Wide-Awake Hand surgery
- Affiliations
-
- 1W Institute for Hand & Reconstructive Microsurgery, W General Hospital, Daegu, Korea
- KMID: 2513200
- DOI: http://doi.org/10.12790/ahm.20.0073
Abstract
- Wide-awake surgery is a surgical procedure which is not used a tourniquet and any sedation by using the function of lidocaine and epinephrine through the tumescent injection technique. The biggest advantages of wide-awake surgery are the prevention of the systemic risk of general anesthesia and the surgeon can confirm the result of surgery by moving the patient’s joint and tendon during the operation. But some modification of wide-awake surgery may be beneficial for the surgeon and patient. For decreasing the patient anxiety, low-grade sedative can be used and short-time use of tourniquet during initial dissection of the operating site can prevent the unexpected complication.
Keyword
Figure
-

Fig. 1. Prepare the 20 mL of 1% lidocaine mixed with the 0.2-mL 1:100,000 epinephrine (buffered at a ratio of 10 mL of lidocaine/epinephrine to 1 mL of 8.4% sodium bicarbonate). The 25–27 gauge needles are used during the injection.

Fig. 2. The usual amount of injection for the wide-awake local anesthesia at the hand volar side surgery.

Fig. 3. In case of long-lasting arterial constriction in the finger after injection, Phentolamine Mesylate (Reyon Pharm., Seoul, Korea; alpha-adrenergic blocking agent) can be injected around the ischemic area.

