICIs). Among ICIs, nivolumab is used as secondline therapy for advanced HCC after sorafenib failure or patient intolerance. In this case, a patient with infiltrative HCC and portal vein tumor thrombosis was treated with hepatic arterial infusion chemotherapy (HAIC) and radiation therapy. New lung metastasis developed after HAICs; thus, lenvatinib treatment was initiated. However, the disease progressed. Thereafter, sorafenib treatment was initiated but he developed intolerance, with grade 3 sorafenib-related diarrhea. Subsequently, nivolumab was administered as rescue therapy. He demonstrated a partial response to nivolumab after the third treatment and viable HCCs in the lungs and liver completely disappeared after the 24th treatment. These findings suggest that nivolumab could be used as an effective rescue therapy for advanced HCC progression after TKI treatment.
Figure
-

Figure 1 Hepatocellular carcinoma at initial diagnosis in order of abdomen, chest computed tomography (CT) and liver magnetic resonance imaging (MRI). Abdominal CT showing a single mass (arrows) on segment 6 with enhancement in the arterial phase (A) and wash-out on the delayed phase (B). Chest CT (C) showing no lung metastasis on initial diagnosis. Liver MRI showing a single mass (arrow) with an expansile tumor thrombus partially extending from the right portal vein to the main portal vein in the delayed arterial phase (D) of T1-weighted images. Transitional phase (E). T2-weighted image (F). Hepatobiliary phase (G). Diffusion-weighted image (b=800) (H).

Figure 2 A change in the portal vein tumor thrombus, newly developed hepatocellular carcinoma (HCC), and lung metastasis in liver dynamic computed tomography after HAIC with radiation therapy (RT). (A, B) Shrinkage of viable tumor and portal vein tumor thrombus (red arrow) after hepatic artery infusion chemotherapy (HAIC) with RT. (C, D) Multiple lung metastases (yellow arrow) after HAIC with RT. (E) New primary HCC (yellow arrow) in segment 8 after HAIC with RT.

Figure 3 Progression of hepatocellular carcinoma (HCC), portal vein tumor thrombus (PVTT), and lung metastases in liver dynamic computed tomography (CT) after lenvatinib therapy. Follow-up liver dynamic CT showing increase in the arterial enhancing portion of the existing primary HCC (red arrow) and PVTT (B) compared to before lenvatinib therapy (A). Additionally, new HCCs (yellow arrows) are visible in several hepatic segments (C–E) and multiple lung metastases show progression (yellow arrows) (F, G).

