Funneling venoplasty for anomalous graft left hepatic vein in living donor liver transplantation using a split left lateral section graft for an infant patient
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2519300
- DOI: http://doi.org/10.14701/ahbps.2021.25.3.408
Abstract
- The left lateral section (LLS) can have an unusual variant left hepatic vein (LHV) anatomy. We present a case of customized funneling venoplasty of the graft LHV in a 22-month-old girl diagnosed with ornithine transcarbamylase deficiency undergoing deceased donor liver transplantation (LT) using a split LLS graft. The split LLS graft weighed 350 g, yielding a graft-to-recipient weight ratio of 3.2%.Notably, the graft LHV opening was located at the graft liver cut surface, which was only 1 cm in size and 2 cm away from the cephalad apex of the LLS graft. Since such a variant location of the small LHV opening was unsuitable for direct anastomosis, we performed a funneling venoplasty using an inferior vena cava fragment homograft obtained from the same donor. The graft implantation was performed according to standard procedures of infant split LT. Follow-up imaging studies showed no vascular complications. The patient recovered uneventfully from the LT operation. She had normal blood test findings, including normal ammonia level. She has been doing well for 6 months after the transplantation. In conclusion, our surgical technique using a funneling venoplasty enabled successful reconstruction of the anomalous graft LHV. Our results suggest that individualized reconstruction techniques should be applied to infant patients undergoing LT using a LLS graft with variant types of graft LHV anatomy.
Keyword
Figure
-
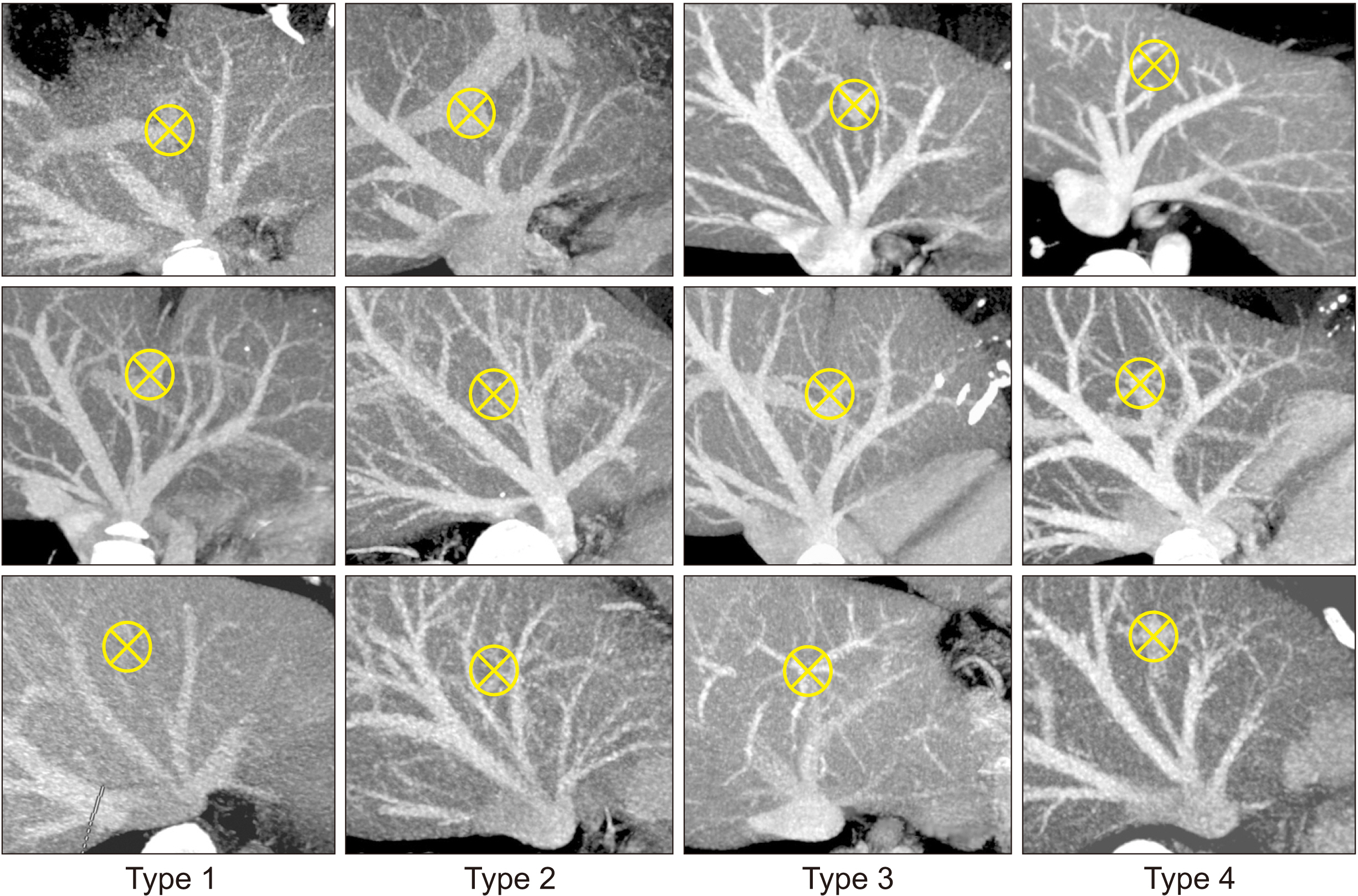
Fig. 1 Classification of the hepatic vein anatomy in the left lateral section in terms of patterns of the left lateral section graft hepatic vein openings. Type 1 makes a single opening. Type 2 makes two widely spaced openings. Type 3 makes large and small adjacent openings. Type 4 makes two widely spaced openings. Crossed circles indicate the location of the umbilical portion. Cited from the article of Hwang et al. (Liver Transpl 2013;19:184-190) [1].
