Korean J Transplant.
2021 Mar;35(1):48-52. 10.4285/kjt.20.0041.
Posttransplantation tuberculosis management in terms of immunosuppressant cost: a case report in Myanmar
- Affiliations
-
- 1Department of Nephrology, University of Medicine, Mandalay, Mandalay, Myanmar
- 2Department of Pharmacology, University of Medicine, Mandalay, Mandalay, Myanmar
- 3Department of Nephrology, Mandalay General Hospital, Mandalay, Myanmar
- KMID: 2514408
- DOI: http://doi.org/10.4285/kjt.20.0041
Abstract
- Drug interactions between anti-tuberculosis and immunosuppressive medications after renal transplantation are a common problem in Myanmar. The efficacy of both types of drugs can be reduced during the treatment period, which can lead to graft failure and flare-ups of infection. Drug adjustments, with frequent monitoring and close follow-up, are crucial in this period. Ketoconazole decreases tacrolimus metabolism by inhibiting cytochrome P450-3A5 enzymes and P-glycoprotein. It is cost effective and has been frequently used to reduce the dose and cost of tacrolimus. Here, we report the case of a 56-year-old male renal transplant recipient with anti-tuberculosis medications.
Figure
-

Fig. 1 Chest radiograph of the patient.

Fig. 2 Computed tomography scan of the patient. (A) Speculated mass lesion in right lower segments and air space opacity with internal air bronchogram. (B) Consolidation in anterior segment of right upper lobe. (C) Soft tissue lesion in right lung field with speculated margin.
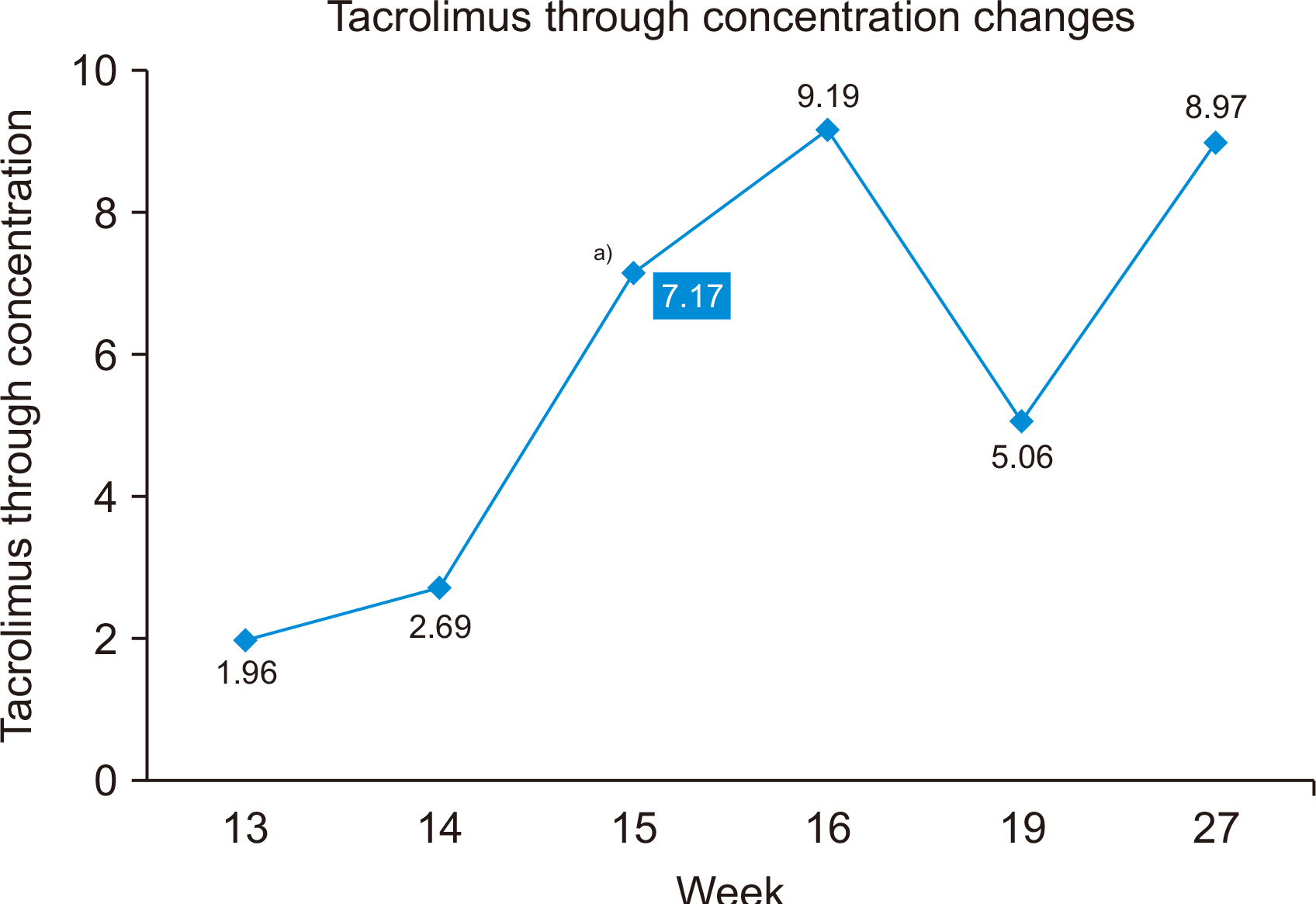
Fig. 3 Changes in tacrolimus trough levels. a)Ketoconazole 100 mg bd added.