Fig. 4. (A, B) Wide-awake local anesthesia for a case with a complete zone II flexor tendon profundus cut in the small finger. Inject 2 mL of 1% lidocaine with 1:100,000 epinephrine (buffered at a ratio of 10 mL of lidocaine/epinephrine to 1 mL of 8.4% sodium bicarbonate) in subcutaneous fat. (C, D) Venting the A4 pulley enhances the motion of the flexor digitorum profundus tendon. (E, F)The range of motion of the small finger 8 months later. Written informed consent was obtained for publication of these images.
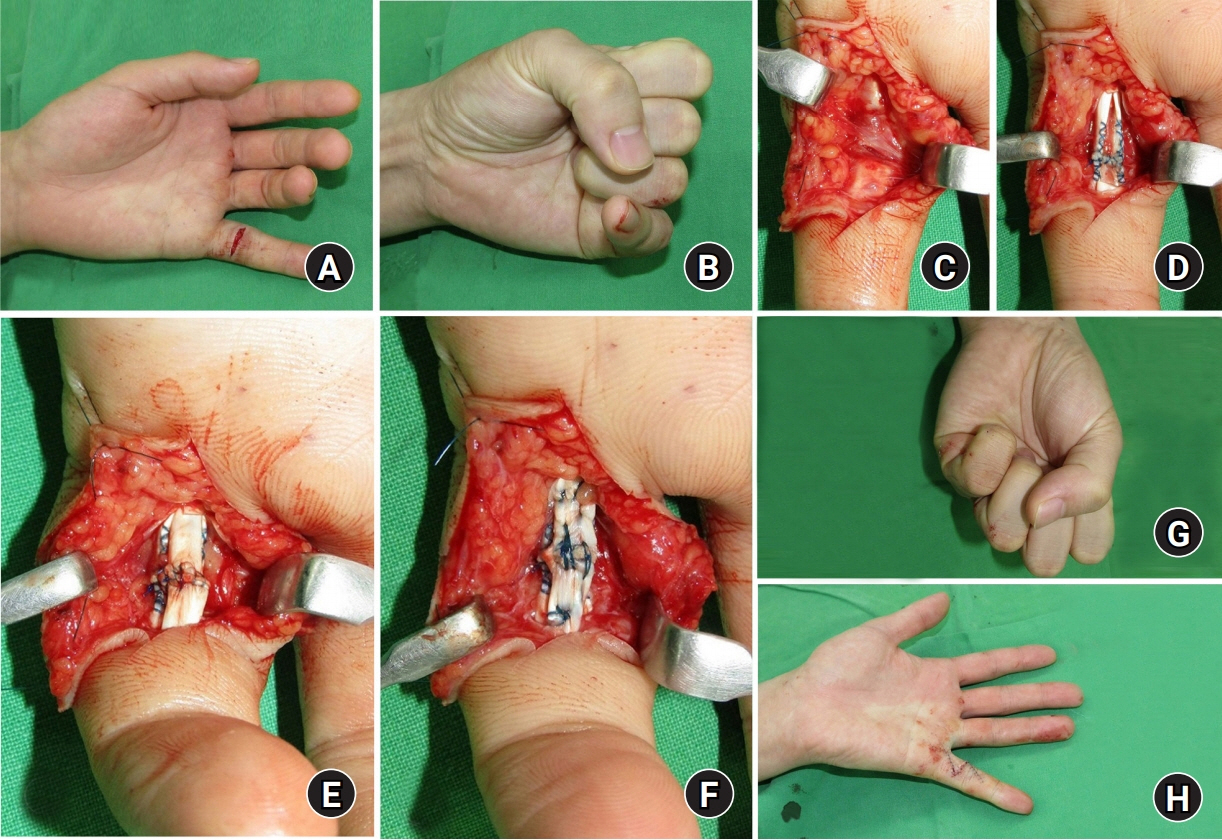
Fig. 5. (A, B) Preoperative view of rupture of the flexor tendons to the left small finger in a 28-year-old man. (C) Ruptured the sharp margin of the fifth flexor digitorum sublimis (FDS) and flexor digitorum profundus (FDP) tendon was shown at zone II. Simultaneous suturing of the ruptured FDS and FDP tendon at zone II increased the size of the two tendons. (D–F) Full release of A4 pulley and partial venting of A2 pulley will prevent the motion limitation of finger flexion. (G, H) Intraoperative views show full flexion and extension of small fingers after tendon repair. Written informed consent was obtained for publication of these images.
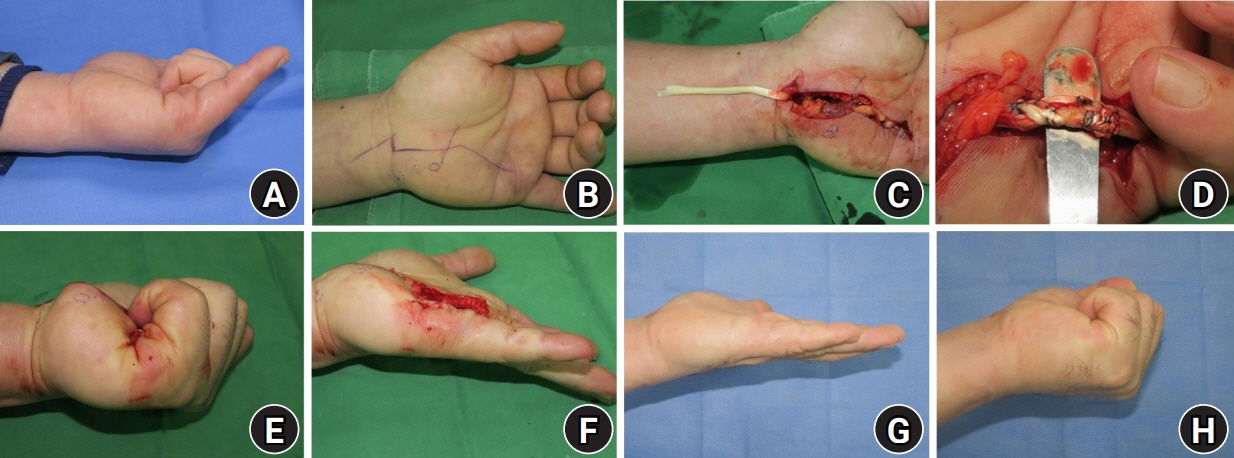
Fig. 6. (A, B) A 46-year-old man, a professional golf player, had been fractured hook of hamate and attritional rupture of both fifth flexor digitorum tendon at zone III. (C) With wide-awake anesthesia, the small profundus tendon was reconstructed with the ring finger superficialis tendon transfer. (D) Interweaving sutures are made fourth flexor digitorum sublimis to the fifth flexor digitorum profundus with adjusting tension. (E, F) Intraoperative assessment of the motion after tendon transfer. (G, H) The range of motion of the small finger 6 months later. Written informed consent was obtained for publication of these images.

