Wide-Awake Hand Surgery
- Affiliations
-
- 1Department of Orthopaedic Surgery, Chungbuk National University Hospital, Cheongju, Korea. carm0916@hanmail.net
- 2Department of Hand and Micro Reconstructive Surgery, Institute for Hand and Reconstructive Microsurgery, W Hospital, Daegu, Korea.
- KMID: 2412485
- DOI: http://doi.org/10.12790/ahm.2018.23.1.1
Abstract
- Wide-awake hand surgery is a surgical procedure that does not use a tourniquet and sedation through lidocaine and epinephrine injections and does not perform regional anesthesia or general anesthesia. Therefore, systemic risk by general anesthesia can be avoided, and more accurate surgeries can be performed through active joint motion during surgery without discomfort due to tourniquet used during local anesthesia. Also, the time and cost associated with anesthesia can be reduced and the hospital day can be reduced by performing the day surgery. The authors will introduce the concept of the wide-awake hand surgery and discuss the indications, drug usage, and injection methods.
Keyword
MeSH Terms
Figure
-

Fig. 1 Phentolamine Mesylate (Reyon Pharm., Seoul, Korea) is an alpha-adrenergic blocking agent that rescue for epinephrine vasoconstriction in the finger.
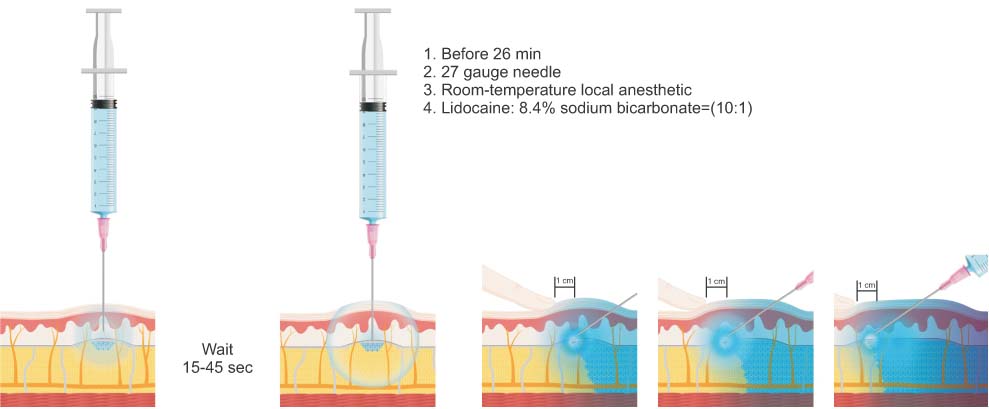
Fig. 2 Illustration for the reduction of injection-associated pain. Adapted from the article of Strazar et al.16 (Plast Reconstr Surg. 2013;132:675–84) with original copyright holder's permission.

