Surgical Treatment of Ten Adults with Spinal Extradural Meningeal Cysts in the Thoracolumbar Spine
- Affiliations
-
- 1Department of Neurosurgery, Peking University First Hospital, Beijing, China
- 2Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, China
- KMID: 2513854
- DOI: http://doi.org/10.3340/jkns.2020.0244
Abstract
Objective
: To retrospectively analyze the clinical characteristics and surgical experience of 10 adults with spinal extradural meningeal cysts (SEMCs) in the thoracolumbar spine which may further provide evidence for surgical decision-making.
Methods
: Ten adults with SEMCs in the thoracolumbar spine were surgically treated and enrolled in this study. Clinical manifestations, imaging data, intraoperative findings and postoperative outcome were recorded.
Results
: Clinical manifestations of SEMCs included motor and sensory dysfunction of the lower limbs and urination and defecation disturbance. The cysts presented as intraspinal occupying lesions dorsal to the spine, ranging from the T8 to L3 level. Defects of eight cases were found on preoperative magnetic resonance imaging (MRI). Selective hemilaminectomy or laminectomy were used to reveal the defect within the cyst, which was further sutured with microscopic technique. The final outcome was excellent or good in seven cases and fair in three cases. No recurrence was observed during follow-up.
Conclusion
: SEMCs are rare intraspinal cystic lesions. Radiography and MRI are clinically practical methods to assess defects within SEMCs. Selective hemilaminectomy or laminectomy may reduce surgical trauma. Detection and microscopic suturing of the defects are the key steps to adequately decompress the nervous tissue and prevent postoperative recurrence.
Figure
-
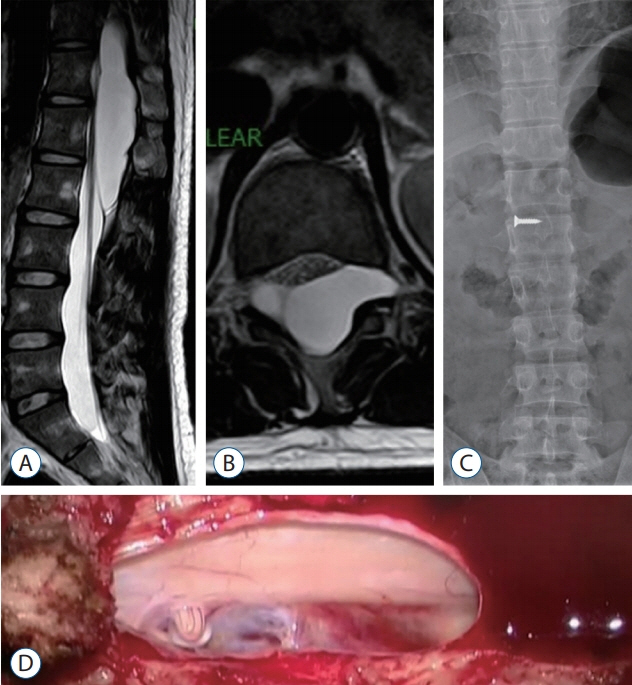
Fig. 1. Case No. 12. A : Sagittal T2-weighted MR image demonstrates a cyst extending from T11 to L2 with dorsal compression of the spinal cord and cauda equina. B : Axial T2-weighted image reveals cyst extension through the left neural foramina. C : Anteroposterior radiography shows narrowing of bilateral vertebral pedicles from T12 to L1 (nail pointed to spinous process of T12). D : Nerve root fiber moves back and forth via the dural defect.
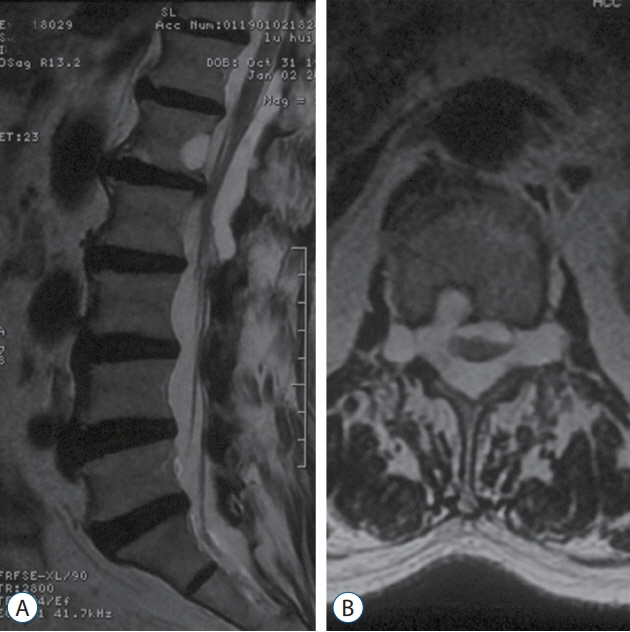
Fig. 2. Case No. 7. A : Sagittal T2-weighted magnetic resonance image demonstrates an irregular cyst extending from T12 to L2 with dorsal compression of the spinal cord. B : Axial T2-weighted image shows a bony erosion in the back of L1 vertebral body (right side) by spinal extradural meningeal cyst and enlargement of bilateral intervertebral foramens.