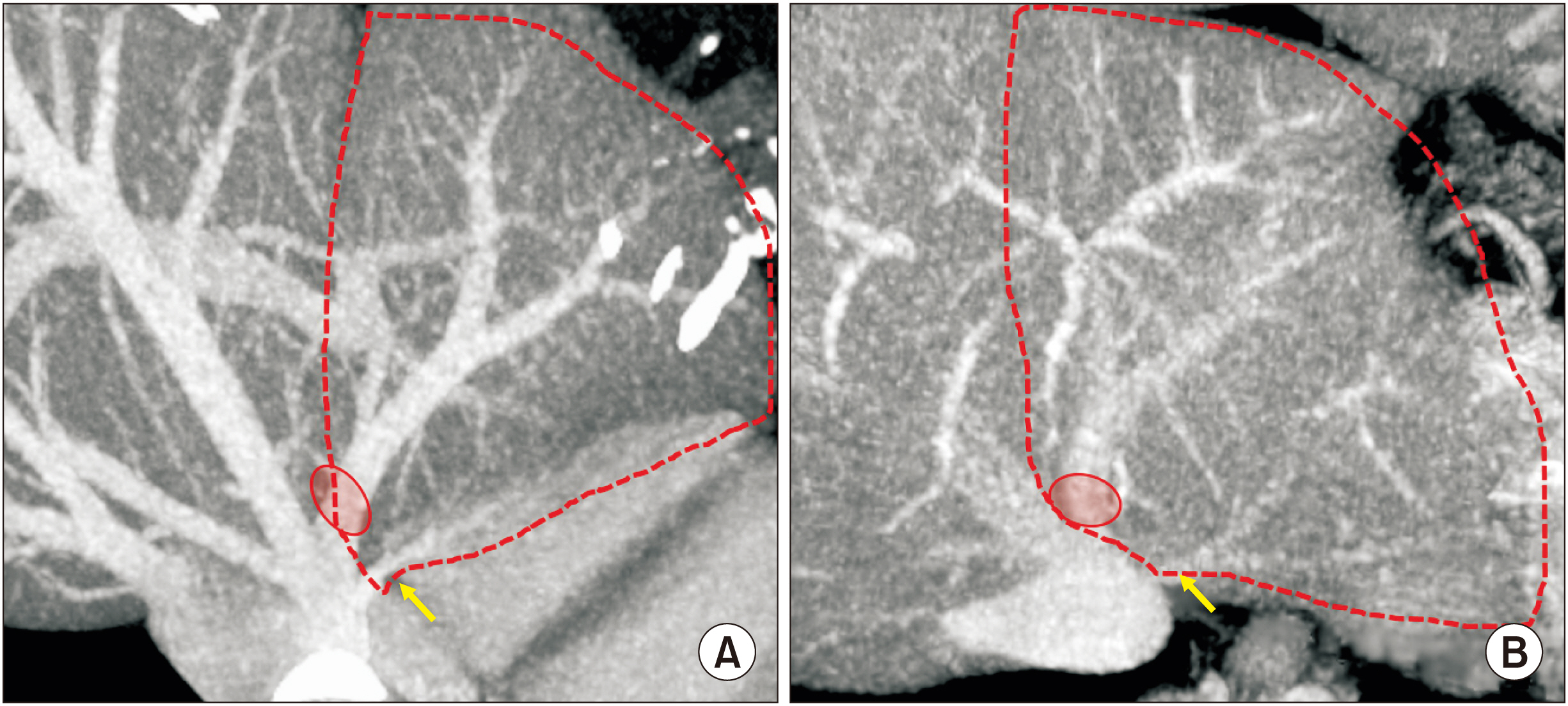
Fig. 2 Presumed anatomy of the donor liver. The anatomy of the left hepatic vein appears to be a mixed type of two images with narrow (A) and wide (B) distances between the large and small hepatic vein openings. The small opening indicates the superficial branch of the left hepatic vein (arrows).
