Which Approach Is Most Optimal for Needle Electromyographic Examination of the Biceps Femoris Short Head: Medial or Lateral?
- Affiliations
-
- 1Department of Dermatology, Korea University Ansan Hospital, Ansan, Korea
- 2Department of Anatomy, Korea University College of Medicine, Seoul, Korea
- 3Division of Brain Korea 21 Plus Program for Biomedical Science, Korea University College of Medicine, Seoul, Korea
- 4Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea
- 5Department of Laboratory Medicine, Korea University Anam Hospital, Seoul, Korea
- 6Department of Orthopedic Surgery, Korea University Ansan Hospital, Ansan, Korea
- 7Department of Physical Medicine and Rehabilitation, Korea University College of Medicine, Seoul, Korea
- KMID: 2513229
- DOI: http://doi.org/10.5535/arm.20092
Abstract
Objective
To investigate the anatomical characteristics of the biceps femoris short head (BS) and determine the optimal needle placement for BS examination.
Methods
Twenty-one lower limbs were dissected. The distances from the medial and lateral margins of the biceps femoris long head (BL) tendon to the common fibular nerve (CFN) (M_CFN_VD and L_CFN_VD, respectively) and the distance from the lateral margin of the BL tendon to the lateral margin of the BS (L_BS_HD) were measured 5 cm proximal to the tip of the fibular head (P1), four fingerbreadths proximal to the tip of the fibular head (P2), and at the upper apex of the popliteal fossa (P3).
Results
The BS was located lateral to the BL tendon. The CFN was located along the medial margin of the BL tendon. The median values were 2.0 (P1), 3.0 (P2), and 0 mm (P3) for M_CFN_VD; and 17.4 (P1), 20.2 (P2), and 21.8 mm (P3) for L_CFN_VD; and 8.1 (P1), 8.8 (P2), and 13.0 mm (P3) for L_BS_VD.
Conclusion
The lateral approach to the BL tendon was safer than the medial approach for examining the BS. Amore proximal insertion site around the upper apex of the popliteal fossa was more accurate than the distal insertion site. In this study, we propose a safer and more accurate approach for electromyography of the BS.
Figure
-
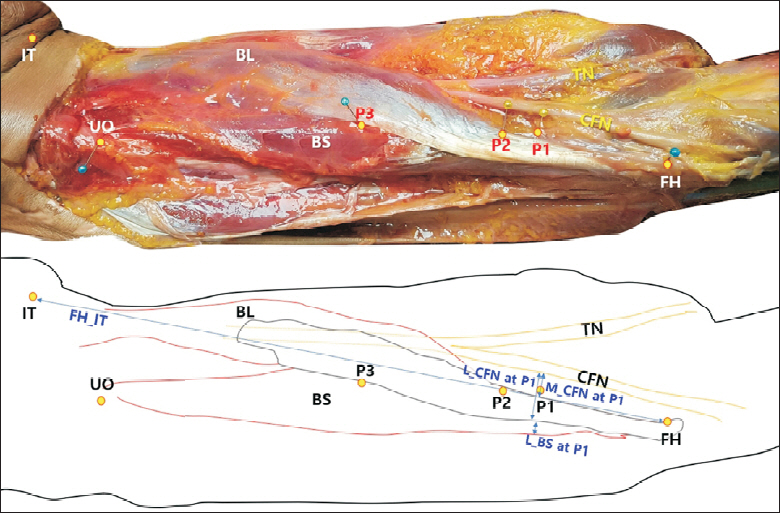
Fig. 1. Dissected cadaver indicating the anatomical marking sites and needle insertion levels according to the three commonly referred methods for electromyography of the biceps femoris short head muscle (BS). The common fibular nerve (CFN) divided from the sciatic nerve follows closely along the medial margin of the biceps femoris long head (BL) tendon. The BS is located laterally along the lateral margin of the BL tendon. TN, tibial nerve; IT, ischial tuberosity; UO, upper origin of the BS; FH, fibular head; P1, 5 cm proximal to the tip of the FH; P2, four fingerbreadths proximal to the FH (approximately 7 cm in this study); P3, the upper apex of the popliteal fossa.