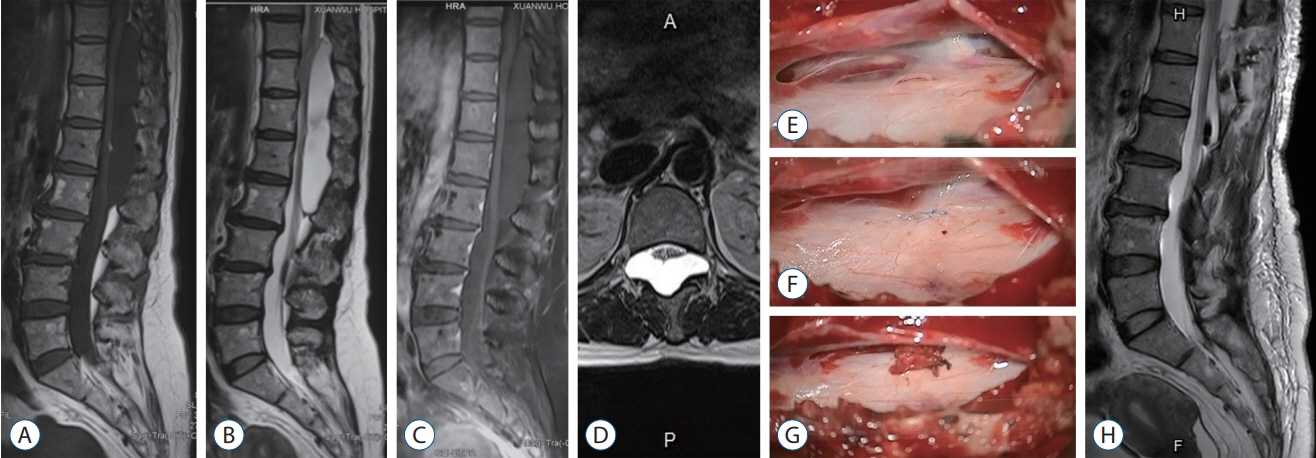
Fig. 3. Case No. 3. A-C : A cyst extended from T10 to L2 with dorsal compression of the spinal cord. All SEMCs shows homogenous low-intensity signals on T1-weighted MRI and high-intensity signals on T2-weighted MRI. No enhancement is demonstrated by contrast agents. A suspected flow void is identified at T12 level. D : Axial T2-weighted image (T12 level) reveals the cyst is larger in the right side. E : Dural defect is identified under T12 nerve root sleeve during surgery, and the nerve root is adherent to the defect. F : Closing of the defect. G : Strengthening with muscle and fibrin sealant at the defect. H : Significant resolution of SEMC and nerve decompression after surgery. SEMC : spinal extradural meningeal cyst, MRI : magnetic resonance imaging.