Figure 4 Changes in α-fetoprotein (AFP) and protein induced by vitamin K absence-II (PIVKA-II) levels as well as liver function during nivolumab therapy. Serum AFP and PIVKA-II levels decreased continuously from the first administration of nivolumab. (A–D) Preserved liver function during nivolumab therapy.
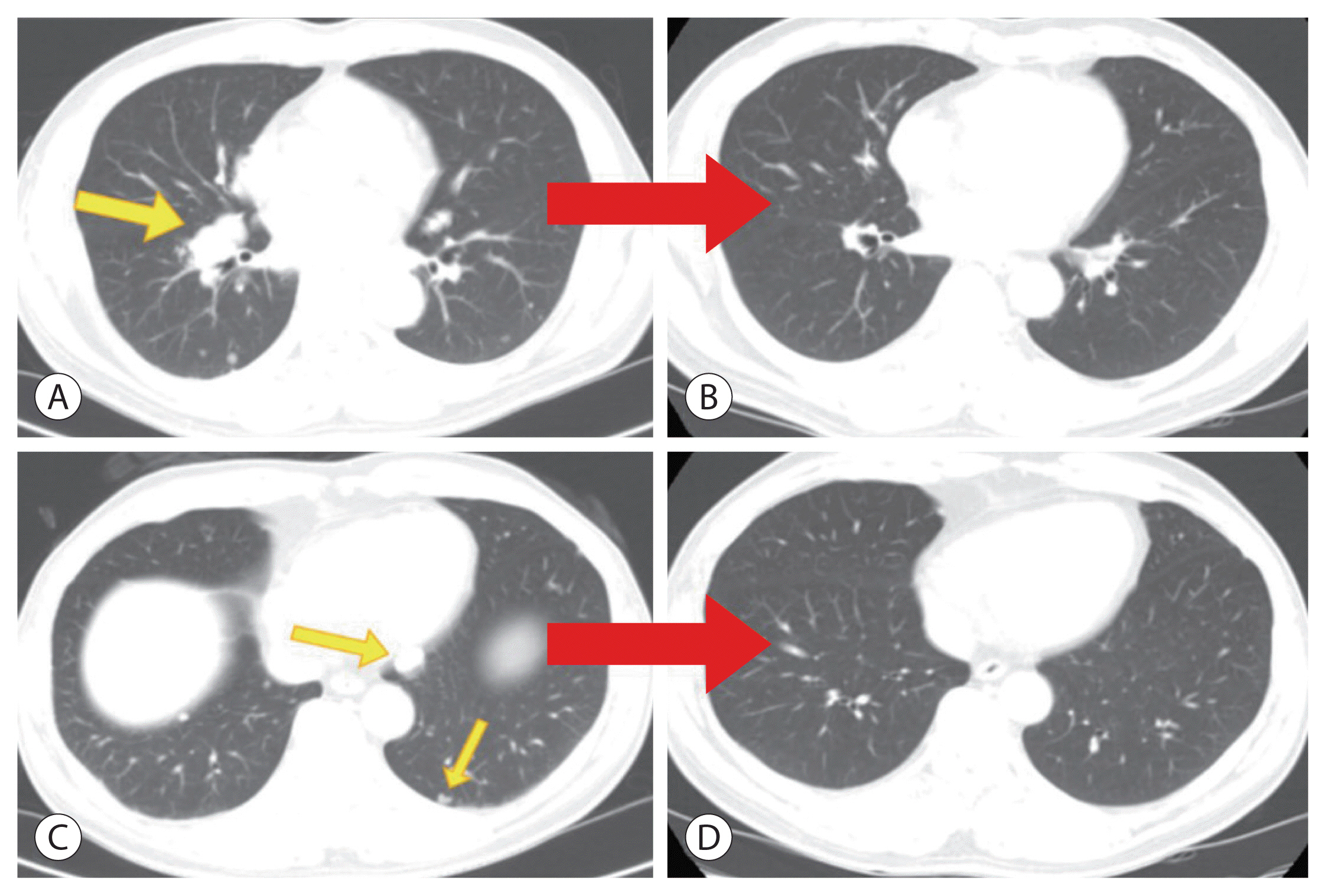
Figure 5 Complete disappearance of multiple lung metastases (arrows) on chest computed tomography after the 18th nivolumab treatment. Multiple pulmonary nodules disappeared after the 18th administration of nivolumab (B, D) compared to before nivolumab therapy (A, C).

