Myopericarditis in a Korean Young Male With Systemic Lupus Erythematosus
- Affiliations
-
- 1Department of Internal Medicine, Hallym University College of Medicine, Chuncheon, Korea. kshong@hallym.ac.kr
- KMID: 1776192
- DOI: http://doi.org/10.4070/kcj.2011.41.6.334
Abstract
- Myocardial involvement with clinical symptoms is a rare manifestation of systemic lupus erythematosus (SLE), despite the relatively high prevalence of myocarditis at autopsies of SLE patients. In this review, we report the case of a 19-year-old male SLE patient who initially presented with myopericarditis and was successfully treated with high dose of glucocorticoids.
Keyword
MeSH Terms
Figure
-

Fig. 1 Chest X-ray. A: chest X-ray shows patchy consolidation with multiple nodular densities in both the lower lung fields and cardiomegaly. B: chest X-ray following treatment with steroids shows improving consolidation and cardiomegaly.
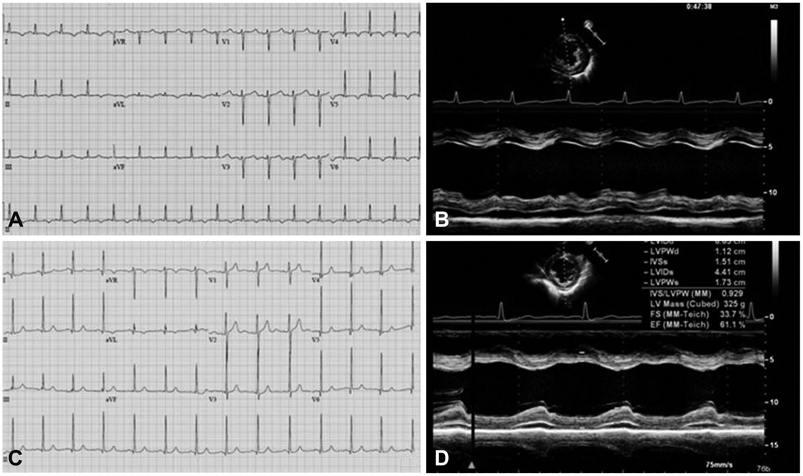
Fig. 2 Electrocardiogram and Echocardiogram. A: electorcardiogram (ECG) shows sinus tachycardia and diffuse T-wave inversion in which leads on the day of admission. B: parasternal short axis view shows pericardial effusion and decreased left ventricular ejection fraction. C: ECG shows normal sinus rhythm and left ventricular hypertrophy after glucocorticoid treatment. D: parasternal short axis views show improving left ventricular ejection fraction and decreasing pericardial effusion after glucocorticoid treatment.
Reference
-
1. Tan EM, Cohen AS, Fries JF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus (SLE). Arthritis Rheum. 1982. 25:1271–1277.2. Chakravarty EF, Bush TM, Manzi S, Clarke AE, Ward MM. Prevalence of adult systemic lupus erythematosus in California and Pennsylvania in 2000: estimates obtained using hospitalization data. Arthritis Rheum. 2007. 56:2092–2094.3. Lahita RG. The role of sex hormones in systemic lupus erythematosus. Curr Opin Rheumatol. 1999. 11:352–356.4. Wijetunga M, Rockson S. Myocarditis in systemic lupus erythematosus. Am J Med. 2002. 113:419–423.5. Doria A, Iaccarino L, Sarzi-Puttini P, Atzeni F, Turriel M, Petri M. Cardiac involvement in systemic lupus erythematosus. Lupus. 2005. 14:683–686.6. Bidani AK, Roberts JL, Schwartz MM, Lewis EJ. Immunopathology of cardiac lesions in fatal systemic lupus erythematosus. Am J Med. 1980. 69:849–858.7. Mandell BF. Cardiovascular involvement in systemic lupus erythematosus. Semin Arthritis Rheum. 1987. 17:126–141.8. Moder KG, Miller TD, Tazellar HD. Cardiac involvement in systemic lupus erythematosus. Mayo Clin Proc. 1999. 74:275–284.9. Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000. 343:1388–1398.10. Murphy JG, Franz RP. Cooper LT, editor. Endomyocardial biopsy in myocarditis. Myocarditis: From Bench to Bedside. 2003. Totowa, NJ: Humana, Press;371–389.11. Noutsias M, Pauschinger M, Poller WC, Schultheiss HP, Kühl U. Current insights into the pathogenesis, diagnosis and therapy of inflammatory cardiomyopathy. Heart Fail Monit. 2003. 3:127–135.12. Park JI, Jeon ES. Mechanical circulatory supports in the treatment of fulminent myocarditis. Korean Circ J. 2005. 35:563–572.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Of Systemic Lupus Erythematosus Associated With Hyperthyroidism And Severe Retinopathy
- A Case of Transverse Myelitis as a First Manifestation of Systemic Lupus Erythematosus
- A Case of Lupus Enteritis That Developed during the Treatment of Systemic Lupus Erythematosus
- Multiple Dermatofibromas in a woman with Systemic Lupus Erythematosus
- Lupus Erythematosus Profundus Associated with Kikuchi's Disease