Fig. 7. A 33-year-old man had extensor tendon subluxation by sagittal band rupture. (A) At the dorsum of metacarpophalangeal (MCP) joint, inject 10 mL of 1% lidocaine with 1:100,000 epinephrine (buffered at a ratio of 10 mL of lidocaine/epinephrine to 1 mL of 8.4% sodium bicarbonate) in subcutaneous fat. (B) Extensor tendon subluxation during MCP joint flexion. (C, D) The patient can regain the stability of the extensor tendon. Written informed consent was obtained for publication of these images.
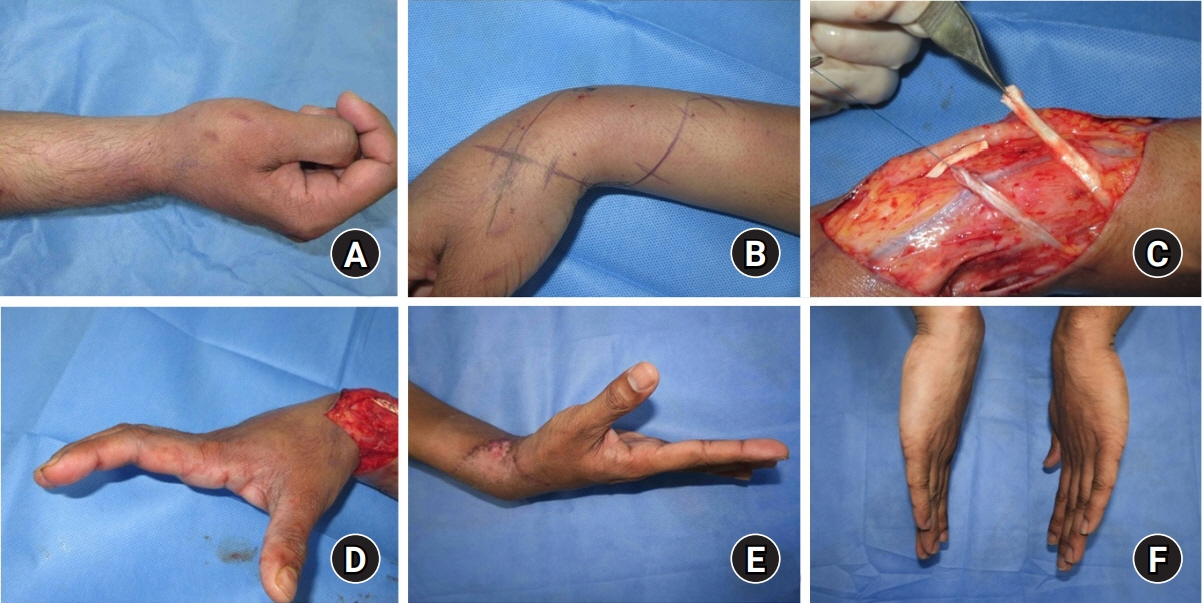
Fig. 8. (A) A 29-year-old man had lower radial nerve palsy of the right arm for 2 years. (B) Around one incision over the radio-dorsal wrist, 50 mL of 0.5% lidocaine with 1:200,000 epinephrine was used to decrease the total amount of injected epinephrine. (C) Skin incision and dissection of both the palmaris longus tendon and extensor pollicis longus tendon, and flexor carpi radialis and extensor digitorum communis are dissected under tourniquet. (D) Intraoperative assessment of the motion after tendon transfer. (E, F) Finger and thumb extension 6 months later. Written informed consent was obtained for publication of these images.

