Do Cardiac Rehabilitation Affect Clinical Prognoses Such as Recurrence, Readmission, Revascularization, and Mortality After AMI?: Systematic Review and Meta-Analysis
- Affiliations
-
- 1Department of Rehabilitation Medicine, Inje University Sanggye Paik Hospital, Seoul, Korea
- 2National Evidence-based Healthcare Collaborating Agency, Seoul, Korea
- 3Department of Rehabilitation Medicine, Kyungpook National University Hospital, Daegu, Korea
- 4Department of Rehabilitation Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- 5Department of Rehabilitation Medicine, Chungnam National University College of Medicine, Daejeon, Korea
- 6Daejeonchungcheong Regional Medical Rehabilitation Center, Chungnam National University Hospital, Daejeon, Korea
- 7Dajeonchungcheong Regional Cardiocerebrovascular Center, Chungnam National University Hospital, Daejeon, Korea
- KMID: 2513231
- DOI: http://doi.org/10.5535/arm.20080
Abstract
Objective
We conducted a systematic review and meta-analysis to analyze the effects of cardiac rehabilitation (CR) on post-discharge prognoses of patients with acute myocardial infarction (AMI).
Methods
A literature search was conducted through four international medical and two Korean databases. Primary outcomes for the effectiveness of CR included all-cause mortality, cardiovascular mortality, recurrence, revascularization, major