Fig. 2. Box-and-whisker plots of the vertical distance from the lateral margin of the biceps femoris long head (BL) tendon to the lateral margin of the biceps femoris short head (BS) (L_BS_VD), and of the vertical distances from the lateral and medial margins of the BL tendon to the common fibular nerve (CFN) (L_CFN_VD and M_CFN_VD, respectively) at the P1, P2, and P3 levels in all cases (21 limbs). Distances were recorded as a negative value if the CFN was located lateral to the lateral or medial margin of the BL tendon, or if the lateral margin of the BS was located lateral to the lateral margin of the BL tendon. P1 level, 5 cm proximal to the tip of the fibular head; P2 level, 4 fingerbreadths proximal to the fibular head (approximately 7 cm in this study); P3 level, upper apex of the popliteal fossa.
Reference
-
1. Tubbs RS, Caycedo FJ, Oakes WJ, Salter EG. Descriptive anatomy of the insertion of the biceps femoris muscle. Clin Anat. 2006; 19:517–21.
Article2. Standring S. Gray’s anatomy: the anatomical basis of clinical practice. 40th ed. Edinburgh, UK: Churchill Livingstone;2008. p. 1377–8.3. Moore KL, Dalley AF, Agur AM. Clinically oriented anatomy. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2018. p. 731.4. Chu-Andrews J, Johnson RJ. Electrodiagnosis: an anatomical and clinical approach. Philadelphia, PA: Lippincott;1986. p. 179.5. Perotto AO, Delagi EF, Iazzetti J, Morrison D. Anatomical guide for the electromyographer: the limbs and trunk. 4th ed. Springfield, IL: Charles C Thomas;2005. p. 230–1.6. Lee HJ, DeLisa JA. Manual of nerve conduction study and surface anatomy for needle electromyography. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2005. p. 233.7. Haig AJ, Goodmurphy CW, Harris AR, Ruiz AP, Etemad J. The accuracy of needle placement in lower-limb muscles: a blinded study. Arch Phys Med Rehabil. 2003; 84:877–82.8. Goodmurphy C, Chiodo A, Haig A. The accuracy of needle placement in extremity muscles: a blinded study. J Clin Neurophysiol. 2007; 24:366–78.
Article9. Yun JS, Chung MJ, Kim HR, So JI, Park JE, Oh HM, et al. Accuracy of needle placement in cadavers: non-guided versus ultrasound-guided. Ann Rehabil Med. 2015; 39:163–9.
Article10. Delagi EF, Perotto A. Anatomic guide for the electromyographer. 2nd ed. Springfield, IL: Charles C Thomas;1980. p. 183–4.11. Geiringer SR. Anatomic localization for needle electromyography. Philadelphia, PA: Hanley & Belfus;1994. p. 122–3.12. Katirji B, Wilbourn AJ. High sciatic lesion mimicking peroneal neuropathy at the fibular head. J Neurol Sci. 1994; 121:172–5.
Article13. Stewart JD. Focal peripheral neuropathies. West Vancouver, Canada: JBJ Publishing;2010. p. 472–509.14. Esquenazi A, Alfaro A, Ayyoub Z, Charles D, Dashtipour K, Graham GD, et al. OnabotulinumtoxinA for lower limb spasticity: guidance from a Delphi panel approach. PM R. 2017; 9:960–8.
Article15. Kaymak B, Kara M, Tok F, Ulasli AM, Ozturk GT, Chang KV, et al. Sonographic guide for botulinum toxin injections of the lower limb: EUROMUSCULUS/USPRM spasticity approach. Eur J Phys Rehabil Med. 2018; 54:486–98.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transfer of the Medial Hamstring or Biceps Femoris to the Patella
- Anatomical Basis of Pronator Teres for Electromyography Needle Placement Using Ultrasonography
- Clinical importance of tensor fasciae suralis arising from linea aspera along with short head of biceps femoris: a rare anomaly
- Isolated Medial Dislocation of the Long Head of the Biceps without Rotator Cuff Tear: A Case Report
- Anomalous Biceps Femoris Tendon Insertion Leading to a Snapping Knee in a Young Male
