Microsurgical treatment of lateral cavernous sinus wall dural arteriovenous fistula with large venous aneurysm: A case report
- Affiliations
-
- 1Department of Neurosurgery, Asan Medical Center, University of Ulsan, College of Medicine, Seoul, Korea
- 2Department of Radiology, Asan Medical Center, University of Ulsan, College of Medicine, Seoul, Korea
- KMID: 2514337
- DOI: http://doi.org/10.7461/jcen.2020.E2020.08.001
Abstract
- We report a case of lateral cavernous sinus wall dural arteriovenous fistula (DAVF) accompanied large venous aneurysm which is presented intracerebral hemorrhage (ICH). A 58-year-old male patient came to emergency department for acute onset of headache and dysarthria. In brain computed tomography scan, large left temporal lobe ICH was noted. In transfemoral cerebral angiography, multiple arteries from external carotid artery and left internal carotid artery (ICA) fed arteriovenous shunt. This shunt was drained through cavernous sinus with enlarged multiple cortical veins. One large venous aneurysm was estimated as bleeding focus for ICH. Considering ICH and high flow shunt, we planned urgent treatment to reduce flow of arteriovenous shunt. However, transvenous embolization was failed due to tortuous venous anatomy. Therefore, we planned craniotomy and microsurgical treatment. There was engorged small vessel in lateral wall of cavernous sinus and vascular trunk which is fistulous connection was noted. Fistula connection was obliterated and disconnected after coagulation. In postoperative image, fistula was completely disappeared and there was no cortical venous reflux, also large venous aneurysm was disappeared. Patient recovered very well without new neurological deficits. We reported successfully treated lateral cavernous sinus wall DAVF by combined endovascular and transcranial-microsurgical treatment.
Figure
-
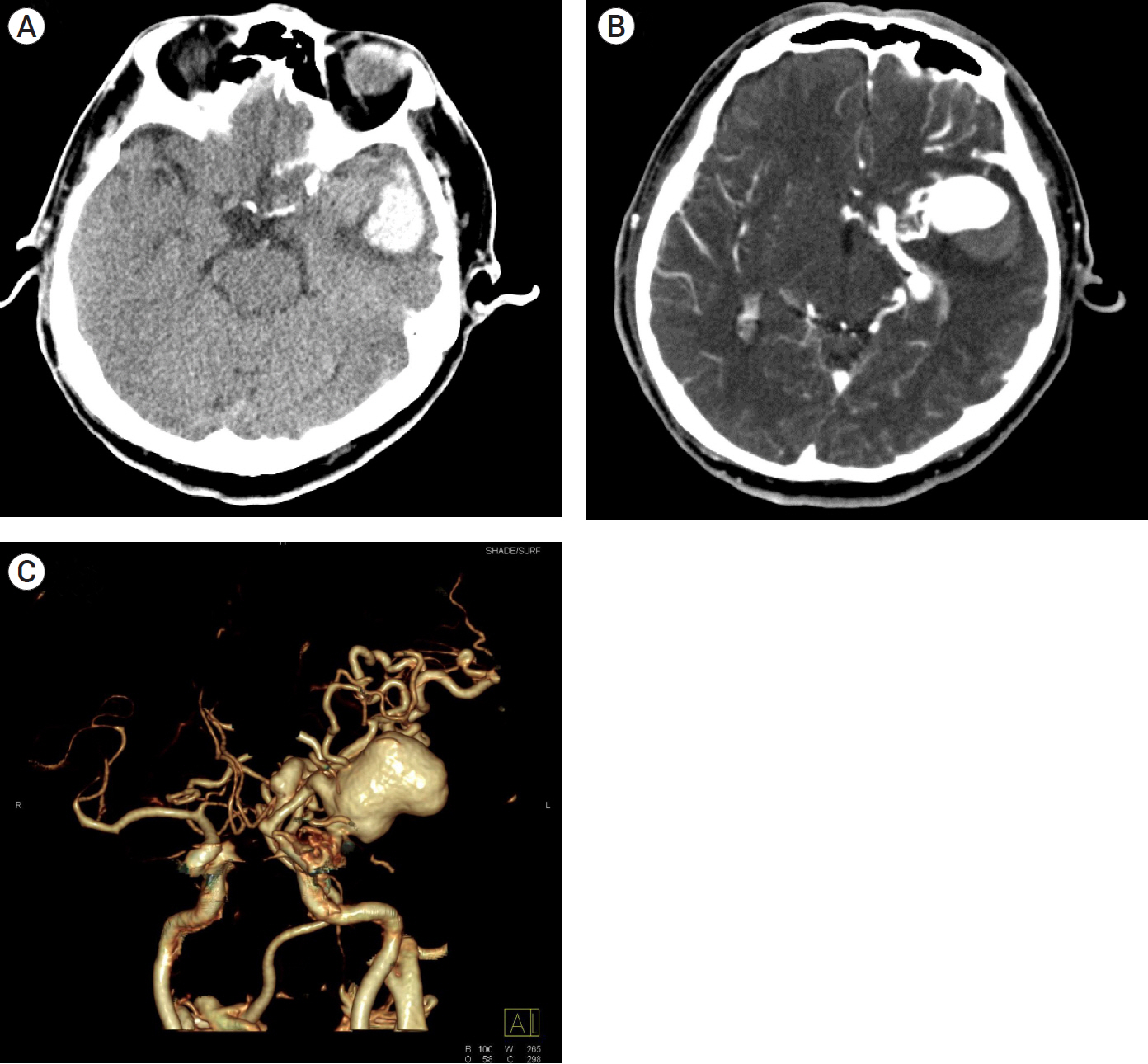