adverse cardiovascular event, major adverse cardiocerebrovascular event, and readmission. We summarized and analyzed results of studies about CR for AMI, including not only randomized controlled trials (RCTs) but also non-RCTs. We calculated the effect size separately by the study type.
Results
Fourteen articles were finally selected. Of these, two articles were RCTs, while 12 were non-RCTs. In RCTs, the overall mortality rate was lower in the group that participated in CR than that in the conventional care group by 28% (relative risk=0.72; 95% confidence interval, 0.34–1.57). Among non-RCTs, CR participation significantly decreased the overall risk of mortality. Moreover, the rates of recurrence and major adverse cardiovascular events were lower in the group that participated in CR compared to those in the non-CR group.
Conclusion
The meta-analysis shows that CR reduces the risk of re-hospitalization and all-cause mortality after AMI, compared to no participation in CR. This outcome was seen in RCTs as well as in non-RCTs. More studies are necessary for concrete conclusions about the beneficial effects of CR after AMI in various settings.
Figure
-
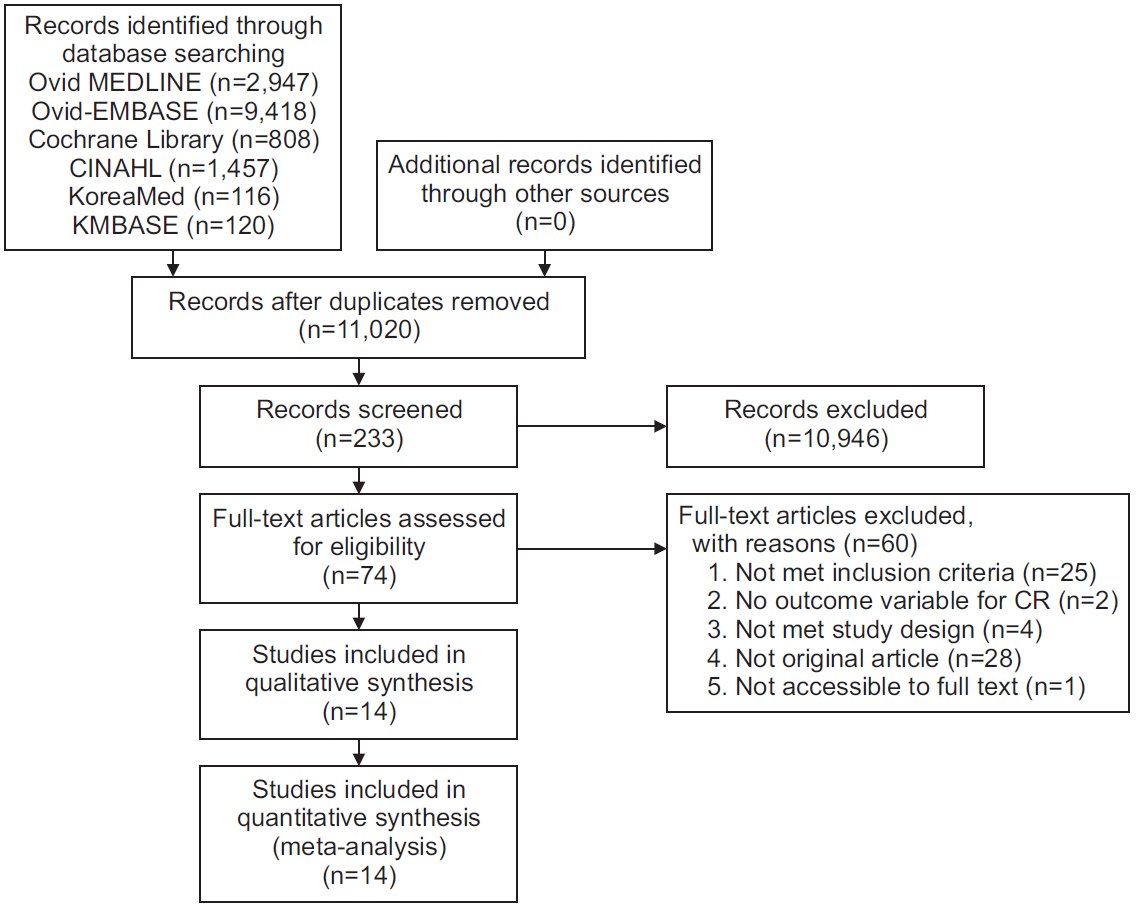
Fig. 1. Summary of study selection process.
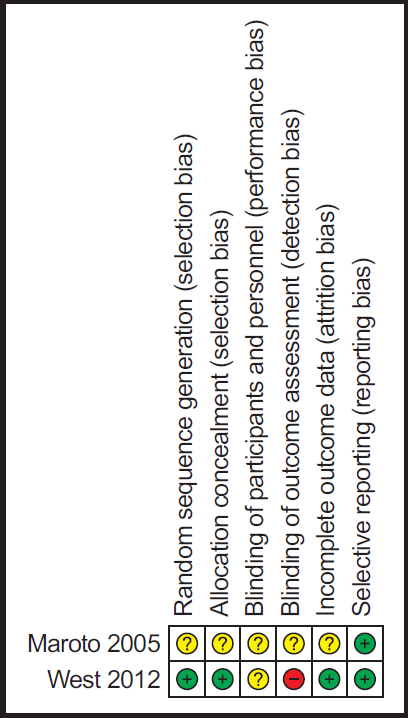
Fig. 2. Summary of risk of bias of the randomized controlled study.