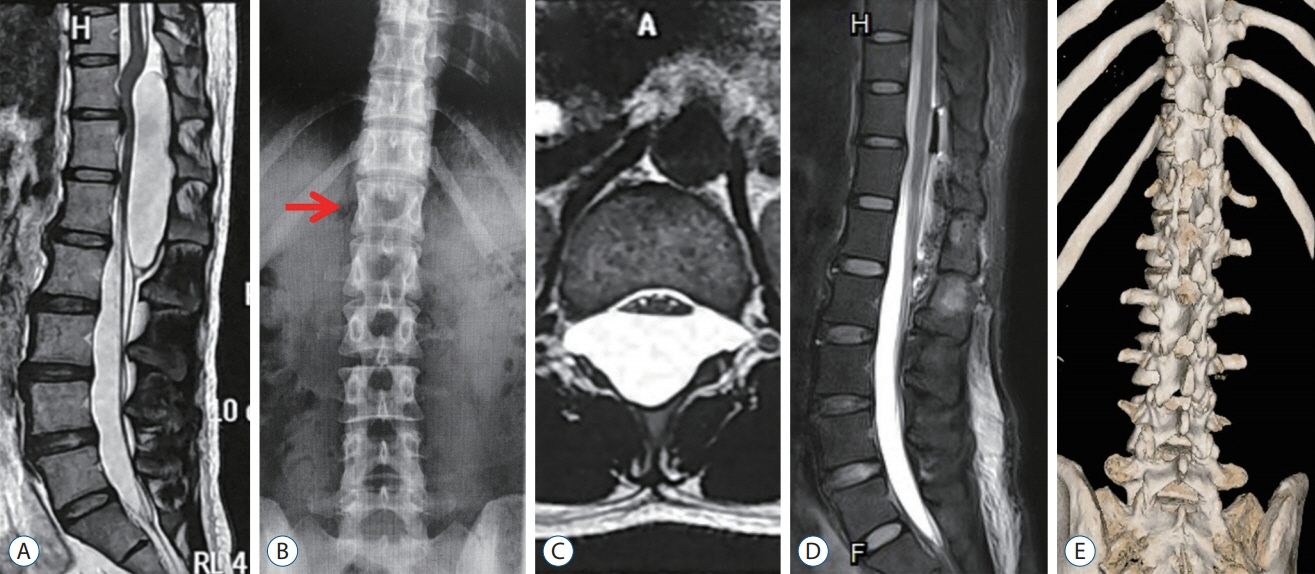
Fig. 4. Case No. 6. A : A cyst extends from T11 to L2 segment. A suspected flow void is identified at T12 level. B : Anteroposterior radiogram demonstrates significant narrowing of left vertebral pedicles of T12 (red arrow). C : However, the cyst presents symmetrically at T12 level on axial T2-weighted image. D : The cyst shranks dramatically and nerve decompression is achieved. E : Postoperative three-dimensional computed tomography reconstruction illustrates the range of hemilaminectomy (from T12 to L2).
Reference
-
References
1. Chen Z, Sun XL, Zhao Y, Wang K, Jian FZ. Dural dissection cyst: a more accurate term for extradural meningeal cyst. CNS Neurosci Ther. 20:515–520. 2014.
Article2. Choi JY, Kim SH, Lee WS, Sung KH. Spinal extradural arachnoid cyst. Acta Neurochir (Wien). 148:579–585. 2006.
Article3. Funao H, Nakamura M, Hosogane N, Watanabe K, Tsuji T, Ishii K, et al. Surgical treatment of spinal extradural arachnoid cysts in the thoracolumbar spine. Neurosurgery. 71:278–284. 2012.
Article4. Furtado SV, Thakar S, Murthy GK, Dadlani R, Hegde AS. Management of complex giant spinal arachnoid cysts presenting with myelopathy. J Neurosurg Spine. 15:107–112. 2011.
Article5. Garg K, Borkar SA, Kale SS, Sharma BS. Spinal arachnoid cysts - our experience and review of literature. Br J Neurosurg. 31:172–178. 2017.
Article6. Gu K, Kwon JW, Kim ES. Digital subtraction cystography for detection of communicating holes of spinal extradural arachnoid cysts. Korean J Radiol. 17:111–116. 2016.
Article7. Hatashita S, Kondo A, Shimizu T, Kurosu A, Ueno H. Spinal extradural arachnoid cyst--case report. Neurol Med Chir (Tokyo). 41:318–321. 2001.8. Ishibe T, Senzoku F, Ikeda N, Kamba Y, Mikawa Y. Detection of the communicating hole(s) of spinal extradural arachnoid cysts using timespatial labeling inversion pulse magnetic resonance imaging. Spine (Phila Pa 1976). 39:E1394–E1397. 2014.
Article9. Ishibe T, Senzoku F, Kamba Y, Ikeda N, Mikawa Y. Time-spatial labeling inversion pulse magnetic resonance imaging of cystic lesions of the spinal cord. World Neurosurg. 88:693.e13–693.e21. 2016.
Article10. Kikuta K, Hojo M, Gomi M, Hashimoto N, Nozaki K. Expansive duraplasty for the treatment of spinal extradural arachnoid cysts: case report. J Neurosurg Spine. 4:251–255. 2006.
Article11. Klekamp J. A new classification for pathologies of spinal meninges, part 1: dural cysts, dissections, and ectasias. Neurosurgery. 81:29–44. 2017.