Fig. 1. Initial brain computed tomography (CT) angiography of lateral cavernous sinus wall dural arteriovenous fistula. (A) Left temporal lobe intracerebral hemorrhage was seen on non-contrast brain CT scan. Slight high density lesion was located in medial portion of hematoma. (B), (C) Contrast enhanced CT scan showed engorged venous structure and large venous aneurysm in anterior and medial temporal lobe. Complex interlacing vascular structure were seen in lateral area of cavernous segment of internal carotid artery.
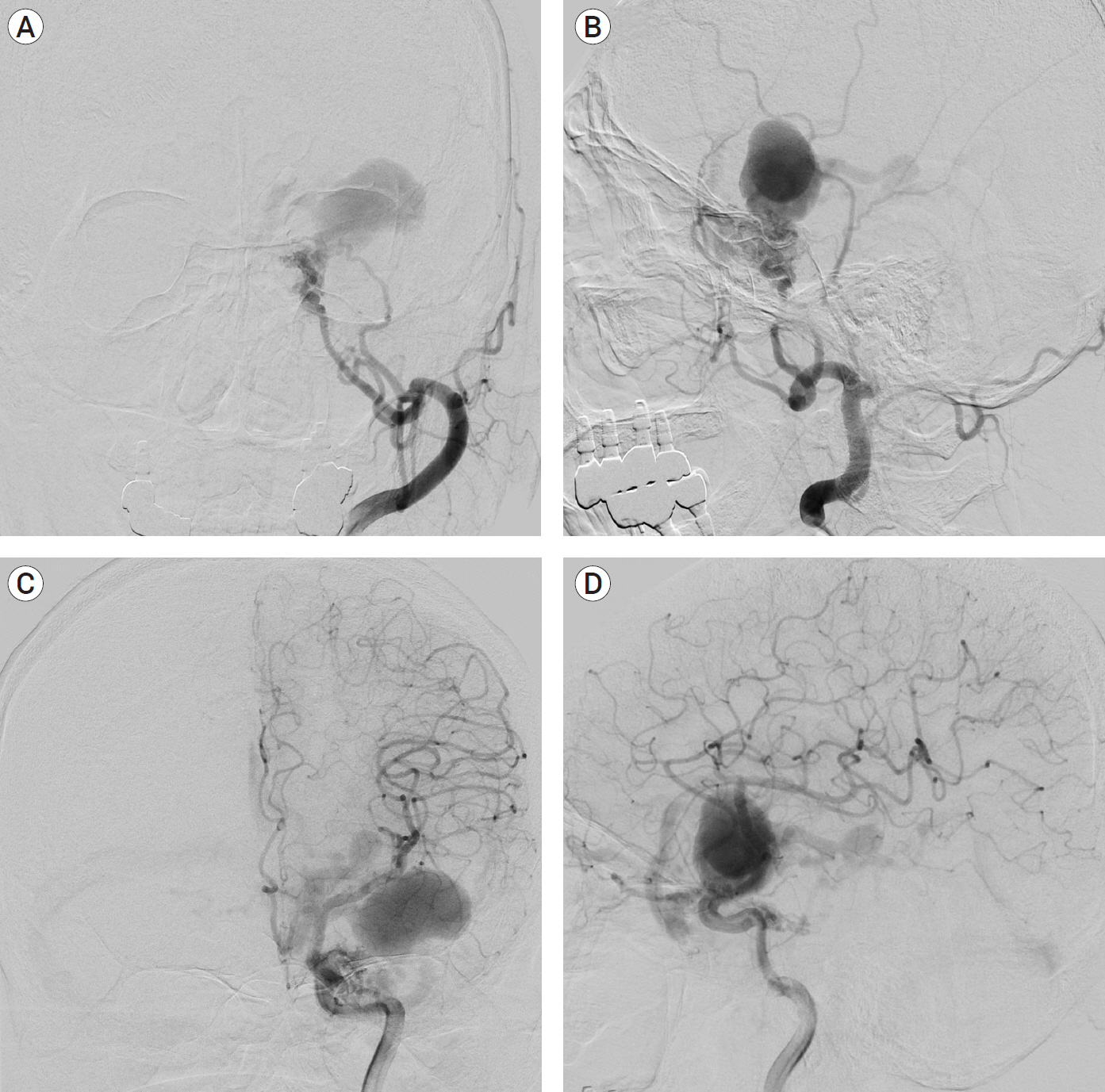
Fig. 2. Initial cerebral angiographic findings of lateral cavernous sinus wall dural arteriovenous fistula (DAVF). (A), (B) External carotid artery angiogram: DAVF was fed by middle meningeal and accessory arteries. Shunt flow was drained by basal vein of Rosenthal and superficial middle cerebral vein. (C), (D) Internal carotid artery angiogram: inferolateral trunk of cavernous segment of internal carotid artery and recurrent branches of ophthalmic artery. Middle cerebral artery was displaced superiorly. Large venous aneurysm of superficial middle cerebral vein was seen.