Fig. 9. (A) A 27-year-old man had previous fifth metacarpal fracture and limitation of metacarpophalangeal (MCP) joint flexion. (B) Severe adhesion of extensor tendon and was seen. (C) After tenolysis of extensor tenon, but no improvement of range of motion by MCP joint dorsal capsule thickening. (D) Immediate postoperative view. After dorsal capsulectomy, full flexion of the MP joint was possible. Written informed consent was obtained for publication of these images.
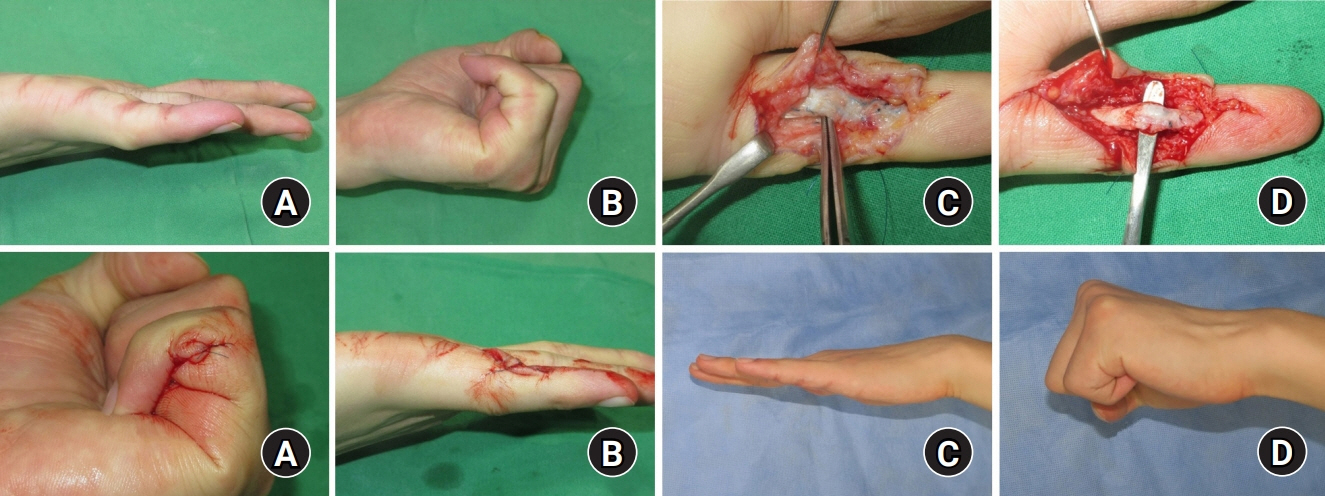
Fig. 10. (A, B) Flexion and extension contracture of the interphalangeal joints of the small finger after flexor tendon repair. (C) After opening the tendon sheath, the authors found severe adhesions between the flexor digitorum sublimis and flexor digitorum profundus (FDP) tendons as well as between flexor tendons and pulleys. (D) Tenolysis with FDP tendon. (E, F) Test of full digital extension and flexion during surgery. (H, I) Postoperative view 6 months later. Full flexion and extension were possible. Written informed consent was obtained for publication of these images.