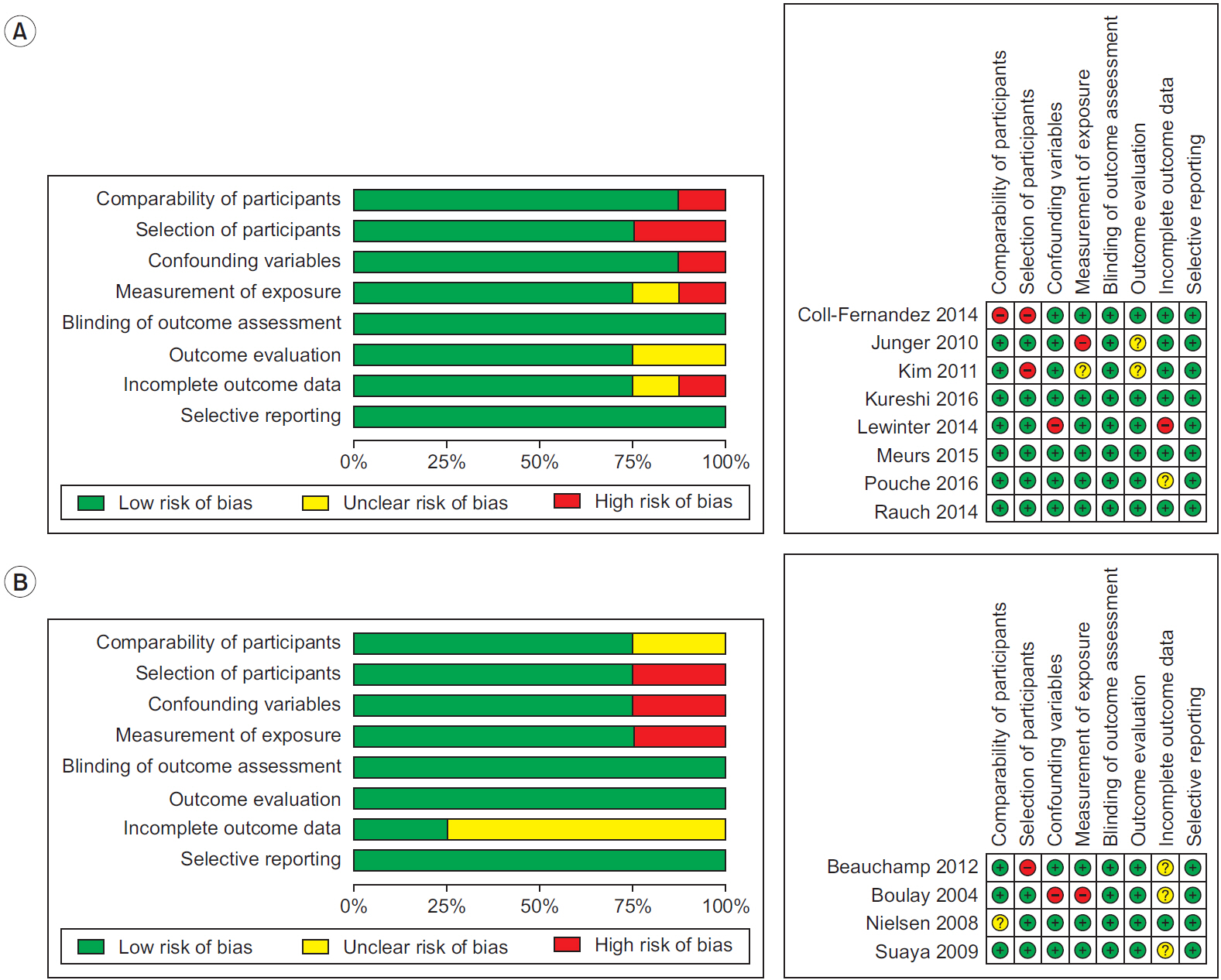
Fig. 3. Summary of risk of bias according to the study design. (A) Prospective cohort study. (B) Retrospective cohort study.