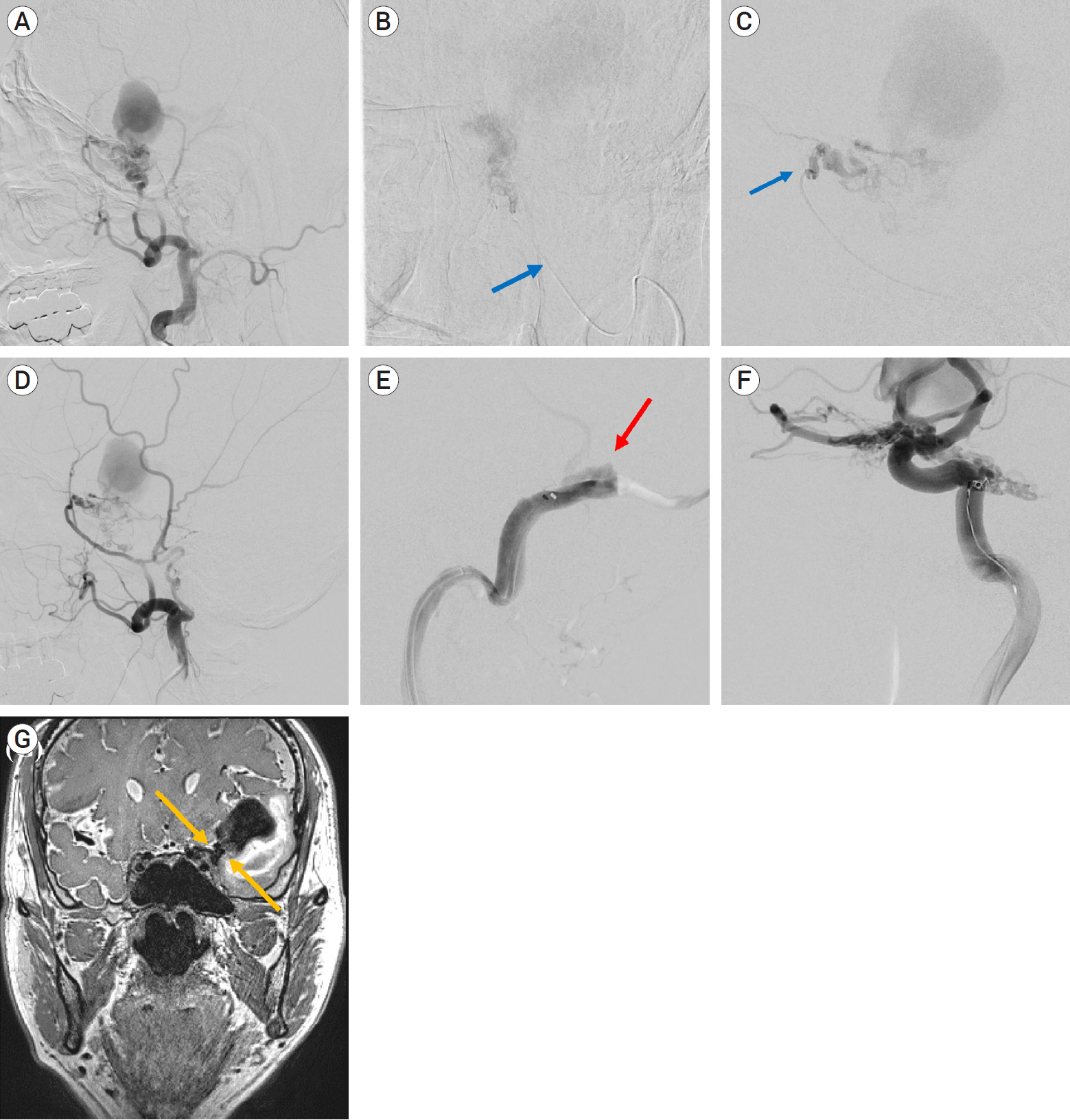
Fig. 3. Preoperative embolization and brain magnetic resonance imaging (MRI) finding of dural arteriovenous fistula (DAVF). (A) Pre-embolization external carotid artery angiogram. (B) Super-selection angiogram of middle meningeal artery for Glue embolization (arrow: tip of microcatheter) (C) Super-selection angiogram of accessory meningeal artery (arrow: tip of microcatheter) (D): after glue embolization of middle meningeal artery. Shunt flow was dramatically reduced. (E) Venous approach through transverse sinus. Transvenous approach to DAVF was failed due to acute angle and complex anatomy between transverse sinus, vein of Labbe and tentorial sinus (arrow). (F) Preoperative coil embolization of inferolateral trunk feeders of DAVF. (G) Coronal view of t2-weighted MRI. Common venous trunk (=fistulous connection) was seen in the lateral wall of cavernous sinus (arrow).