Fig. 3 A simple technique to decrease movement during injection is to stabilize the syringe holding hand with fingers, and too much local anesthetic is better than not enough.
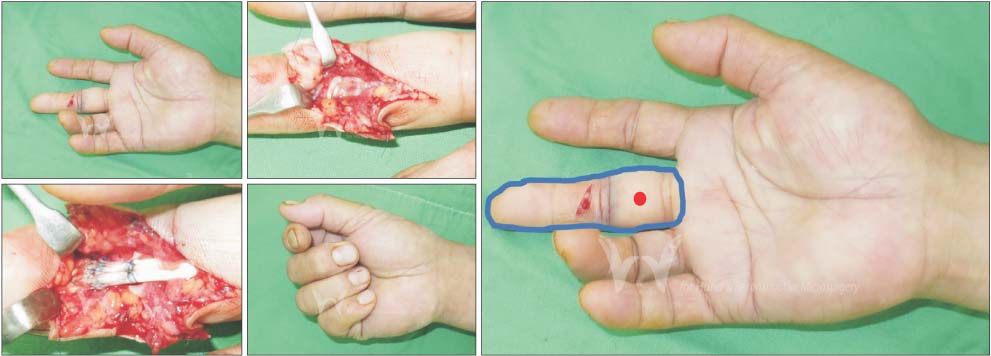
Fig. 4 Wide-awake local anesthesia for a case with a complete zone 2 flexor tendon cut in the middle finger. Inject 2 mL of 1% lidocaine with 1:100,000 epinephrine (buffered at a ratio of 10 mL of lidocaine/epinephrine to 1 mL of 8.4% sodium bicarbonate) in subcutaneous fat in the red injection point just under the skin.
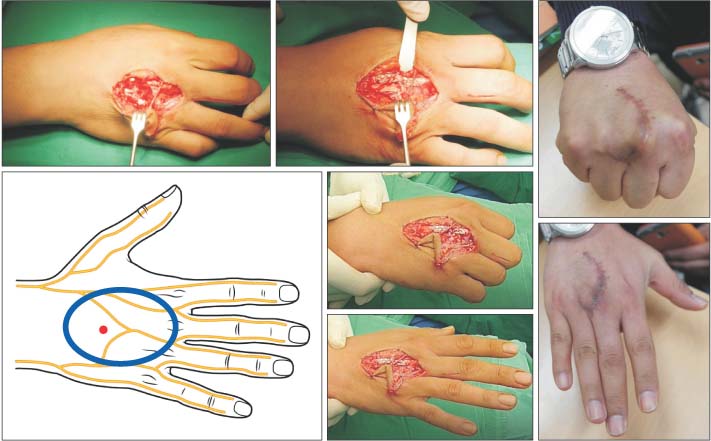
Fig. 5 Wide-awake local anesthesia for a case with a complete zone 5 extensor tendon cut in the hand. Inject 20 mL of 1% lidocaine with 1:100,000 epinephrine buffered with 2 mL of 8.4% sodium bicarbonate in subcutaneous fat in the red injection point just under the skin.
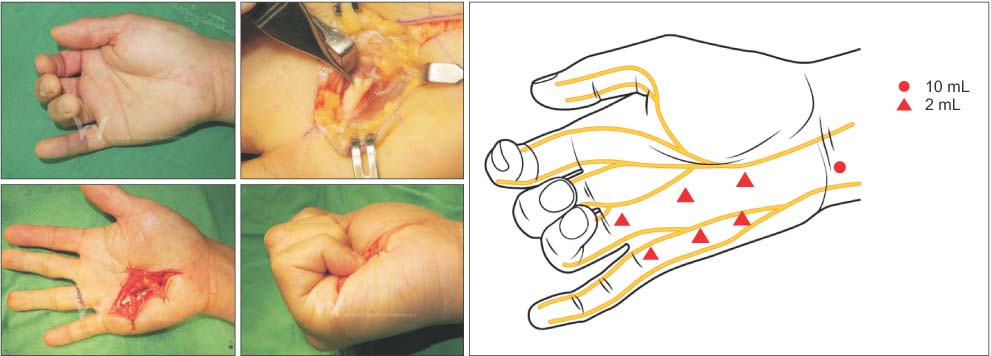
Fig. 6 Wide-awake local anesthesia for a case with a spontaneous ruptured both flexors of the small finger. The small profundus was reconstructed with a tendon transfer to the ring finger superficialis tendon.

Fig. 7 Extensor indicis proprius to extensor pollicis longus tendon transfer with the wide awake approach. (A) Inject 20 mL of 1% lidocaine with 1:100,000 epinephrine buffered with 2 mL of 8.4% bicarbonate, starting 3 cm proximal to the Lister's tubercle. (B) Exposure of the ruptured EPL tendon (C) after the tendon transfer, (D, E) intraoperative testing of thumb flexion and extension. (F, G) At three months postoperatively, the range of motion of the thumb was fully recovered.

Fig. 8 Tendon transfer for rupture of the extensors to the long, ring and small finger with the wide awake approach.