Figure 6 Liver magnetic resonance imaging after the 24th nivolumab treatment, showing no evidence of viable tumors exhibiting arterial enhancement in the liver and contracted expansile portal vein tumor thrombus. (A) T1-weighted image, hepatic arterial phase. (B) Portal venous phase. (C) Delayed phase. (D) T2-weighted image. (E) Hepatobiliary phase. (F) Diffusion-weighted image (b=800).
Reference
-
References
1. Global Burden of Disease Liver Cancer Collaboration. Akinyemiju T, Abera S, Ahmed M, Alam N, Alemayohu MA, et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: results from the global burden of disease study 2015. JAMA Oncol. 2017; 3:1683–1691.2. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017; 153:996–1005.e1001.3. Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021; 7:6.4. Yim SY, Lee JS. The genomic landscape and its clinical implications in hepatocellular carcinoma. J Liver Cancer. 2019; 19:97–107.5. Choi JH, Chung WJ, Bae SH, Song DS, Song MJ, Kim YS, et al. Randomized, prospective, comparative study on the effects and safety of sorafenib vs. hepatic arterial infusion chemotherapy in patients with advanced hepatocellular carcinoma with portal vein tumor thrombosis. Cancer Chemother Pharmacol. 2018; 82:469–478.6. Song DS, Song MJ, Bae SH, Chung WJ, Jang JY, Kim YS, et al. A comparative study between sorafenib and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis. J Gastroenterol. 2015; 50:445–454.7. Guo Y, Li J, Dong P, Feng X, Xu J, Ye Y, et al. Epidemiological serosurvey of hepatitis B in national disease surveillance points of Henan province in 2014. Zhonghua Yu Fang Yi Xue Za Zhi. 2016; 50:279–281.8. Chan SL, Chong CC, Chan AW, Poon DM, Chok KS. Management of hepatocellular carcinoma with portal vein tumor thrombosis: Review and update at 2016. World J Gastroenterol. 2016; 22:7289–7300.9. Katyal S, Oliver JH 3rd, Peterson MS, Ferris JV, Carr BS, Baron RL. Extrahepatic metastases of hepatocellular carcinoma. Radiology. 2000; 216:698–703.10. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999; 19:329–338.11. Mohr R, Jost-Brinkmann F, Özdirik B, Lambrecht J, Hammerich L, Loosen SH, et al. Lessons from immune checkpoint inhibitor trials in hepatocellular carcinoma. Front Immunol. 2021; 12:652172.12. Ringelhan M, Pfister D, O’Connor T, Pikarsky E, Heikenwalder M. The immunology of hepatocellular carcinoma. Nat Immunol. 2018; 19:222–232.13. Finn RS, Ryoo BY, Merle P, Kudo M, Bouattour M, Lim HY, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. 2020; 38:193–202.14. Qin S, Ren Z, Meng Z, Chen Z, Chai X, Xiong J, et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, phase 2 trial. Lancet Oncol. 2020; 21:571–580.15. Cheng H, Sun G, Chen H, Li Y, Han Z, Li Y, et al. Trends in the treatment of advanced hepatocellular carcinoma: immune checkpoint blockade immunotherapy and related combination therapies. Am J Cancer Res. 2019; 9:1536–1545.16. Yau T, Park JW, Finn RS, Cheng AL, Mathurin P, Edeline J, et al. LBA38_PR - CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2019; 30:v874–v875.17. Kim J, Chang JW, Park JY. Nivolumab for advanced hepatocellular carcinoma with multiple lung metastases after sorafenib failure. J Liver Cancer. 2020; 20:72–77.18. Zhu SG, Li HB, Yuan ZN, Liu W, Yang Q, Cheng Y, et al. Achievement of complete response to nivolumab in a patient with advanced sarcomatoid hepatocellular carcinoma: a case report. World J Gastrointest Oncol. 2020; 12:1209–1215.19. Trojan J, Sarrazin C. Complete response of hepatocellular carcinoma in a patient with end-stage liver disease treated with nivolumab: whishful thinking or possible? Am J Gastroenterol. 2016; 111:1208–1209.20. Liu YT, Sun ZJ. Turning cold tumors into hot tumors by improving T-cell infiltration. Theranostics. 2021; 11:5365–5386.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nivolumab for Advanced Hepatocellular Carcinoma with Multiple Lung Metastases after Sorafenib Failure
- A case of nearly complete response in hepatocellular carcinoma with disseminated lung metastasis by combination therapy of nivolumab and ipilimumab after treatment failure of atezolizumab plus bevacizumab
- Uptake of 99mTc - DISDA in Primary Hepatocellular Carcinoma and Metastatic Nodule in the Lung
- A Case of Cutaneous Metastasis from Hepatocellular Carcinoma Manifested as Multiple Nodules on Whole Body
- Unusual Semimembranosus Muscle Metastasis from Hepatocellular Carcinoma
