Fatal Myopericarditis in a Patient With Lupus Erythematosus Supported by Extracorporeal Membrane Oxygenation: A Case Report
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine and Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea
- 2Division of Rheumatology, Department of Internal Medicine, Daedong Hosipital, Busan, Korea
- 3Department of Pathology, Pusan National University Yangsan Hospital, Yangsan, Korea
- 4Division of Pulmonology, Allergy and Critical Care Medicine, Department of Internal Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea
- 5Division of Infectious Disease, Department of Internal Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea
- KMID: 2516953
- DOI: http://doi.org/10.4078/jrd.2021.28.3.165
Abstract
- Systemic lupus erythematosus (SLE) may occur in any organ. In patients with SLE, myocarditis is extremely rare and potentially life-threatening. Herein, we report on a patient with lupus myocarditis, diagnosed by myocardial biopsy, immunologic tests, and clinical manifestations. Our findings suggest that securing time for diagnosis via extracorporeal membrane oxygenation and other intensive care is helpful for obtaining a good prognosis.
Figure
-
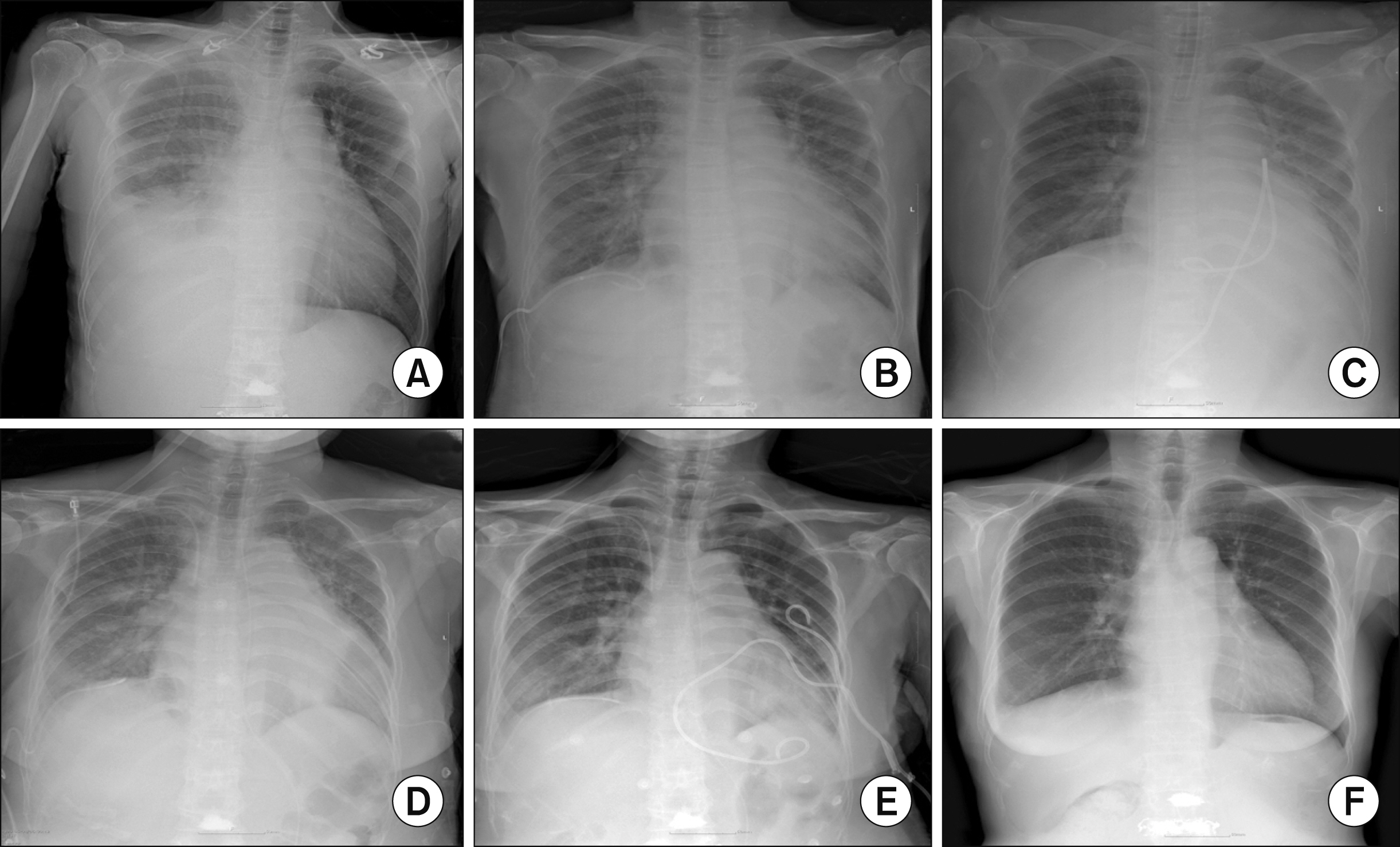
Figure 1 Chest X-rays of the patients over time. (A) At the time of previous hospital admission, 17 days before visit; (B) 1st day of hospitalization; (C) 3rd day of hospitalization (endomyo-cardial biopsy was performed); (D) 12th day of hospitalization (2nd pericardiocentesis was performed due to aggravated pericardial effusion); (E) 21st day of hospitalization (9 days after the restart of steroid therapy); (F) 49th day of hospitalization, at the time of discharge.