Fig. 4 Recheck chest radiograph (posteroanterior view) taken 6 months after anti-tuberculosis treatment.
Reference
-
1. Flynn JL, Chan J. 2001; Immunology of tuberculosis. Annu Rev Immunol. 19:93–129. DOI: 10.1146/annurev.immunol.19.1.93. PMID: 11244032.2. Kaufmann SH, Cole ST, Mizrahi V, Rubin E, Nathan C. 2005; Mycobacterium tuberculosis and the host response. J Exp Med. 201:1693–7. DOI: 10.1084/jem.20050842. PMID: 15939785. PMCID: PMC2213264.
Article3. Anand M, Nayyar E, Concepcion B, Salani M, Schaefer H. 2017; Tuberculosis in kidney transplant recipients: a case series. World J Transplant. 7:213–21. DOI: 10.5500/wjt.v7.i3.213. PMID: 28698838. PMCID: PMC5487311.
Article4. Zhang R. 2013; Modern immunosuppressive therapy in kidney transplantation. Open J Organ Transpl Surg. 3:22–31. DOI: 10.4236/ojots.2013.32005.5. Lemahieu WP, Maes BD, Verbeke K, Vanrenterghem Y. 2004; CYP3A4 and P-glycoprotein activity in healthy controls and transplant patients on cyclosporin vs. tacrolimus vs. sirolimus. Am J Transplant. 4:1514–22. DOI: 10.1111/j.1600-6143.2004.00539.x. PMID: 15307840.
Article6. Scholten EM, Cremers SC, Schoemaker RC, Rowshani AT, van Kan EJ, den Hartigh J, et al. 2005; AUC-guided dosing of tacrolimus prevents progressive systemic overexposure in renal transplant recipients. Kidney Int. 67:2440–7. DOI: 10.1111/j.1523-1755.2005.00352.x. PMID: 15882290.
Article7. el-Dahshan KF, Bakr MA, Donia AF, Badr Ael-S, Sobh MA. 2004; Co-administration of ketoconazole to tacrolimus-treated kidney transplant recipients: a prospective randomized study. Nephrol Dial Transplant. 19:1613–7. DOI: 10.1093/ndt/gfh191. PMID: 15034161.
Article8. El-Dahshan KF, Bakr MA, Donia AF, Badr Ael-S, Sobh MA. 2006; Ketoconazole-tacrolimus coadministration in kidney transplant recipients: two-year results of a prospective randomized study. Am J Nephrol. 26:293–8. DOI: 10.1159/000094133. PMID: 16804292.
Article9. Subramanian AK, Morris MI. AST Infectious Diseases Community of Practice. 2013; Mycobacterium tuberculosis infections in solid organ transplantation. Am J Transplant. 13 Suppl 4:68–76. DOI: 10.1111/ajt.12100. PMID: 23465000.10. Chen CH, Lian JD, Cheng CH, Wu MJ, Lee WC, Shu KH. 2006; Mycobacterium tuberculosis infection following renal transplantation in Taiwan. Transpl Infect Dis. 8:148–56. DOI: 10.1111/j.1399-3062.2006.00147.x. PMID: 16913973.
Article11. Melchor JL, Gracida C, Ibarra A. 2002; Increased frequency of tuberculosis in Mexican renal transplant recipients: a single-center experience. Transplant Proc. 34:78–9. DOI: 10.1016/S0041-1345(01)02674-4. PMID: 11959194.
Article12. Marques ID, Azevedo LS, Pierrotti LC, Caires RA, Sato VA, Carmo LP, et al. 2013; Clinical features and outcomes of tuberculosis in kidney transplant recipients in Brazil: a report of the last decade. Clin Transplant. 27:E169–76. DOI: 10.1111/ctr.12077. PMID: 23351041.
Article13. Walsh R, Ortiz J, Foster P, Palma-Vargas J, Rosenblatt S, Wright F. 2008; Fungal and mycobacterial infections after Campath (alemtuzumab) induction for renal transplantation. Transpl Infect Dis. 10:236–9. DOI: 10.1111/j.1399-3062.2007.00292.x. PMID: 18086280.
Article14. Finch CK, Chrisman CR, Baciewicz AM, Self TH. 2002; Rifampin and rifabutin drug interactions: an update. Arch Intern Med. 162:985–92. DOI: 10.1001/archinte.162.9.985. PMID: 11996607.15. Sundaram M, Adhikary SD, John GT, Kekre NS. 2008; Tuberculosis in renal transplant recipients. Indian J Urol. 24:396–400. DOI: 10.4103/0970-1591.42625. PMID: 19468476. PMCID: PMC2684355.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Status of Standard Diagnostics and Treatment for Malaria, Tuberculosis, and Hepatitis in Myanmar
- Epstein-Barr Virus Related Polymorphic Posttransplantation Lymphoproliferative Disease in a Patient with Latent Infection of JC Virus
- Dawn of Theranostics in Myanmar (Dream, Reality, and Constraint)
- A Report of Participation in WHO Seminar on Tuberculosis Management
- Phenotypic and Genotypic Analysis of Anti-Tuberculosis Drug Resistance in Mycobacterium tuberculosis Isolates in Myanmar