Fig. 9 A 23-year-old man who had a stiff finger by prior metacarpal fracture surgery. (A, B) The metacarpophalangeal (MCP) extension contracture. (C-F) The patient can regain functional motion of the MCP joint after wide-awake surgical release.
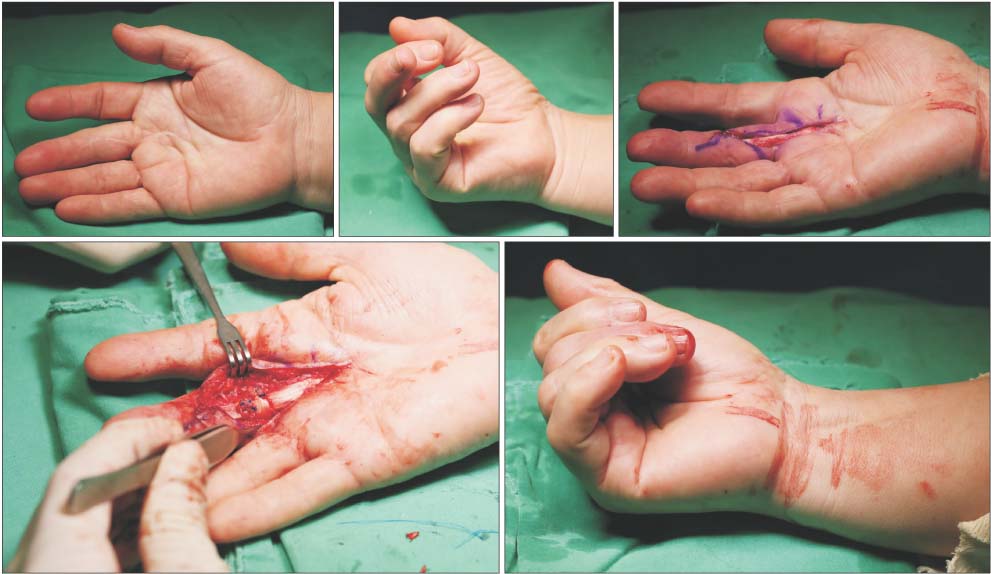
Fig. 10 Tenolysis and pulley reconstruction in a 58-year-old woman who had been unable to flex her long finger.

Fig. 11 A 55-year-old man underwent plate fixation for an open metacarpal fracture. Inject a total of 30 to 40 mL of 1% lidocaine with 1:100,000 epinephrine (buffered with 10 mL lidocaine/epinephrine:1 mL of 8.4% sodium bicarbonate).

Fig. 12 The rotation was assessed from an active range of motion of the metacarpophalangeal joints during the surgery.

Fig. 13 (A, B) A 34-year-old man who sustained scissoring of the small finger after minimally displaced metacarpal fracture. (C, D) The malrotation was corrected with the wide awake approach.