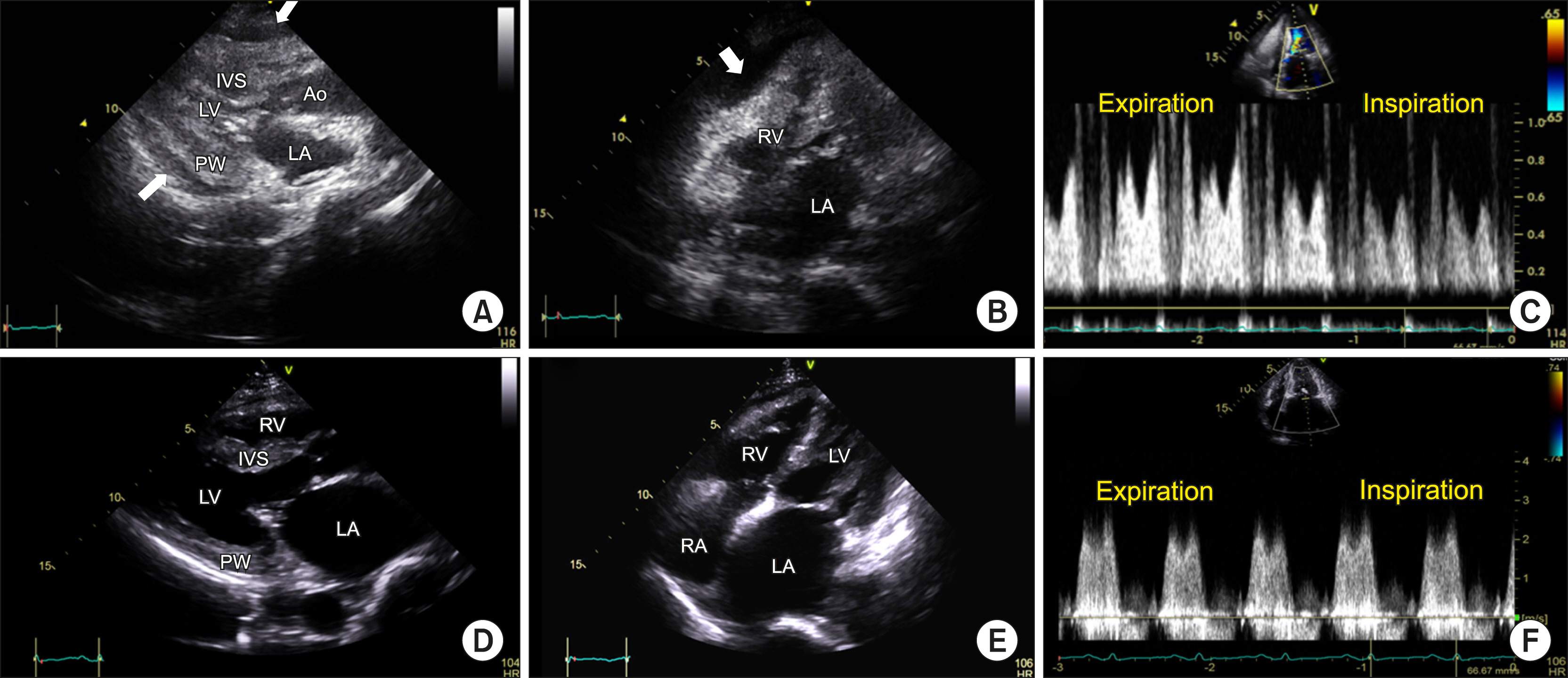
Figure 2 Echocardiogram. Still images (A~C) have been captured after extracorporeal membrane oxygenation and before pericardiocentesis. (A) End diastole of the parasternal long-axis view shows a thickened LV wall with decreased LV cavity; (B) End diastole of the modified four-chamber view. Pericardial effusion compressing the right ventricular lateral wall is seen (arrows in A, B); (C) Mitral inflow pattern; the images (D~F) have been captured 2 weeks after the steroid therapy. (D~F) The ventricular wall thickness returned to the normal range compared with the initial echocardiogram (A). Mitral valvular calcification, thickening, doming, and elevated mean trans-mitral pressure gradient of 5 mmHg suggested concomitant mild mitral stenosis. Ao: ascending aorta, IVS: interventricular septum, LA: left atrium, LV: left ventricular cavity, MV: mitral valve, PW: posterior wall, RV: right ventricle, RA: right atrium.
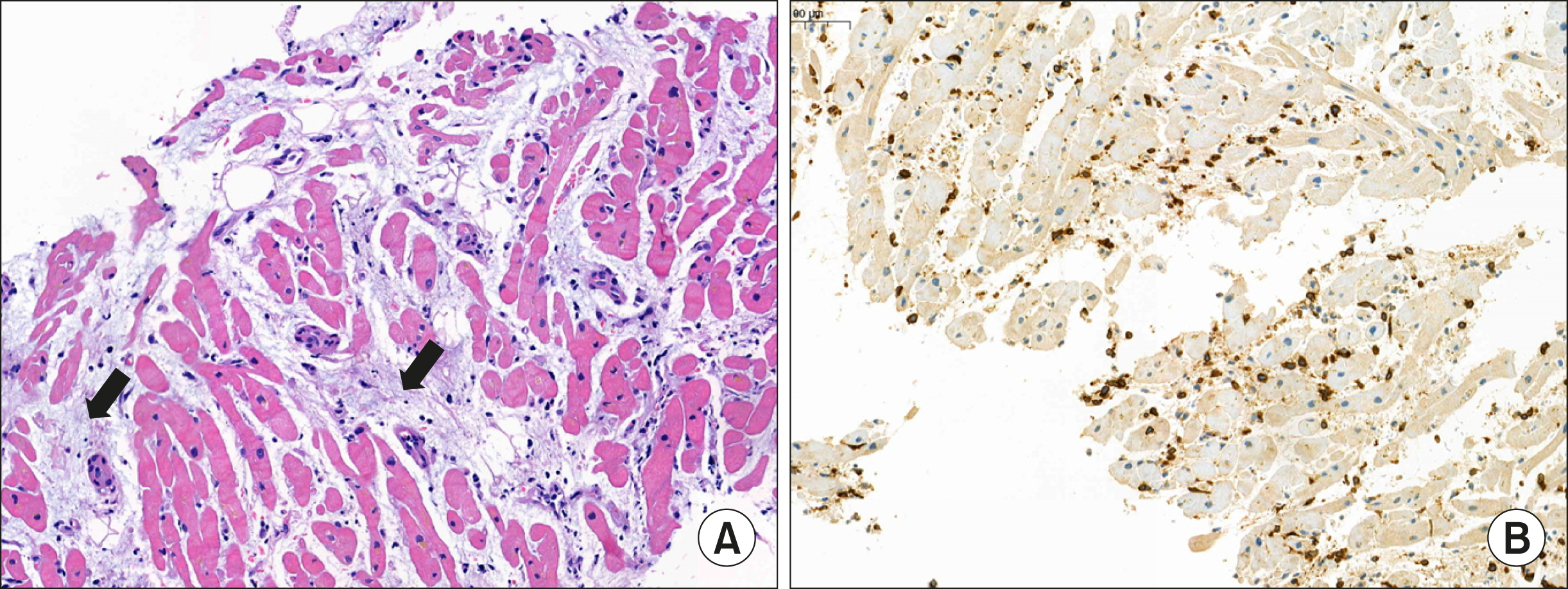
Figure 3 Pathologic findings. (A) Scattered lymphocytes and loss of myocardium replaced by progressive fibrosis (arrows) (H&E stain, ×11); (B) Immuno-histochemistry of CD3. The diffusely scattered lymphocytes have been stained dominantly with CD3 (×11).