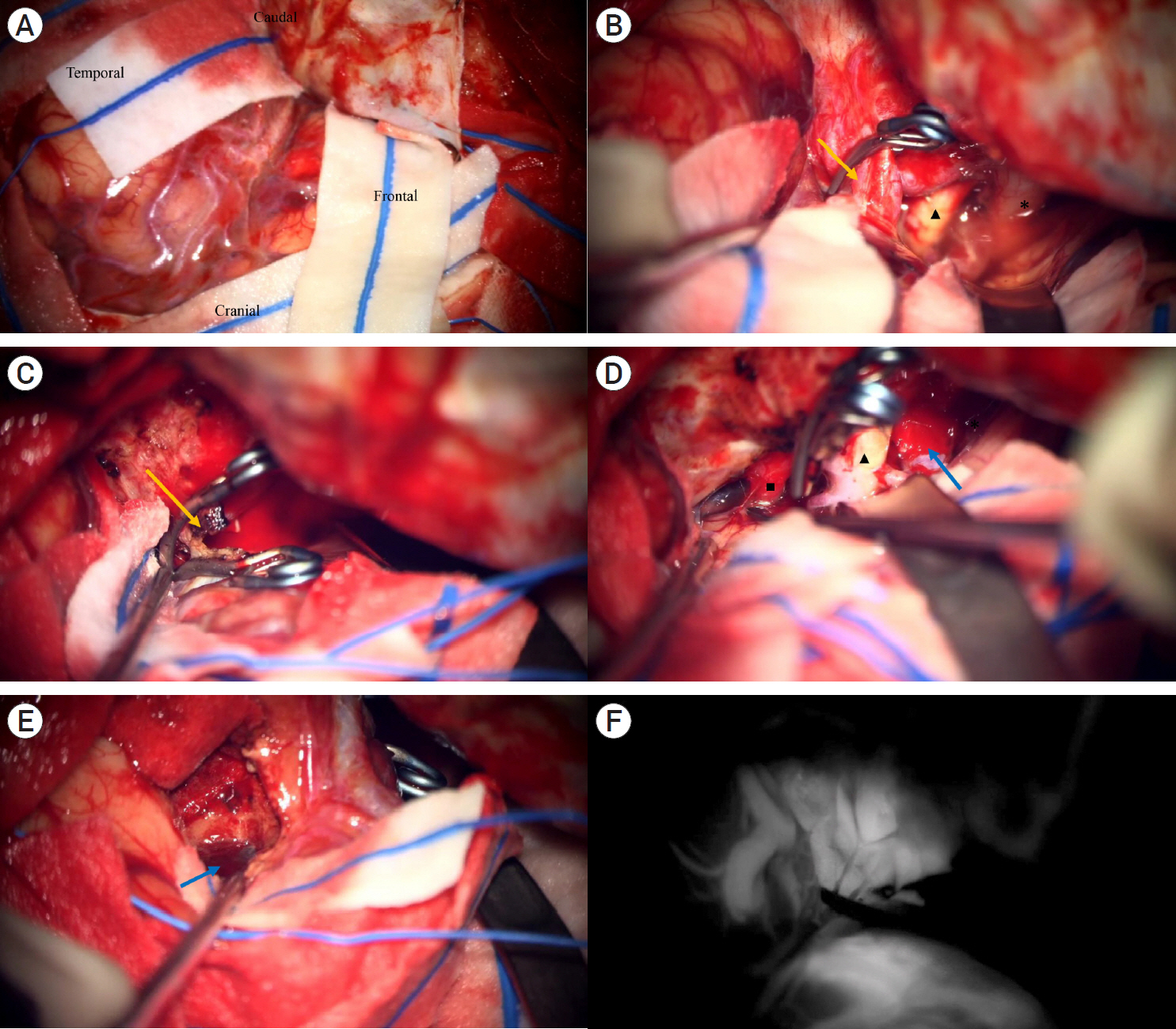
Fig. 4. Intraoperative photography of lateral cavernous sinus wall dural arteriovenous fistula. (A) Frontotemporal zygomatic osteotomy was performed for skull base approach. (B) Fistulous connection was seen in lateral area of internal carotid artery. It located in the lateral wall of cavernous sinus. Engorged vessel was seen in the surface of lateral wall of cavernous sinus. Vascular clip was placed in the connection of fistula. (C) Fistula connection was disconnected after coagulation. (D) Further exploration was performed temporal base dura and tentorial edge. There was no additional abnormal vascular structure. (arrow: one enlarged branch of basal vein). (E) Evacuation of intracerebral hematoma of temporal lobe. (arrow: Shrunken wall of venous aneurysm was noted in hematoma cavity). (F) Indocyanine green videoangiogram of venous trunk. Venous trunk and reflux venous flow through superficial middle cerebral vein were visualized in early arterial phase. *: optic nerve, ▲: internal carotid artery, ■: oculomotor nerve.