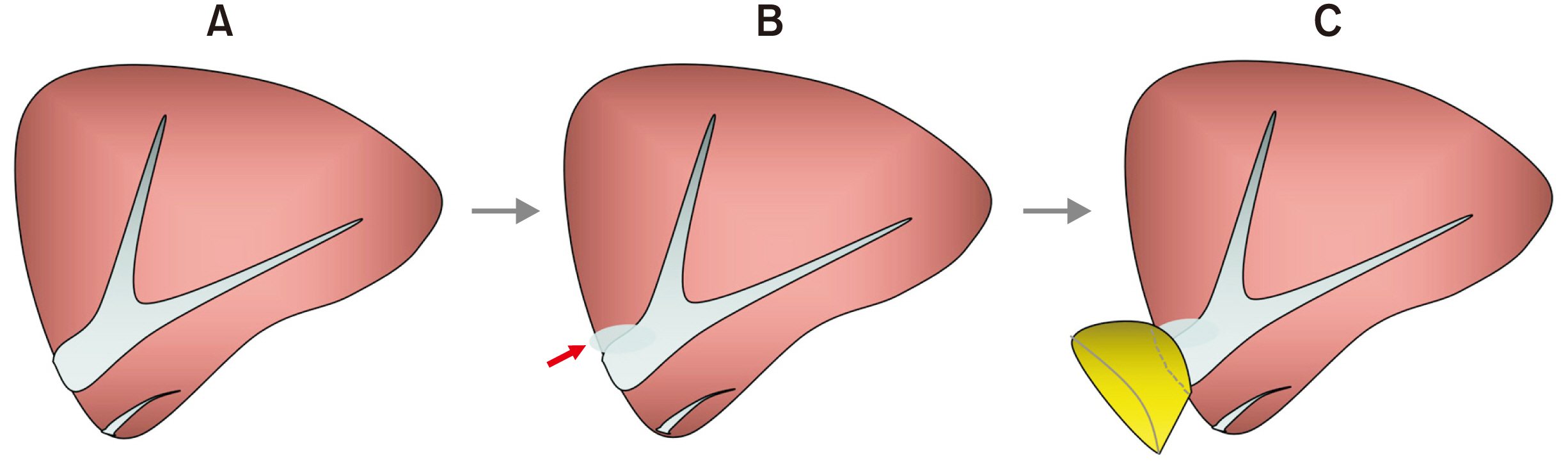
Fig. 3 Design of customized funneling venoplasty for the graft left hepatic vein opening. The 1 cm-sized orifice (A) is partially incised to increase the diameter (B). A vein patch is attached at the enlarged graft hepatic vein opening to make a funnel-shaped conduit (C). Arrow indicates a slit incision.
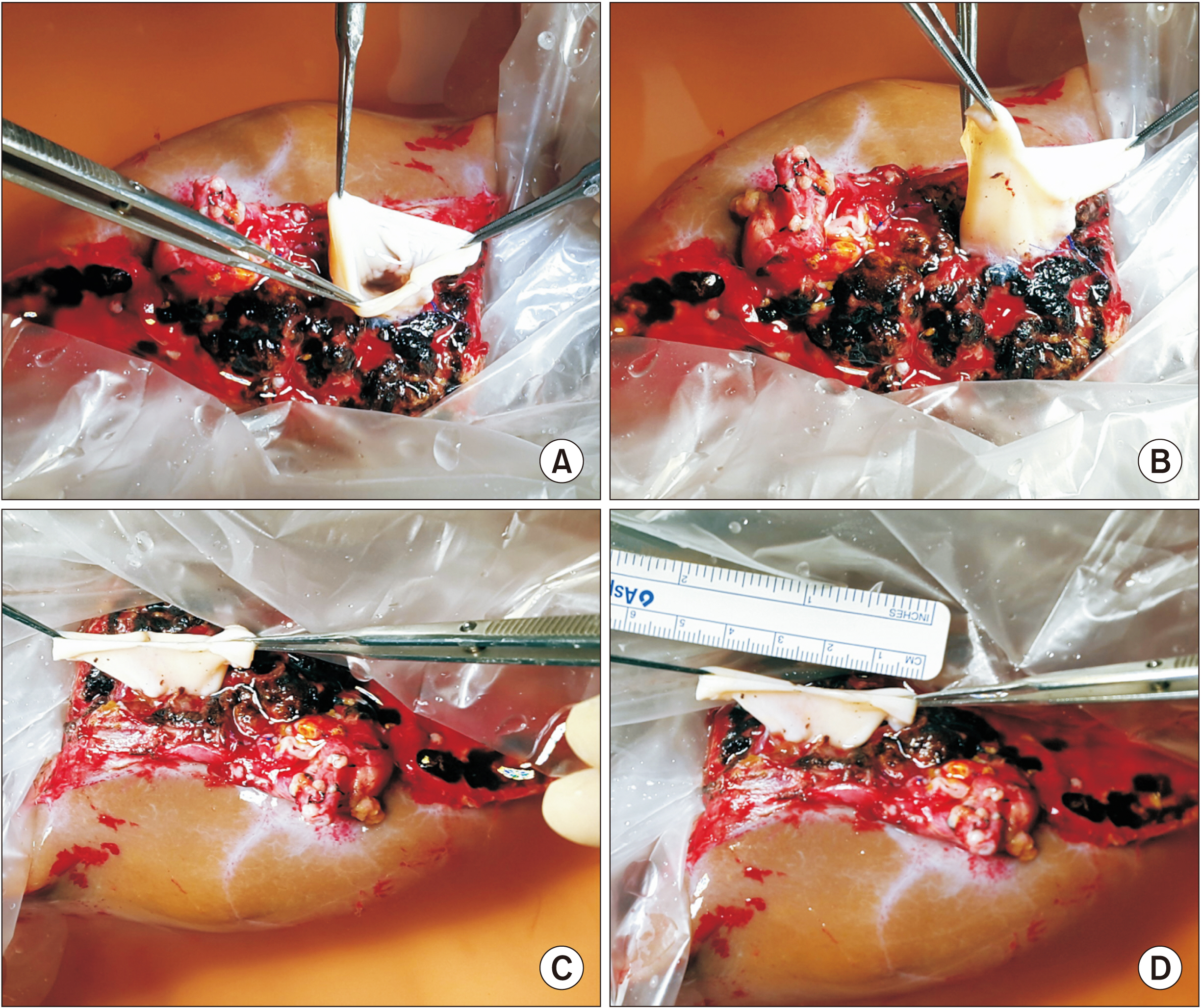