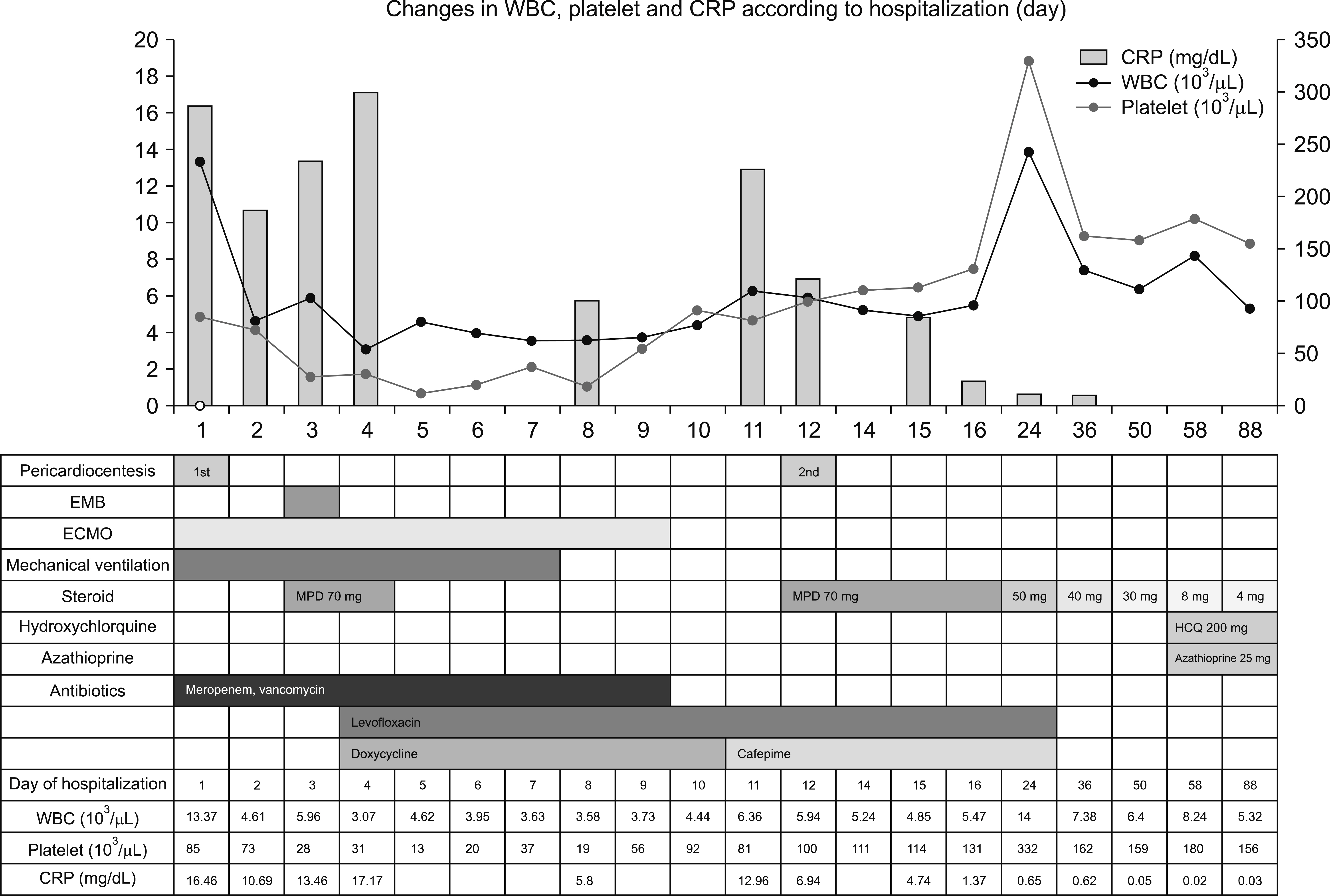
Figure 4 Changes in laboratory findings and treatment according to hospitalization and outpatient follow-up periods. EMB: endomyocardial biopsy, ECMO: extracorporeal membrane oxygenation, MPD: Methylprednisolone, HCQ: hydroxychloroquine, WBC: white blood cell, CRP: C-reactive protein.