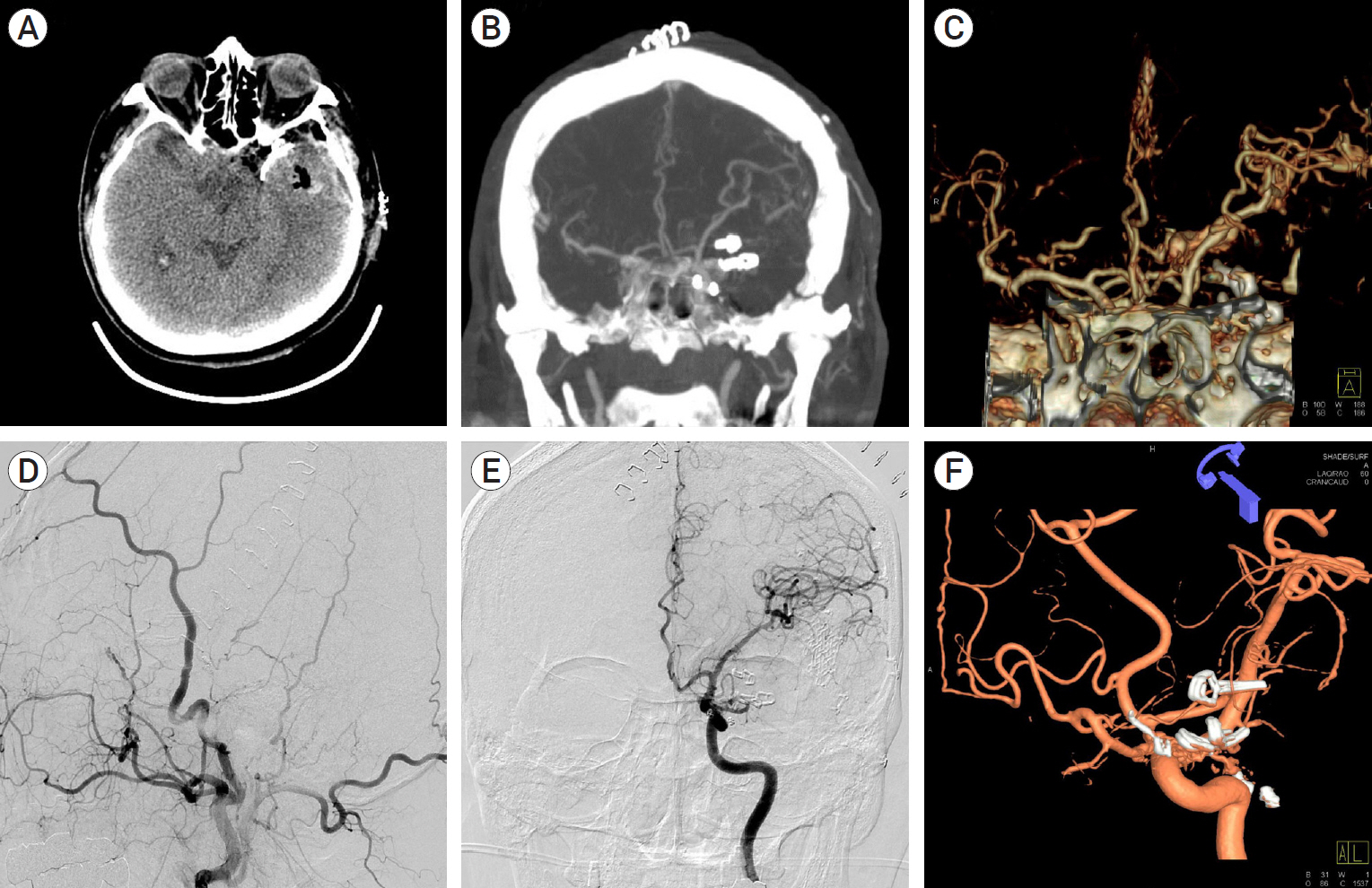
Fig. 5. Postoperative brain computed tomography (CT) and trans femoral cerebral angiography (TFCA). (A-C) Postoperative CT scan: Temporal lobe hematoma was totally removed. Engorged vein and venous aneurysm could not be seen on the postoperative images. (D-F) Postoperative TFCA: complete disconnection of dural arteriovenous fistula was confirmed on both external and internal carotid artery angiograms.