Article12. Lee CH, Hyun SJ, Kim KJ, Jahng TA, Kim HJ. What is a reasonable surgical procedure for spinal extradural arachnoid cysts: is cyst removal mandatory? Eight consecutive cases and a review of the literature. Acta Neurochir (Wien). 154:1219–1227. 2012.
Article13. Lim MS, Khalil A, Okafo U, Dunlea O, Kaar G. Hemilaminectomy for large spinal extradural meningeal cysts: a case report and review of surgical techniques. Ann R Coll Surg Engl. 98:e162–e164. 2016.
Article14. Liu JK, Cole CD, Kan P, Schmidt MH. Spinal extradural arachnoid cysts: clinical, radiological, and surgical features. Neurosurg Focus. 22:E6. 2007.
Article15. Millward CP, Bhagawati D, Chan HW, Bestwick J, Brecknell JE. Retrospective observational comparative study of hemilaminectomy versus laminectomy for intraspinal tumour resection; shorter stays, lower analgesic usage and less kyphotic deformity. Br J Neurosurg. 29:390–395. 2015.
Article16. Mishra RK, Pruthi N, Bharath RD, Malla BR. Role of intraoperative dynamic magnetic resonance myelogram in management of giant dorsolumbar spinal extradural arachnoid cyst: case report. J Neurosurg Spine. 27:185–188. 2017.
Article17. Miyakoshi N, Hongo M, Kasukawa Y, Shimada Y. Huge thoracolumbar extradural arachnoid cyst excised by recapping T-saw laminoplasty. Spine J. 10:e14–e18. 2010.
Article18. Miyamoto M, Kim K, Matsumoto R, Isobe M, Isu T. Utility of preoperative magnetic resonance imaging myelography for identifying dural defects in patients with spinal extradural arachnoid cysts: case report. Neurosurgery. 59:E941. 2006.
Article19. Morizane K, Fujibayashi S, Otsuki B, Sakamoto T, Tsutsumi R, Odate S, et al. Clinical and radiological features of spinal extradural arachnoid cysts: valve-like mechanism involving the nerve root fiber as a possible cause of cyst expansion. J Orthop Sci. 23:464–469. 2018.
Article20. Nabors MW, Pait TG, Byrd EB, Karim NO, Davis DO, Kobrine AI, et al. Updated assessment and current classification of spinal meningeal cysts. J Neurosurg. 68:366–377. 1988.
Article21. Neo M, Koyama T, Sakamoto T, Fujibayashi S, Nakamura T. Detection of a dural defect by cinematic magnetic resonance imaging and its selective closure as a treatment for a spinal extradural arachnoid cyst. Spine (Phila Pa 1976). 29:E426–E430. 2004.
Article22. Netra R, Min L, Shao Hui M, Wang JC, Bin Y, Ming Z. Spinal extradural meningeal cysts: an MRI evaluation of a case series and literature review. J Spinal Disord Tech. 24:132–136. 2011.23. Oh JK, Lee DY, Kim TY, Yi S, Ha Y, Kim KN, et al. Thoracolumbar extradural arachnoid cysts: a study of 14 consecutive cases. Acta Neurochir. 154:341–348. 2012.
Article24. Qi W, Zhao L, Fang J, Chang X, Xu Y. Clinical characteristics and treatment strategies for idiopathic spinal extradural arachnoid cysts: a single-center experience. Acta Neurochir (Wien). 157:539–545. 2015.
Article25. Tokmak M, Ozek E, Iplikcioglu AC. Spinal extradural arachnoid cysts: a series of 10 cases. J Neurol Surg A Cent Eur Neurosurg. 76:348–352. 2015.
Article26. Tureyen K, Senol N, Sahin B, Karahan N. Spinal extradural arachnoid cyst. Spine J. 9:e10–e15. 2009.
Article27. Woo JB, Son DW, Kang KT, Lee JS, Song GS, Sung SK, et al. Spinal extradural arachnoid cyst. Korean J Neurotrauma. 12:185–190. 2016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noncommunicating Spinal Extradural Meningeal Cyst in Thoracolumbar Spine
- Spinal Extradural Meningeal Cyst: Case Report
- The Spinal Extradural Meningeal Cyst Associated with High Disc Lumbar Herniation: Case Report
- Spinal Extradural Meningeal Cyst in Klippel-Trenaunay Syndrome
- Interdural Cyst of the Thoracolumbar Region