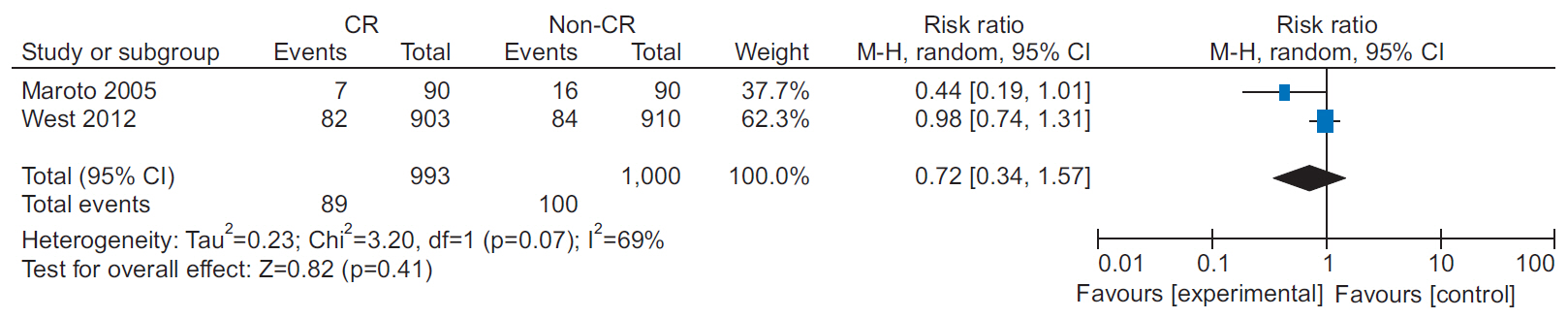
Fig. 4. Forest plot of all-cause mortality in two randomized controlled trials (RCTs). There was a decreased tendency on all-cause mortality in the cardiac rehabilitation (CR) group.
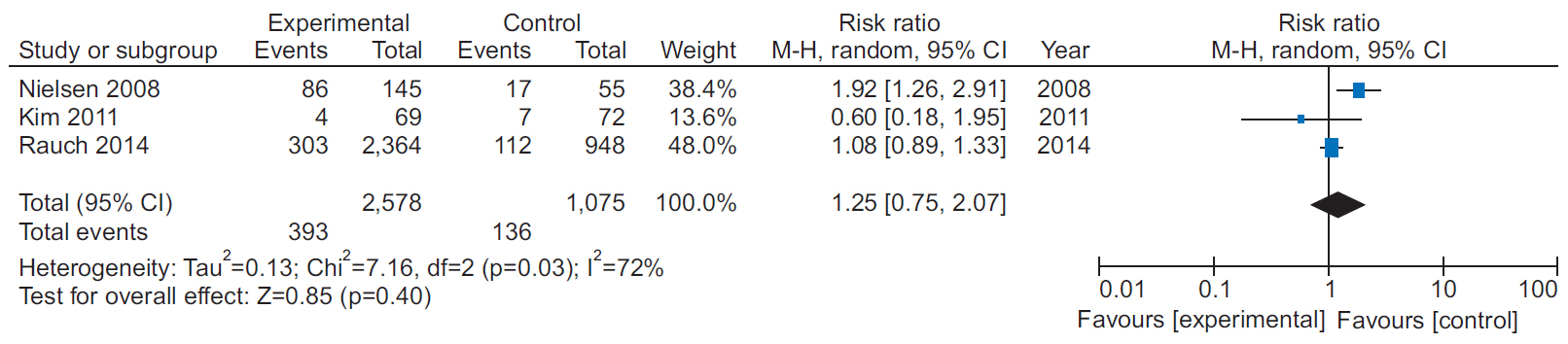
Fig. 5. Forest plot for re-intervention among non-randomized controlled trials (non-RCTs).