Fig. 4 Intraoperative photographs of bench work. (A–C) An inferior vena cava fragment homograft is attached to the graft hepatic vein orifice to make a funnel-shaped conduit. (D) The cephalad end of the conduit is much larger than the graft side.
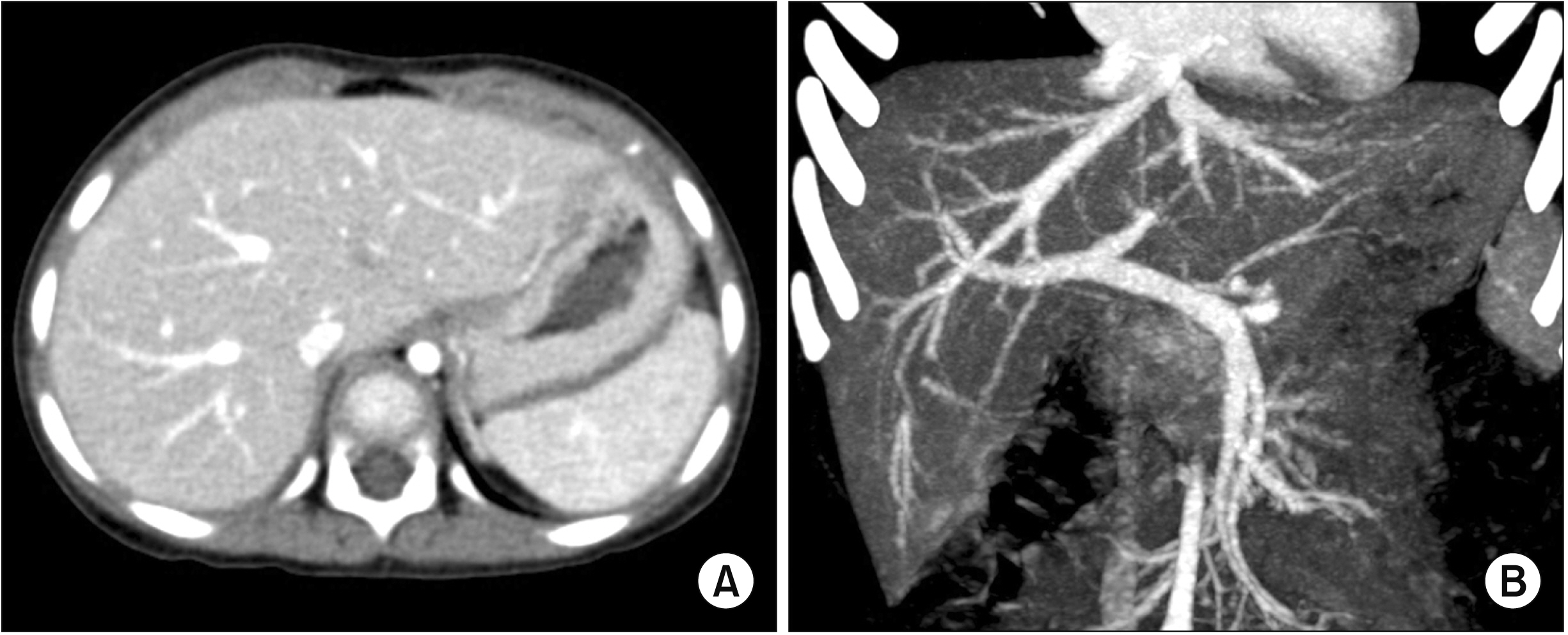
Fig. 5 Preoperative computed tomography images showing no gross abnormality in liver shape (A) or hepatic vasculature (B).