Reference
-
1. Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995; Feb. 82(2):166–79.
Article2. Cognard C, Januel AC, Silva NA Jr, Tall P. Endovascular treatment of intracranial dural arteriovenous fistulas with cortical venous drainage: new management using Onyx. AJNR Am J Neuroradiol. 2008; Feb. 29(2):235–41.
Article3. Daniels DJ, Vellimana AK, Zipfel GJ, Lanzino G. Intracranial hemorrhage from dural arteriovenous fistulas: clinical features and outcome. Neurosurg Focus. 2013; May. 34(5):E15.
Article4. Gandhi D, Chen J, Pearl M, Huang J, Gemmete JJ, Kathuria S. Intracranial dural arteriovenous fistulas: classification, imaging findings, and treatment. AJNR Am J Neuroradiol. 2012; Jun. 33(6):1007–13.
Article5. Lamin S, Chew HS, Chavda S, Thomas A, Piano M, Quilici L, et al. Embolization of intracranial dural arteriovenous fistulas using PHIL liquid embolic agent in 26 patients: a multicenter study. AJNR Am J Neuroradiol. 2017; Jan. 38(1):127–31.
Article6. Roy D, Raymond J. The role of transvenous embolization in the treatment of intracranial dural arteriovenous fistulas. Neurosurgery. 1997; Jun. 40(6):1133–41. discussion 1141.
Article7. Tomak PR, Cloft HJ, Kaga A, Cawley CM, Dion J, Barrow DL. Evolution of the management of tentorial dural arteriovenous malformations. Neurosurgery. 2003; Apr. 52(4):750–60. discussion 60-2.
Article8. Uchiyama T, Horiuchi T, Murata T, Hongo K. Dural arteriovenous fistula between inferolateral trunk of the internal carotid artery and superficial sylvian vein. Neurol Med Chir (Tokyo). 2011; Sep. 51(9):642–4.
Article9. Ushikoshi S, Honma T, Uchida K, Yasuda H, Ajiki M. Dural arteriovenous fistula at the anterior clinoid process draining directly into the superficial middle cerebral vein. Neurol Med Chir (Tokyo). 2013; Mar. 53(3):195–8.
Article10. Watanabe J, Maruya J, Nishimaki K. Surgical treatment of a dural arteriovenous fistula in the sphenoid wing with a unique drainage pattern through the basal vein of Rosenthal. NMC Case Rep J. 2015; Jun. 2(3):88–92.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistula Using the Direct Superior Ophthalmic Vein Approach: A Case Report
- Borden Type I Sigmoid Sinus Dural Arteriovenous Fistula Presenting as Subarachnoid Hemorrhage from a Feeding Artery Aneurysm of the Anterior Inferior Cerebellar Artery: A Case Report
- Endovascular management of cavernous sinus dural arteriovenous fistulas: Overall review and considerations
- A Case of Dural Arterio-venous Malformation Involving the Cavernous Sinus
- Surgical Treatment of Carotid-Cavernous Fistula and Intracranial Dural Arteriovenous Malformations