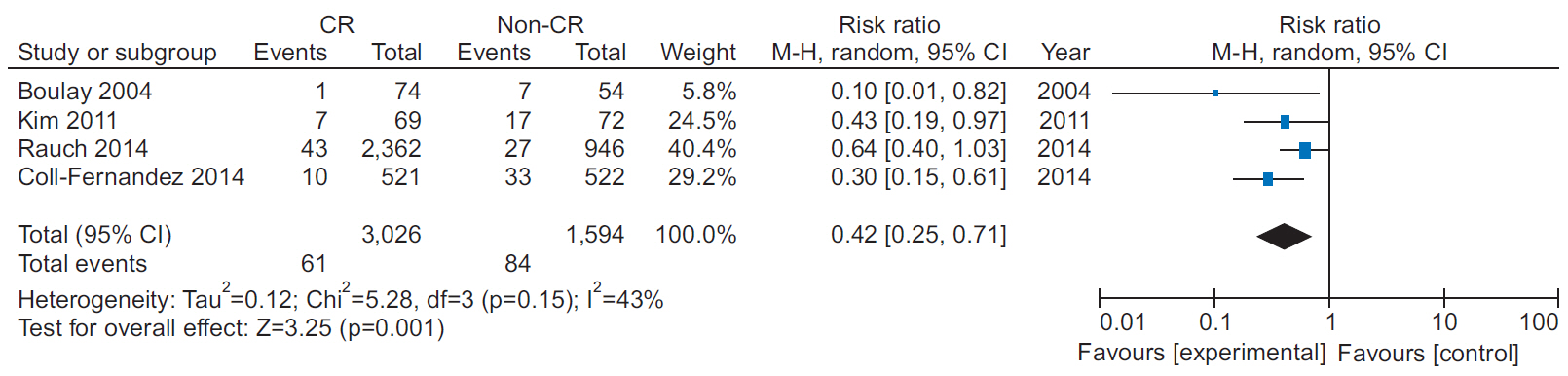
Fig. 6. Forest plot on recurrence after acute myocardial infarction among non-randomized controlled trials (non-RCTs). Cardiac rehabilitation (CR) group showed a significant decrease in recurrence.

Fig. 7. Forest plot on readmission after acute myocardial infarction among non-randomized controlled trials (non-RCTs). CR, cardiac rehabilitation.

Fig. 8. Forest plot on major adverse cardiac and cerebrovascular events after acute myocardial infarction
Cited by 1 articles
-
Fact Sheet on Cardiac Rehabilitation for Cardiovascular Disease in South Korea
Ki-Hong Kim, Jae-Young Han
Ann Rehabil Med. 2023;47(5):318-325. doi: 10.5535/arm.23050.
Reference
-
1. Statistics Korea. 2015 causes of death statistics [Internet]. Daejeon, Korea: Statistics Korea;2016. [cited 2020 Dec 31]. Available from: http://kostat.go.kr/portal/korea/kor_nw/1/6/2/index.board?bmode=read&bSeq=&aSeq=356345&pageNo=1&rowNum=10&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt=.2. Kweon S, Sohn MK, Jeong JO, Kim S, Jeon H, Lee H, et al. Quality of life and awareness of cardiac rehabilitation program in people with cardiovascular diseases. Ann Rehabil Med. 2017; 41:248–56.
Article3. WHO Expert Committee on Rehabilitation of Patients with Cardiovascular Diseases & World Health Organization. Rehabilitation of patients with cardiovascular diseases: report of a WHO Expert Committee (meeting held in Geneva from 23 to 29 July 1963). Geneva, Switzerland: World Health Organization;1964.4. Anderson L, Oldridge N, Thompson DR, Zwisler AD, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016; 67:1–12.5. Rauch B, Davos CH, Doherty P, Saure D, Metzendorf MI, Salzwedel A, et al. The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: a systematic review and meta-analysis of randomized and non-randomized studies. The Cardiac Rehabilitation Outcome Study (CROS). Eur J Prev Cardiol. 2016; 23:1914–39.6. Kim SY, Park JE, Lee YJ, Seo HJ, Sheen SS, Hahn S, et al. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J Clin Epidemiol. 2013; 66:408–14.
Article7. Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011; 64:401–6.
Article8. West RR, Jones DA, Henderson AH. Rehabilitation after myocardial infarction trial (RAMIT): multi-centre randomised controlled trial of comprehensive cardiac rehabilitation in patients following acute myocardial infarction. Heart. 2012; 98:637–44.
Article9. Maroto Montero JM, Artigao Ramirez R, Morales Duran MD, de Pablo Zarzosa C, Abraira V. Cardiac rehabilitation in patients with myocardial infarction: a 10-year follow-up study. Rev Esp Cardiol. 2005; 58:1181–7.
Article10. Pouche M, Ruidavets JB, Ferrieres J, Iliou MC, Douard H, Lorgis L, et al. Cardiac rehabilitation and 5-year mortality after acute coronary syndromes: the 2005 French FAST-MI study. Arch Cardiovasc Dis. 2016; 109:178–87.