Reference
-
1. Chung JW, Joe DY, Park HJ, Kim HA, Park HS, Suh CH. 2008; Clinical characteristics of lupus myocarditis in Korea. Rheumatol Int. 28:275–80. DOI: 10.1007/s00296-007-0414-6. PMID: 17634899.
Article2. Chaudhari D, Madani MA, Balbissi Md KA, Paul TK. 2015; Lupus myocarditis presenting as life-threatening overt heart failure: a case report with review of cardiovascular manifestations of systemic lupus erythematosus. J La State Med Soc. 167:220–2. PMID: 27159597.3. Mohanty B, Sunder A. 2020; Lupus myocarditis-a rare case. J Family Med Prim Care. 9:4441–3. DOI: 10.4103/jfmpc.jfmpc_716_20. PMID: 33110880. PMCID: PMC7586557.
Article4. Wijetunga M, Rockson S. 2002; Myocarditis in systemic lupus erythematosus. Am J Med. 113:419–23. DOI: 10.1016/S0002-9343(02)01223-8. PMID: 12401537.
Article5. Doria A, Iaccarino L, Sarzi-Puttini P, Atzeni F, Turriel M, Petri M. 2005; Cardiac involvement in systemic lupus erythematosus. Lupus. 14:683–6. DOI: 10.1191/0961203305lu2200oa. PMID: 16218467.
Article6. Thomas G, Cohen Aubart F, Chiche L, Haroche J, Hié M, Hervier B, et al. 2017; Lupus myocarditis: initial presentation and longterm outcomes in a multicentric series of 29 patients. J Rheumatol. 44:24–32. DOI: 10.3899/jrheum.160493. PMID: 28042125.
Article7. Miner JJ, Kim AH. 2014; Cardiac manifestations of systemic lupus erythematosus. Rheum Dis Clin North Am. 40:51–60. DOI: 10.1016/j.rdc.2013.10.003. PMID: 24268009.
Article8. Gartshteyn Y, Tamargo M, Fleischer S, Kapoor T, Li J, Askanase A, et al. 2020; Endomyocardial biopsies in the diagnosis of myocardial involvement in systemic lupus erythematosus. Lupus. 29:199–204. DOI: 10.1177/0961203319897116. PMID: 31924147. PMCID: PMC7261237.
Article9. Kociol RD, Cooper LT, Fang JC, Moslehi JJ, Pang PS, Sabe MA, et al. 2020; Recognition and initial management of fulminant myocarditis: a scientific statement from the American Heart Association. Circulation. 141:e69–92. DOI: 10.1161/CIR.0000000000000745. PMID: 31902242.
Article10. Barrie M, McKnight L, Solanki P. 2012; Rapid resolution of acute fulminant myocarditis after IVIG and steroid treatment. Case Rep Crit Care. 2012:262815. DOI: 10.1155/2012/262815. PMID: 24826334. PMCID: PMC4010038.
Article11. Saito T, Katayama H, Kodani E. 2019; Is steroid therapy really banned for lymphocytic myocarditis before excluding viral infection? Eur Heart J. 40:1014–5. DOI: 10.1093/eurheartj/ehy738. PMID: 30403793.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Use of Extracorporeal Membrane Oxygenation in Diffuse Alveolar Hemorrhage Secondary to Systemic Lupus Erythematosus
- Anesthetic management of cesarean delivery of parturient with systemic lupus erythematosus associated with pulmonary arterial hypertension - A case report -
- Myopericarditis in a Korean Young Male With Systemic Lupus Erythematosus
- Blood Transfusion Strategies in Patients Supported by Extracorporeal Membrane Oxygenation
- A case of rescuing a patient with acute cardiovascular instability from sudden and massive intraoperative pulmonary thromboembolism by extracorporeal membrane oxygenation