Fig. 14 For carpal tunnel release, inject 10 mL of buffered 1% lidocaine with 1:100,000 epinephrine just ulnar to the palmaris longus at the proximal injection point. After the initial 10 mL, come back to the subcutaneous plane with the needle tip and slowly infiltrate 10 mL from proximal to distal in an antegrade direction down the palm between the skin and the superficial palmar fascia.
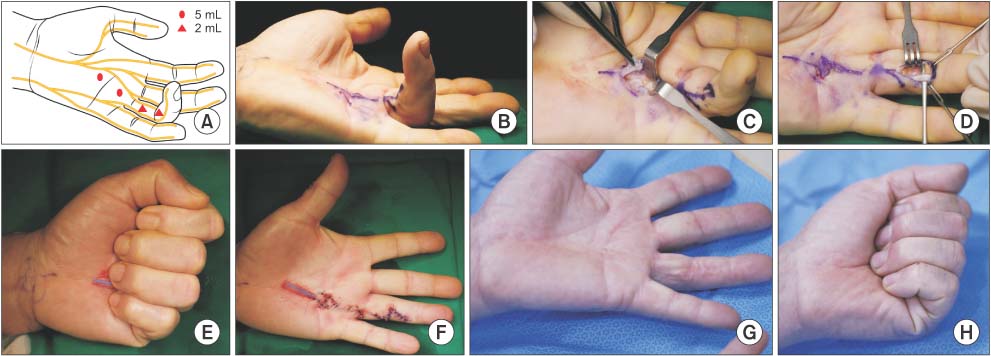
Fig. 15 The wide-awake approach to Dupuytren's contracture. (A, B) Inject to 14 mL of 1% lidocaine with 1:100,000 epinephrine. (C-F) Verifying active extension with active movement after cord resection. (G, H) At 3 years follow-up, the patient achieved optimal functional outcomes with a good range of motion.
Cited by 1 articles
-
Wide-Awake Hand surgery
Young Woo Kim
Arch Hand Microsurg. 2021;26(1):1-11. doi: 10.12790/ahm.20.0073.
Reference
-
1. Edwards SA, Harper GD, Giddins GE. Efficacy of forearm versus upper arm tourniquet for local anaesthetic surgery of the hand. J Hand Surg Br. 2000; 25:573–574.
Article2. Prodhomme G, Mouraux D, Dugailly PM, Chantelot C, Fontaine C, Schuind F. Tolerance of upper extremity pneumatic tourniquets and their effect on grip strength. J Hand Surg Eur Vol. 2008; 33:266–271.3. Ogufere WE, Giddins GE, Thom JS. Upper arm tourniquet pain in local anaesthetic surgery. J Hand Surg Br. 1995; 20:413–414.
Article4. Lalonde D, Bell M, Benoit P, Sparkes G, Denkler K, Chang P. A multicenter prospective study of 3,110 consecutive cases of elective epinephrine use in the fingers and hand: the Dalhousie Project clinical phase. J Hand Surg Am. 2005; 30:1061–1067.
Article5. Chowdhry S, Seidenstricker L, Cooney DS, Hazani R, Wilhelmi BJ. Do not use epinephrine in digital blocks: myth or truth? Part II. A retrospective review of 1111 cases. Plast Reconstr Surg. 2010; 126:2031–2034.
Article6. Thomson CJ, Lalonde DH, Denkler KA, Feicht AJ. A critical look at the evidence for and against elective epinephrine use in the finger. Plast Reconstr Surg. 2007; 119:260–266.
Article7. Nodwell T, Lalonde D. How long does it take phentolamine to reverse adrenaline-induced vasoconstriction in the finger and hand? A prospective, randomized, blinded study: the Dalhousie project experimental phase. Can J Plast Surg. 2003; 11:187–190.
Article8. Fitzcharles-Bowe C, Denkler K, Lalonde D. Finger injection with high-dose (1:1,000) epinephrine: Does it cause finger necrosis and should it be treated? Hand (N Y). 2007; 2:5–11.
Article9. Zhang JX, Gray J, Lalonde DH, Carr N. Digital necrosis after lidocaine and epinephrine injection in the flexor tendon sheath without phentolamine rescue. J Hand Surg Am. 2017; 42:e119–e123.
Article10. Klein JA. Tumescent technique for regional anesthesia permits lidocaine doses of 35 mg/kg for liposuction. J Dermatol Surg Oncol. 1990; 16:248–263.
Article11. Burk RW 3rd, Guzman-Stein G, Vasconez LO. Lidocaine and epinephrine levels in tumescent technique liposuction. Plast Reconstr Surg. 1996; 97:1379–1384.
Article12. Lalonde DH. Wide awake hand Surgery. Boca Raton: CRC press;2015. p. 29–47.13. McKee DE, Lalonde DH, Thoma A, Glennie DL, Hayward JE. Optimal time delay between epinephrine injection and incision to minimize bleeding. Plast Reconstr Surg. 2013; 131:811–814.
Article14. Frank SG, Lalonde DH. How acidic is the lidocaine we are injecting, and how much bicarbonate should we add? Can J Plast Surg. 2012; 20:71–73.
Article15. Hogan ME, vanderVaart S, Perampaladas K, Machado M, Einarson TR, Taddio A. Systematic review and meta-analysis of the effect of warming local anesthetics on injection pain. Ann Emerg Med. 2011; 58:86–98.
Article16. Strazar AR, Leynes PG, Lalonde DH. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013; 132:675–684.
Article17. Jung SW, Kim CK, Ahn BW, Kim DH, Kang SH, Kang SS. Standard versus over-tensioning in the transfer of extensor indicis proprius to extensor pollicis longus for chronic rupture of the thumb extensor. J Plast Reconstr Aesthet Surg. 2014; 67:979–985.
Article18. Bezuhly M, Sparkes GL, Higgins A, Neumeister MW, Lalonde DH. Immediate thumb extension following extensor indicis proprius-to-extensor pollicis longus tendon transfer using the wide-awake approach. Plast Reconstr Surg. 2007; 119:1507–1512.
Article19. Hagert E, Lalonde DH. Wide-awake wrist arthroscopy and open TFCC repair. J Wrist Surg. 2012; 1:55–60.
Article20. Nakanishi Y, Omokawa S, Kobata Y, et al. Ultrasound-guided selective sensory nerve block for wide-awake forearm tendon reconstruction. Plast Reconstr Surg Glob Open. 2015; 3:e392.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Wide-Awake Hand surgery
- Tumescent Local Anesthesia for Hand Surgery: Improved Results, Cost Effectiveness, and Wide-Awake Patient Satisfaction
- Wide Awake Hand Surgery
- Wide Awake Local Anesthesia No Tourniquet Technique for Extensor Indicis Proprius Tendon Transfer
- Anesthetic considerations for awake craniotomy