Article11. Coll-Fernandez R, Coll R, Pascual T, Sanchez MunozTorrero JF, Sahuquillo JC, Manzano L, et al. Cardiac rehabilitation and outcome in stable outpatients with recent myocardial infarction. Arch Phys Med Rehabil. 2014; 95:322–9.12. Kureshi F, Kennedy KF, Jones PG, Thomas RJ, Arnold SV, Sharma P, et al. Association between cardiac rehabilitation participation and health status outcomes after acute myocardial infarction. JAMA Cardiol. 2016; 1:980–8.
Article13. Kim C, Kim DY, Moon CJ. Prognostic influences of cardiac rehabilitation in Korean acute myocardial infarction patients. Ann Rehabil Med. 2011; 35:375–80.
Article14. Junger C, Rauch B, Schneider S, Liebhart N, Rauch G, Senges J, et al. Effect of early short-term cardiac rehabilitation after acute ST-elevation and non-ST-elevation myocardial infarction on 1-year mortality. Curr Med Res Opin. 2010; 26:803–11.15. Rauch B, Riemer T, Schwaab B, Schneider S, Diller F, Gohlke H, et al. Short-term comprehensive cardiac rehabilitation after AMI is associated with reduced 1-year mortality: results from the OMEGA study. Eur J Prev Cardiol. 2014; 21:1060–9.
Article16. Lewinter C, Bland JM, Crouch S, Doherty P, Lewin RJ, Kober L, et al. The effect of referral for cardiac rehabilitation on survival following acute myocardial infarction: a comparison survival in two cohorts collected in 1995 and 2003. Eur J Prev Cardiol. 2014; 21:163–71.
Article17. Meurs M, Burger H, van Riezen J, Slaets JP, Rosmalen JG, van Melle JP, et al. The association between cardiac rehabilitation and mortality risk for myocardial infarction patients with and without depressive symptoms. J Affect Disord. 2015; 188:278–83.
Article18. Beauchamp A, Worcester M, Ng A, Murphy B, Tatoulis J, Grigg L, et al. Attendance at cardiac rehabilitation is associated with lower all-cause mortality after 14 years of follow-up. Heart. 2013; 99:620–5.19. Suaya JA, Stason WB, Ades PA, Normand SL, Shepard DS. Cardiac rehabilitation and survival in older coronary patients. J Am Coll Cardiol. 2009; 54:25–33.
Article20. Nielsen KM, Faergeman O, Foldspang A, Larsen ML. Cardiac rehabilitation: health characteristics and socio-economic status among those who do not attend. Eur J Public Health. 2008; 18:479–83.
Article21. Boulay P, Prud’homme D. Health-care consumption and recurrent myocardial infarction after 1 year of conventional treatment versus short- and long-term cardiac rehabilitation. Prev Med. 2004; 38:586–93.22. Santiago de Araujo Pio C, Marzolini S, Pakosh M, Grace SL. Effect of cardiac rehabilitation dose on mortality and morbidity: a systematic review and meta-regression analysis. Mayo Clin Proc. 2017; 92:1644–59.23. Mann DL, Zipes DP, Libby P, Bonow RO. Braunwald’s heart disease : a textbook of cardiovascular medicine. 10th ed. Philadelphia, PA: Elsevier/Saunders;2015.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correction: Do Cardiac Rehabilitation Affect Clinical Prognoses Such as Recurrence, Readmission, Revascularization, and Mortality After AMI?: Systematic Review and Meta-Analysis
- An Introduction of the Systematic Review and Meta-Analysis
- Critical Appraisal of Systematic Review/Meta-analysis
- Clinical Outcomes following Primary Hip Replacement Arthroplasties in Patients with Solid Organ Transplantation: A Systematic Review and Meta-Analysis
- Factors Related to Persistent Postoperative Pain after Cardiac Surgery: A Systematic Review and Meta-Analysis