Fig. 6 Intraoperative photographs of recipient hepatic vein reconstruction. (A) The three hepatic vein openings are widely opened to make an enlarged orifice. (B) The hepatic vein openings at the recipient inferior vena cava and the graft are well matched in size. (C) The posterior wall of the hepatic vein reconstruction is visible. (D) The anterior wall of the hepatic vein reconstruction is visible.
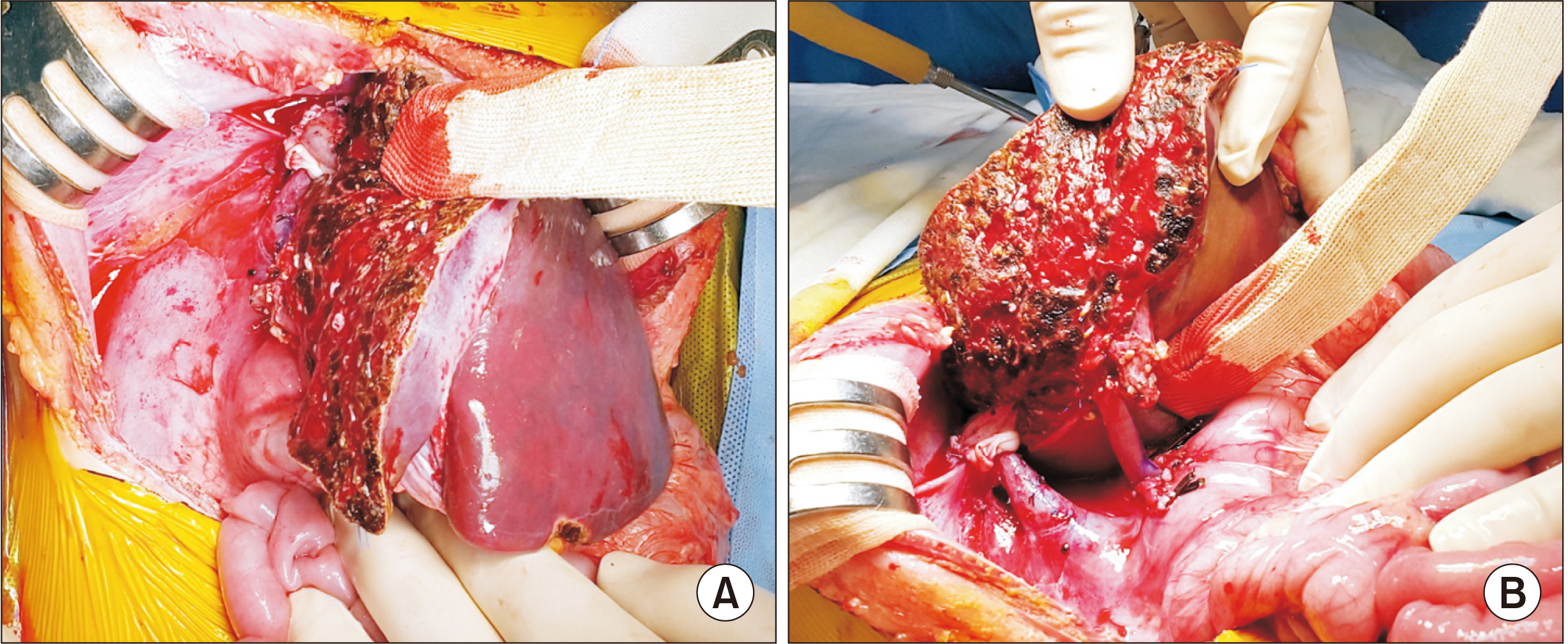
Fig. 7 Intraoperative photographs of left lateral section graft implantation. (A) The hepatic vein reconstruction is located at the orthodox position. (B) Portal vein reconstruction is performed using a branch patch of the recipient portal vein.