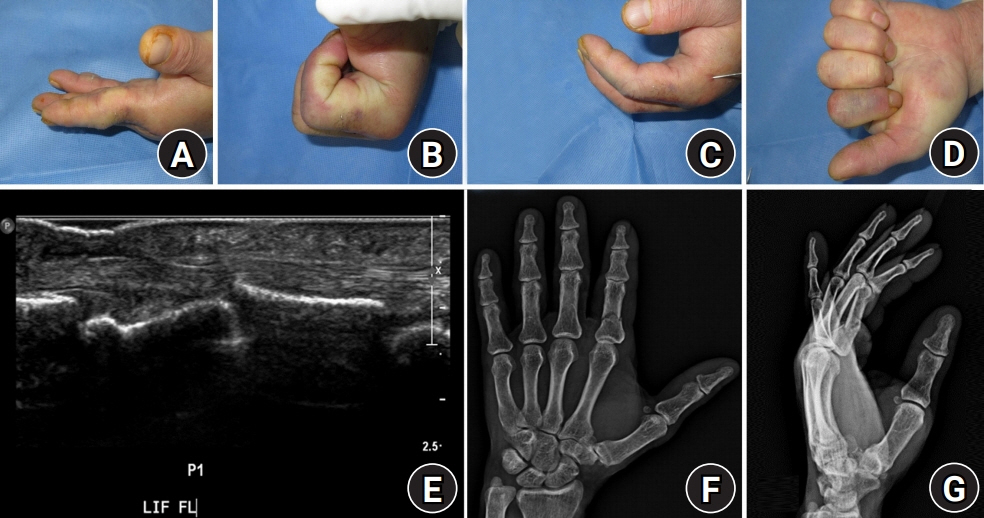
Fig. 11. A 55-year-old man underwent K-wire fixation for a closed proximal phalanx fracture of the index finger. (A–D) Intraoperative view of the index finger motion before and after fixation of K-wire. (E) Ultrasonogram showed catching of the flexor digitorum profundus tendon. (F, G) Preoperative radiographic findings. Written informed consent was obtained for publication of these images.
Reference
-
1. Lalonde D, Eaton C, Amadio P, Jupiter J. Wide-awake hand and wrist surgery: a new horizon in outpatient surgery. Instr Course Lect. 2015; 64:249–59.2. Lalonde D, Martin A. Epinephrine in local anesthesia in finger and hand surgery: the case for wide-awake anesthesia. J Am Acad Orthop Surg. 2013; 21:443–7.
Article3. Bezuhly M, Sparkes GL, Higgins A, Neumeister MW, Lalonde DH. Immediate thumb extension following extensor indicis proprius-to-extensor pollicis longus tendon transfer using the wide-awake approach. Plast Reconstr Surg. 2007; 119:1507–12.
Article4. Higgins A, Lalonde DH, Bell M, McKee D, Lalonde JF. Avoiding flexor tendon repair rupture with intraoperative total active movement examination. Plast Reconstr Surg. 2010; 126:941–5.
Article5. Khor WS, Langer MF, Wong R, Zhou R, Peck F, Wong JK. Improving outcomes in tendon repair: a critical look at the evidence for flexor tendon repair and rehabilitation. Plast Reconstr Surg. 2016; 138:1045e–1058e.6. Gregory S, Lalonde DH, Fung Leung LT. Minimally invasive finger fracture management: wide-awake closed reduction, K-wire fixation, and early protected movement. Hand Clin. 2014; 30:7–15.7. Hagert E, Lalonde DH. Wide-awake wrist arthroscopy and open TFCC repair. J Wrist Surg. 2012; 1:55–60.
Article8. Lalonde DH. Latest advances in wide awake hand surgery. Hand Clin. 2019; 35:1–6.
Article9. Wong J, Lin CH, Chang NJ, Chen HC, Lin YT, Hsu CC. Digital revascularization and replantation using the wide-awake hand surgery technique. J Hand Surg Eur Vol. 2017; 42:621–5.
Article10. MacNeill AL, Mayich DJ. Wide-awake foot and ankle surgery: a retrospective analysis. Foot Ankle Surg. 2017; 23:307–10.
Article11. Mackley CL, Marks JG Jr, Anderson BE. Delayed-type hypersensitivity to lidocaine. Arch Dermatol. 2003; 139:343–6.
Article12. Carazo JL, Morera BS, Colom LP, Gálvez Lozano JM. Allergic contact dermatitis from ethyl chloride and benzocaine. Dermatitis. 2009; 20:E13–5.13. Kennedy KS, Cave RH. Anaphylactic reaction to lidocaine. Arch Otolaryngol Head Neck Surg. 1986; 112:671–3.
Article14. Klein JA. Tumescent technique for regional anesthesia permits lidocaine doses of 35 mg/kg for liposuction. J Dermatol Surg Oncol. 1990; 16:248–63.
Article15. Strazar AR, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013; 132:675–84.
Article16. Kang SW, Kim YW, Park JK. Wide-awake hand surgery. Arch Hand Microsurg. 2018; 23:1–11.