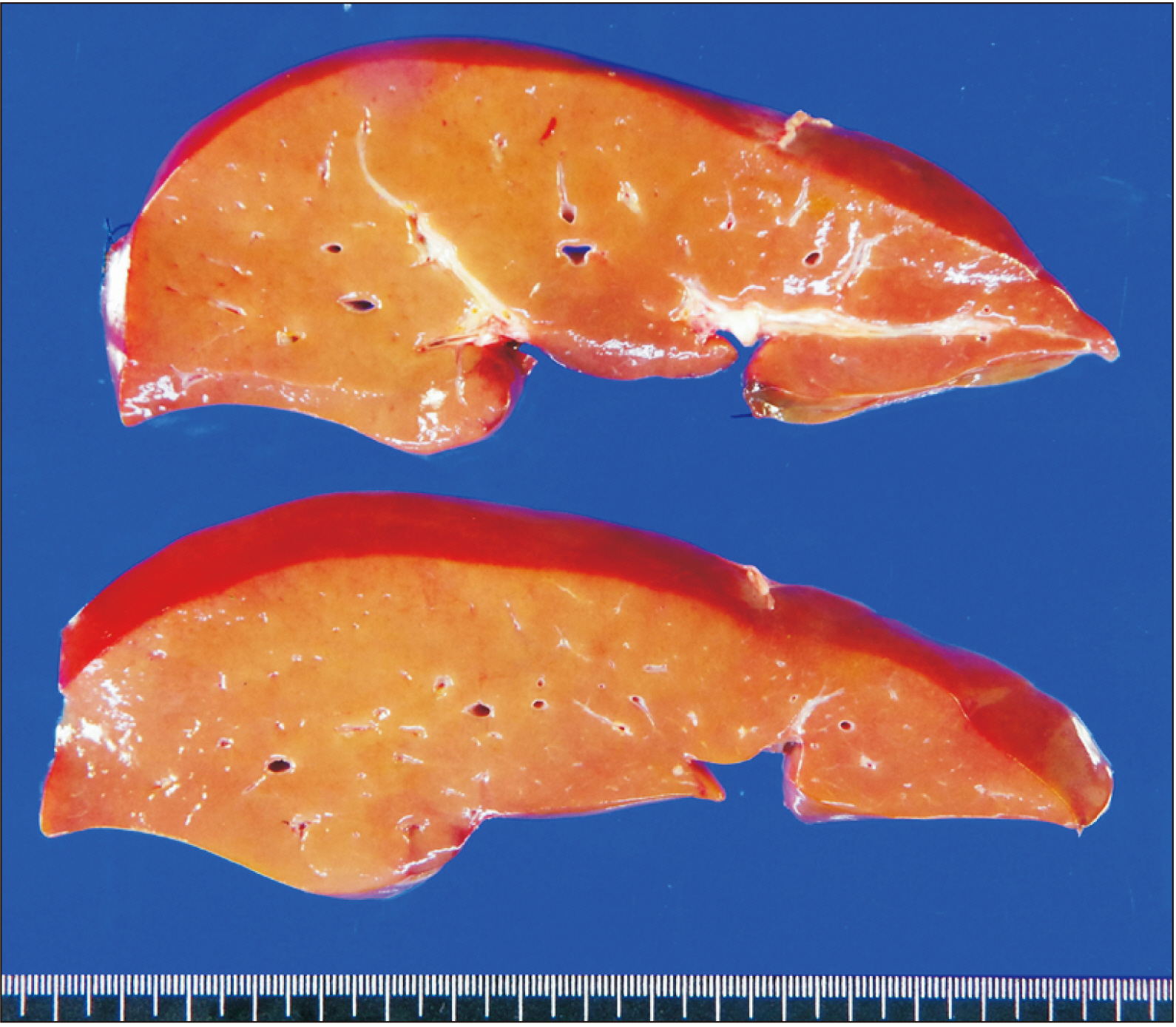
Fig. 8 Gross photograph of the explant liver.