Article17. Arendt-Nielsen L, Egekvist H, Bjerring P. Pain following controlled cutaneous insertion of needles with different diameters. Somatosens Mot Res. 2006; 23:37–43.
Article18. Farhangkhoee H, Lalonde J, Lalonde DH. Wide-awake trapeziectomy: video detailing local anesthetic injection and surgery. Hand (N Y). 2011; 6:466–7.
Article19. Frank SG, Lalonde DH. How acidic is the lidocaine we are injecting, and how much bicarbonate should we add? Can J Plast Surg. 2012; 20:71–3.
Article20. Chowdhry S, Seidenstricker L, Cooney DS, Hazani R, Wilhelmi BJ. Do not use epinephrine in digital blocks: myth or truth? Part II. A retrospective review of 1111 cases. Plast Reconstr Surg. 2010; 126:2031–4.
Article21. Thomson CJ, Lalonde DH, Denkler KA, Feicht AJ. A critical look at the evidence for and against elective epinephrine use in the finger. Plast Reconstr Surg. 2007; 119:260–6.
Article22. Zhang JX, Gray J, Lalonde DH, Carr N. Digital necrosis after lidocaine and epinephrine injection in the flexor tendon sheath without phentolamine rescue. J Hand Surg Am. 2017; 42:e119–23.
Article23. Nodwell T, Lalonde D. How long does it take phentolamine to reverse adrenaline-induced vasoconstriction in the finger and hand?: a prospective, randomized, blinded study: the Dalhousie project experimental phase. Can J Plast Surg. 2003; 11:187–90.
Article24. McKee DE, Lalonde DH, Thoma A, Glennie DL, Hayward JE. Optimal time delay between epinephrine injection and incision to minimize bleeding. Plast Reconstr Surg. 2013; 131:811–4.
Article25. Tang JB. Wide-awake primary flexor tendon repair, tenolysis, and tendon transfer. Clin Orthop Surg. 2015; 7:275–81.
Article26. Gao LL, Chang J. Wide awake secondary tendon reconstruction. Hand Clin. 2019; 35:35–41.
Article27. Lalonde DH. Wide-awake extensor indicis proprius to extensor pollicis longus tendon transfer. J Hand Surg Am. 2014; 39:2297–9.
Article28. Woo SH, Yoo MJ, Ahn HC. Lessons learned in the authors’ first years of wide-awake hand surgery at the W hospital in Korea. Hand Clin. 2019; 35:59–66.
Article29. Diao E, Eaton RG. Total collateral ligament excision for contractures of the proximal interphalangeal joint. J Hand Surg Am. 1993; 18:395–402.
Article30. Das De S, Vranceanu AM, Ring DC. Contribution of kinesophobia and catastrophic thinking to upper-extremity-specific disability. J Bone Joint Surg Am. 2013; 95:76–81.31. Lied L, Borchgrevink GE, Finsen V. Wide awake hand surgery. J Hand Surg Asian Pac Vol. 2017; 22:292–6.
Article32. Teo I, Lam W, Muthayya P, Steele K, Alexander S, Miller G. Patients’ perspective of wide-awake hand surgery: 100 consecutive cases. J Hand Surg Eur Vol. 2013; 38:992–9.33. Odinsson A, Finsen V. The position of the tourniquet on the upper limb. J Bone Joint Surg Br. 2002; 84:202–4.
Article34. Nakanishi Y, Omokawa S, Kobata Y, et al. Ultrasound-guided selective sensory nerve block for wide-awake forearm tendon reconstruction. Plast Reconstr Surg Glob Open. 2015; 3:e392.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Wide-Awake Hand Surgery
- Tumescent Local Anesthesia for Hand Surgery: Improved Results, Cost Effectiveness, and Wide-Awake Patient Satisfaction
- Wide Awake Hand Surgery
- Wide Awake Local Anesthesia No Tourniquet Technique for Extensor Indicis Proprius Tendon Transfer
- Anesthetic considerations for awake craniotomy