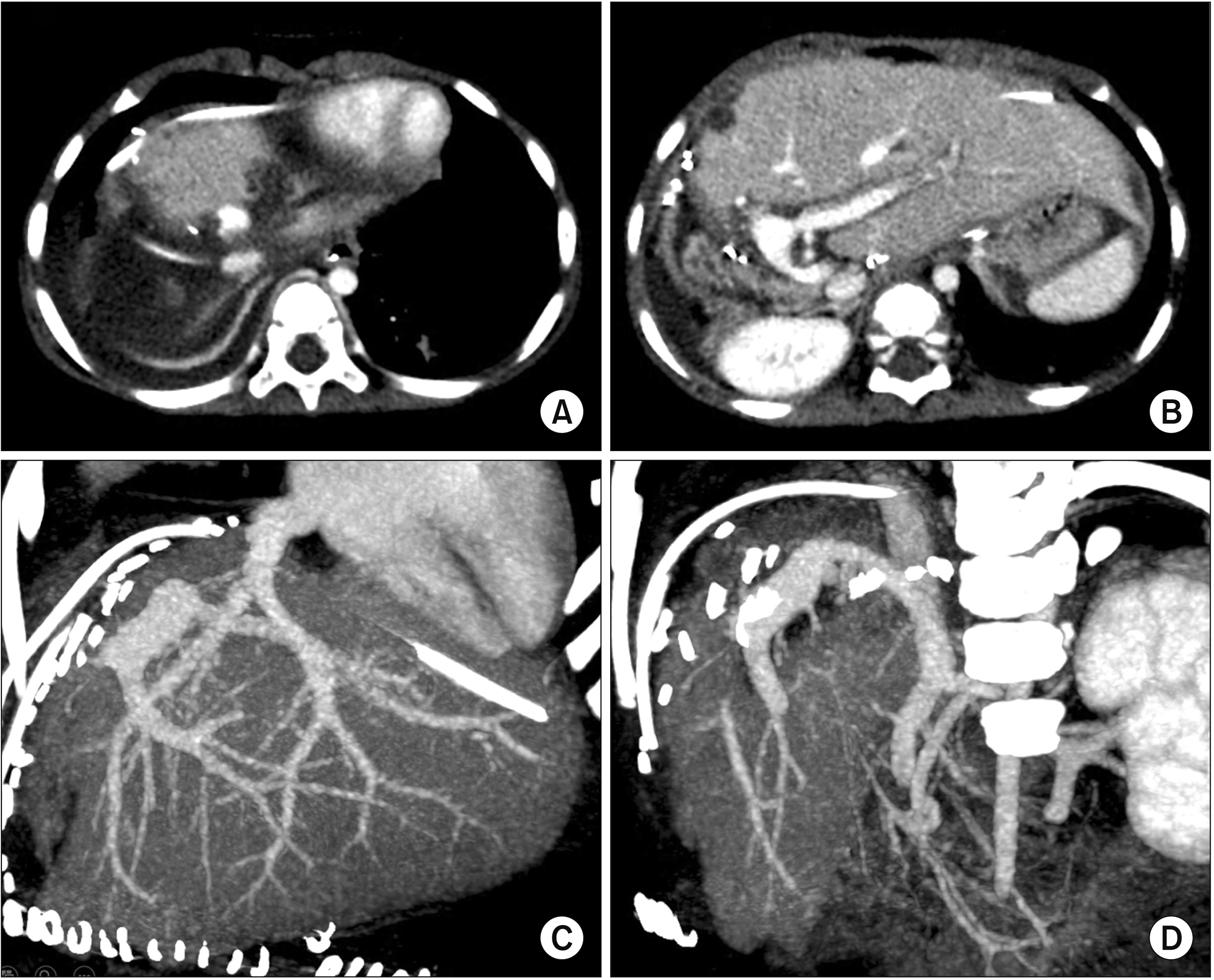
Fig. 9 Follow-up computed tomography images taken 4 days after liver transplantation. The hepatic vein reconstruction (A, C) appears smooth and streamlined without stenosis. The portal vein reconstruction (B, D) shows a size discrepancy without noticeable stenosis.
Cited by 1 articles
-
Modified left liver graft with funneling venoplasty of middle hepatic vein branches for pediatric living donor liver transplantation
Jung-Man Namgoong, Gil-Chun Park, Shin Hwang, Sang-Hoon Kim, Suhyeon Ha, Kyung Mo Kim, Seak Hee Oh
Ann Liver Transplant. 2023;3(1):44-49. doi: 10.52604/alt.23.0002.
Reference
-
1. Hwang S, Kim KH, Kim DY, Kim KM, Ahn CS, Moon DB, et al. 2013; Anomalous hepatic vein anatomy of left lateral section grafts and customized unification venoplasty for pediatric living donor liver transplantation. Liver Transpl. 19:184–190. DOI: 10.1002/lt.23557. PMID: 23045153.
Article2. Hwang S, Lee SG, Choi ST, Moon DB, Ha TY, Lee YJ, et al. 2005; Hepatic vein anatomy of the medial segment for living donor liver transplantation using extended right lobe graft. Liver Transpl. 11:449–455. DOI: 10.1002/lt.20387. PMID: 15776411.
Article3. Radtke A, Sotiropoulos GC, Sgourakis G, Molmenti EP, Schroeder T, Saner FH, et al. 2010; Hepatic venous drainage: how much can we learn from imaging studies? Anatomic-functional classification derived from three-dimensional computed tomography reconstructions. Transplantation. 89:1518–1525. DOI: 10.1097/TP.0b013e3181dd6bac. PMID: 20410853.
Article4. Mochizuki K, Takatsuki M, Soyama A, Hidaka M, Obatake M, Eguchi S. 2012; The usefulness of a high-speed 3D-image analysis system in pediatric living donor liver transplantation. Ann Transplant. 17:31–34. DOI: 10.12659/AOT.882633. PMID: 22466906.
Article5. Hwang S, Lee SG, Lee YJ, Park KM, Ahn CS, Kim KH. 2006; Postoperative changes in remnant medial segment parenchyma of living donor livers after procurement of left lateral segment graft. Hepatogastroenterology. 53:773–777. PMID: 17086886.6. Seda-Neto J, Godoy AL, Carone E, Pugliese V, Fonseca EA, Porta G, et al. 2008; Left lateral segmentectomy for pediatric live-donor liver transplantation: special attention to segment IV complications. Transplantation. 86:697–701. DOI: 10.1097/TP.0b013e318183ed22. PMID: 18791451.
Article7. Namgoong JM, Hwang S, Park GC, Ahn CS, Kim KH, Kim KM, et al. 2021; Outflow vein venoplasty of left lateral section graft for living donor liver transplantation in infant recipients. Pediatr Transplant. 25:e13970. DOI: 10.1111/petr.13970. PMID: 33433048.
Article8. Galloux A, Pace E, Franchi-Abella S, Branchereau S, Gonzales E, Pariente D. 2018; Diagnosis, treatment and outcome of hepatic venous outflow obstruction in paediatric liver transplantation: 24-year experience at a single centre. Pediatr Radiol. 48:667–679. DOI: 10.1007/s00247-018-4079-y. PMID: 29468367.
Article9. Katano T, Sanada Y, Hirata Y, Yamada N, Okada N, Onishi Y, et al. 2019; Endovascular stent placement for venous complications following pediatric liver transplantation: outcomes and indications. Pediatr Surg Int. 35:1185–1195. DOI: 10.1007/s00383-019-04551-9. PMID: 31535198.
Article10. Zhang ZY, Jin L, Chen G, Su TH, Zhu ZJ, Sun LY, et al. 2017; Balloon dilatation for treatment of hepatic venous outflow obstruction following pediatric liver transplantation. World J Gastroenterol. 23:8227–8234. DOI: 10.3748/wjg.v23.i46.8227. PMID: 29290659. PMCID: PMC5739929.
Article11. Lu KT, Cheng YF, Chen TY, Tsang LC, Ou HY, Yu CY, et al. 2018; Efficiency of transluminal angioplasty of hepatic venous outflow obstruction in pediatric liver transplantation. Transplant Proc. 50:2715–2717. DOI: 10.1016/j.transproceed.2018.04.022. PMID: 30401383.
Article12. Yeh YT, Chen CY, Tseng HS, Wang HK, Tsai HL, Lin NC, et al. 2017; Enlarging vascular stents after pediatric liver transplantation. J Pediatr Surg. 52:1934–1939. DOI: 10.1016/j.jpedsurg.2017.08.060. PMID: 28927979.
Article13. Namgoong JM, Hwang S, Yoon YI, Cho YP, Kang WH, Kwon YJ, et al. 2021; Third retransplantation using a whole liver graft for late graft failure from hepatic vein stent stenosis in a pediatric patient who underwent split liver retransplantation. Ann Hepatobiliary Pancreat Surg. 25:299–306. DOI: 10.14701/ahbps.2021.25.2.299. PMID: 34053936. PMCID: PMC8180402.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tailored techniques of graft outflow vein reconstruction in pediatric liver transplantation at Asan Medical Center
- Modified left liver graft with funneling venoplasty of middle hepatic vein branches for pediatric living donor liver transplantation
- Graft outflow vein unification venoplasty with superficial left hepatic vein branch in pediatric living donor liver transplantation using a left lateral section graft
- Graft outflow vein venoplasty for a laparoscopically harvested left lateral section graft in pediatric living donor liver transplantation
- Outflow vein venoplasty of left lateral section graft for living donor liver transplantation in infant recipients
